
Submitted:
11 December 2025
Posted:
12 December 2025
You are already at the latest version
Abstract
External causes of death contribute to over four million annual global fatalities, with drug use representing a significant risk factor. However, the true national impact and regional variations of psychoactive substance use in these deaths remains unde-fined in Brazil. To address this critical knowledge gap, this pioneering four-region study sought to elucidate the influence of alcohol and drug use on external cause mor-tality. We collected post-mortem blood from 3,577 victims of violent death across four distinct Brazilian regions using a standardized protocol to identify alcohol, illicit drugs, and psychoactive medicines. Analysis revealed a predominantly male cohort (89.7%; 56.0% aged 30 years or more), with homicide as the primary manner of death (67.3%). Critically, over half of the victims (53.0%) were positive for at least one psy-choactive substance prior to death, most commonly cocaine (29.6%) and alcohol (27.7%). Substance consumption was highest among homicide victims (55.7%), pre-dominantly cocaine (36.0%), and in self-harm cases (26.4%), which showed high ben-zodiazepine rates (20.0%). Consumption patterns varied regionally: alcohol-related deaths were more common in the Northeast, drug-only deaths concentrated in the Southeast and North, and the South showed a higher prevalence of alcohol use versus drug use. This widespread, regionally heterogeneous prevalence underscores the ur-gent need for targeted, region-specific interventions. By critically linking psychoactive substance use to various modes of violent death, these data provide crucial forensic and public health insights to inform tailored preventive strategies.
Keywords:
post-mortem
; violent deaths
; illicit drugs
; homicides
1. Introduction
External causes of mortality refer to all circumstances of unnatural deaths—that is, deaths not involving diseases or pathological conditions—as defined in chapter 23 of the 11th revision of the International Classification of Diseases (ICD-11). These deaths typically result from injuries caused by external agents, which the World Health Organization (WHO) classifies into categories: unintentional (accidental), intentional, interpersonal, self-inflicted, legal intervention, war, civil unrest, and undetermined intent [1] and are typically addressed as violent deaths.
In 2021, external causes accounted for over 4.4 million deaths globally, with traffic crashes leading at more than 1.1 million fatalities [1]. In Brazil, these causes resulted in 158,250 deaths in 2024, ranking fourth after circulatory system diseases, neoplasms, and respiratory diseases. Mortality rates from external causes have remained relatively stable from 2012 to 2023, with approximately 75 deaths per 100,000 inhabitants in the latest year [2] (DATASUS, 2024). According to the Pan American Health Organization (PAHO, 2021), traffic crashes combined with interpersonal violence prematurely cost Brazil 2,649.1 years of life and accounted for a loss of 91.9 Disability-Adjusted Life Years (DALYs) [3].
External causes remain a major public health concern in Brazil, with an age-adjusted mortality rate of approximately 70.8 per 100,000 population in 2023, reflecting significant losses due to homicides (31.6/100,000), traffic crashes (15.1/100,000), and suicides (6.4/100,000) (WHO, 2024). Mortality disproportionately affects men and young adults, while regional disparities show higher risks in the North, Northeast, and Central-West regions [2]. These deaths not only cause premature mortality but also contribute substantially to the nation’s economic and social burden
Multiple complex factors influence injury occurrence from external causes, often making their elucidation challenging. Alcohol and drug use stand out as significant risk factors for such injuries and deaths. Goldstein (1985) proposed a triadic framework to understand the violence-drug nexus: psychopharmacological effects of substances (e.g., alcohol, cocaine, stimulants) that may provoke violent behavior; economic-compulsive motives driven by drug-seeking; and systemic factors related to the illegal drug market, which primarily victimizes users. These systemic factors stem from the illicit nature of drugs, rendering violence endemic to their context [4].
Victimization from external causes may also be linked to drug consumption, since the use of psychoactive substances (PSA) impairs cognitive and motor functions, potentially leading to involvement in accidents or acts that put the physical safety of the user or others at risk. These effects are generally associated with the pharmacological classes of the PSAs (stimulants, depressants, or central nervous system—CNS—disturbing agents) and the dose consumed [5].
Brazil’s vast territorial extent comprises diverse social, economic, cultural, and health landscapes, leading to regional variations in psychoactive substance use patterns and their impact on deaths from external causes. Regional differences also affect drug availability and pricing, influencing consumer profiles [6]. Despite the significance of substance use in external cause mortality, Brazil lacks nationwide studies correlating psychoactive substance consumption with deaths from traffic crashes, homicides, and suicides. Amid varying consumption patterns and drug availability across Brazil, a nationwide study correlating psychoactive substance use to these violent deaths remains crucial but methodologically challenging. This study aims to fill this knowledge gap by pioneering a comprehensive assessment across four macro-regions.
2. Materials and Methods
2.1. Study Design and Sample Collection
External causes deceased victims were included in a cross-sectional study among four Brazilian regions. In each geographical region, one state capital was selected as target based upon mortality rate and for being located along drug trafficking routes. Belém/PA, Recife/PE, Vitória/ES and Curitiba/PR were involved in sample collection representing the North, Northeast, Southeast and South regions respectively. In addition to the capital cities, satellite cities from each metropolitan region were also included. The selected cities exhibit significant differences in cultural, economic, social, and sanitary aspects, with human development indices (HDI) comparable to those of different countries, such as Tunisia (0.746), South Africa (0.741), Qatar (0.886), and Portugal (0.890) (Table 1). Sampling occurred during autopsies at the Institutes of Legal Medicine (ILM), that are official public forensic institutions responsible for autopsies in criminal cases.
A representative sample of all violent death cases in each city was achieved by adopting a probabilistic sampling strategy [7]. All days and hours were included proportionally, allowing a population-based sample from each city to be achieved. Sample collection occurred in the four cities simultaneously and continuously from March 2022 to June 2024. All victims older than 18 years who were autopsied within eight hours of death were included. Decomposed corpses and victims who received six or more hours of medical treatment were excluded.
Data from the victim (age and sex) and information about the fatal injuries (i.e. day, time, cause and manner of death) were obtained from police records. Only closed cases with definitively determined causes of death were included.
2.2. Toxicological Analysis
Cardiac blood samples were collected during autopsies, using vacuum tubes containing sodium fluoride and ethylenediamine tetraacetic acid (EDTA) and stored at -20ºC until transportation to the Toxicology Laboratory at the University of Sao Paulo Medical School. In cases where the cardiac chamber was not intact and sample risked contamination with stomach contents or other biological fluids or if there was insufficient blood available due to the extent of the injuries, peripheral (femoral) blood was collected.
All blood samples were analyzed at the Toxicological Laboratory from the University of Sao Paulo Medical School in Sao Paulo. Blood Alcohol Concentration – BAC was analyzed by headspace gas chromatography with flame ionization detector (HS-GC-FID) whilst drugs were detected by liquid chromatography with tandem mass spectrometry (LC-MS/MS). All analyzed substances and their respective cut-offs are presented in Table 2. Analytes were chosen given its importance at a Brazilian setting. Benzoylecgonine, major cocaine metabolite, was used to identify cocaine consumption.
Substance use was categorized into five groups (1) Any alcohol presence - detection of alcohol (2) at least one substance - confirmed positivity for alcohol and/or other drugs (3) only alcohol - positive BAC but negative for all other drugs (4) only other drugs - negative BAC but positive for at least one other drug (5) two or more substances - positive for at least two different substances (which may include alcohol).
Additionally, proportions for alcohol-positive cases and drug-positive cases are reported, along with other combinations. These proportions indicate positivity for each respective group of substances and do not mutually exclude the concurrent use of other substances.
2.3. Geospatial Analysis
A geospatial analysis based on the macro region within the state capital was conducted to study the influence of alcohol and other drug use according to the place of the fatal injury. Death densities were calculated for each of the 4 macro regions based on the population rate for 2021 (per 100,000 population).
A map of Brazil divided into all states was used to input data on death densities by states according to drug and alcohol use positivity. A color gradient was used to illustrate death density rates across all four included states, with darker tones representing higher densities than lighter ones. The grouping of density rates across maps was reached using a Jerks algorithm, which makes an approximation of the intervals to the closest possible value of the median for each rate reported. MapInfo Professional software, version 10.0 was used.
Additionally, a ratio was created between mean death densities obtained for drug and alcohol positivity (ρ drug positivity / ρ alcohol positivity) grouped according to the four Brazilian regions involved in the study (North, Northeast, Southeast and South). A region with a “drug problem ratio” (DPR) greater than 1 indicates a higher density of drug positivity compared to alcohol, whereas rate values less than 1 indicate the opposite. DPR I is based on any results of alcohol and drugs, whereas DPR II considers findings of alcohol alone and drugs alone.
2.4. Statistical Analysis
Absolute and relative frequencies (%) are presented for categorical variables. Associations between categorical variables were analyzed using bivariate cross-tabulation and Pearson’s chi-square test. Crude odds ratios (ORs) and adjusted odds ratios (aORs), adjusting for sex, alcohol, cocaine, cannabis, and benzodiazepines use, were calculated using multivariable logistic regression. Variables for each logistic regression model were selected based upon statistical significance derived from Pearson’s chi-square test. Significance levels were set at p < 0.05. All analyses were conducted using STATA statistical software, version 16.1 (College Station, Texas, USA).
3. Results
A total of 3,577 victims were included. The vast majority were males (89.7%), aged 30 years or older (56.0%), and non-white (80.8%). Homicides were the main manner of death (67.3%), followed by traffic crashes (14.7%) and suicides (9.2%). More than half of the victims (53.0%) had consumed at least one substance before death, with cocaine being the most common (29.6%), followed by alcohol (27.7%), benzodiazepines (6.8%), and cannabis (2.2%). Homicide victims had the highest prevalence of alcohol/drug use (55.7%; 95% CI: 53.7-57.7), mainly cocaine use (36.0%; 95% CI: 34.1-38.0). Self-harm victims had the second-highest prevalence of substance use, with alcohol being the main substance (29.4%; 95% CI: 24.7-34.6). Those victims also presented very high rates of benzodiazepine consumption; one-fifth of the sample tested positive in toxicological analysis. While more than two in five traffic-related victims had consumed substances, this was driven especially by alcohol (38%; 95% CI: 33.9-42.2) (Table 3).
Men were more likely to have consumed substances (OR = 1.52; 95% CI: 1.24-1.89), specially drugs (OR=1.92; 95%CI: 1.42-2.61) or a combination of substances. Young victims (less than 30 years old) consumed more drugs (OR=1.89; 95% CI: 1.59-2.22) while those aged 30 or more were more likely to have consumed alcohol alone (OR = 1.94; 95% CI: 1.59-2.36). Alcohol alone was strongly associated with traffic-related deaths, drug use associated with homicides and combination of substances with homicides and suicides. Alcohol use was associated with deaths occurring at nighttime and at weekends, used alone or in combination with other substances (Table 4).
The consumption of substances across Brazilian states was uneven. Deaths involving alcohol, either solely or in combination with drugs, were more prevalent in the Northeast region, while deaths involving only drugs were concentrated in the Southeast and North regions (Figure 1). The calculated DPR further confirmed the prominence of drug-related deaths in these regions. In contrast, the South region exhibited a higher prevalence of alcohol-related deaths compared to drug-related deaths, whereas the Northeast region showed a more similar distribution between alcohol and drug-related deaths (Table 5).
4. Discussion
The present study represents the first investigation among four Brazilian regions to comprehensively examine the association between psychoactive substance use and violent deaths across multiple geographic regions. The finding that over half of violent death victims (53.0%) tested positive for at least one psychoactive substance prior to death underscores the substantial role of substance use in premature mortality from external causes in Brazil. Overall, our findings align with international [8,9,10] and national [7,11,12] findings regarding postmortem toxicological analysis, while also revealing important regional and substance-specific patterns. Internationally, patterns of substance use vary by region; for example, in Cape Town, South Africa, 61% of assessed victims had consumed drugs, with methamphetamine, methaqualone, and diphenhydramine being the most prevalent [8]. In New South Wales, Australia, among homicide victims, 32.8% tested positive for illicit drugs, with cannabis (21.4%) and opioids (11.2%) being the most common [9]. By contrast, in Milan, Italy, cocaine was the most frequently used substance (27.9%) among postmortem cases, a pattern more closely aligned with our findings [10].
A previous Brazilian study found considerably higher figures for cocaine and cannabis use among homicide victims, 72.2% and 67.7%, respectively. However, in that study toxicological analyses were performed in a non-systematic way, restricted to victims in whom there was already some suspicion of drug use [12], which likely led to an overestimation of drug positivity when compared with the population-based and standardized approach used here.
The demographic characteristics of the victims in our study support the evidence that men are more likely not only to use alcohol and other drugs, but also to be involved in injurious events that result in fatal outcomes [13]. Moreover, given the significant association between exclusive drug use and victims under 30 years of age, there is a clear need to identify and intervene on problematic drug use in youth, since such behaviors can lead both to the perpetration of violence and to victimization [14].
Although cannabis is the most widely used drug in Brazil and its consumption has increased in the last decade [15], its prevalence in the present study was lower than expected, given that another investigation using the same general study design found a higher percentage of cannabis use (14.0%) among victims of violent deaths in the city of São Paulo [7]. A direct relationship between cannabis use and violence is not firmly established in the scientific literature, and there is ongoing debate about the magnitude of the association between the psychopharmacological effects of cannabis and the occurrence of injuries and deaths. Available data indicate that there may be a moderate increase in the probability of violence among cannabis users, a relationship that seems more evident among those with daily use and some degree of psychosis [16]. The pharmacological effects of cannabis include an altered state of consciousness and changes in time perception; at moderate concentrations, some studies suggest a temporary inhibition of violent behaviors [17]. Our results therefore do not suggest an absence of cannabis use in the population, but rather a low frequency of THC detection among victims of external causes in the studied cities, which may reflect a weaker epidemiological link.
Cocaine, in contrast, emerged as the most frequently detected illicit drug in our sample, particularly among homicide victims. This pattern is consistent with Brazil’s role as both a transit corridor and the biggest consumer market for cocaine in South America and with previous studies that identified strong associations between cocaine use, criminal activity, and violent victimization [18]. However, the present study is cross-sectional and cannot establish causality between cocaine use and homicide, and the observed associations should be interpreted in light of psychopharmacological effects, economic-compulsive motives, and systemic violence related to the illegal drug market rather than acute intoxication alone. Even though, the consumption of cocaine has already been associated with increased criminality activities such as robberies [19].
Although alcohol has been regulated in road traffic in Brazil since 1998, it remains the main contributor to traffic crashes. Alcohol is a central nervous system depressant that reduces visual acuity, alertness, and motor and cognitive coordination, all of which are essential abilities for driving [20]. Even at low concentrations, alcohol causes impairments in users, and there is no safe level for driving, since there is a dose–response relationship with an exponential increase in the risk of involvement in traffic crashes [21]. In legal terms, Brazil has one of the strictest frameworks in the world, adopting a zero-tolerance policy for alcohol in drivers. Despite this, alcohol continues to be detected as the main substance among individuals injured [22] and killed [7,23,24] in traffic crashes, and our multicenter postmortem data confirm that alcohol remains the primary substance associated with traffic-related deaths. Enforcement of alcohol and other drug use among drivers is one of the most effective ways to reduce consumption of these substances by drivers and, consequently, to reduce deaths resulting from alcohol use. On the other hand, under current Brazilian law drivers may refuse to undergo breathalyzer testing, which, even with administrative sanctions (loss of driver’s license and fines), results in a certain degree of impunity for offenders [25]. Thus, to translate Brazil’s strict legal framework into greater population impact, it will be necessary to strengthen random testing and police enforcement, reduce the incentive to refuse testing, and integrate roadside enforcement with broader alcohol-control policies.
Regarding the geospatial analysis of alcohol and drug use, the cities located in the North (Belém, PA) and Southeast (Vitória, ES) regions showed the highest drug problem ratio coefficients, indicating greater drug use compared with alcohol. In our study, the drug problem ratio reflected the relationship between death densities with drug positivity and those with alcohol positivity, thereby summarizing whether a region is more “drug-dominant” or “alcohol-dominant” in terms of substance involvement in violent deaths. Belém lies within the Amazon region and has several river branches used to transport cocaine from neighboring countries such as Peru and Colombia, which may partly explain the higher drug consumption relative to alcohol in this area [26]. By contrast, the cities in the Northeast and South regions (Recife, PE, and Curitiba, PR, respectively) are also located along drug trafficking routes but showed higher alcohol use than drug use [6]. These patterns suggest that, beyond trafficking routes, local drug markets, cultural norms, and social context shape which substances are most involved in fatal events. Therefore, more in-depth studies are needed to understand the dynamics of alcohol and other drug use in these regions, ideally combining toxicological data with information on seizures, prices, treatment demand, and community-level use.
Brazil, with its vast size and diverse landscapes, grapples with significant homicide rates despite a decline in certain states. In 2024, over 39,000 deaths resulted from homicides nationwide. The distribution of homicide rates is uneven throughout the country, with the Northeastern states experiencing the highest rates, while the Southeast and South states have witnessed a decline. Moreover, regions characterized by intense drug trafficking, particularly near international borders, tend to exhibit elevated rates. Beyond drug-trade violence, cocaine consumption itself may contribute to the heightened mortality rates observed in specific Brazilian regions, as our findings substantiate a link between cocaine use and homicides, suggesting that increases in cocaine availability and use may be accompanied by greater levels of lethal violence. A Brazilian study found that victims of violent deaths with a previous criminal record were more likely to have consumed any psychoactive substance before death [7], supporting the hypothesis that substance use, criminal involvement, and victimization form a mutually reinforcing cycle in certain populations.
The main strength of the study was the use of blood samples for toxicological analysis, since this is one of the best biological matrices to estimate the effect at the moment of death, meaning that at the time of the fatal event the victim was under the influence of the substance. In addition, the systematic and standardized collection of samples provided valuable inter-regional insights from different Brazilian locations, allowing a better understanding of the burden of drugs on violent deaths through a population-based analysis over a 27-month period and across four macro-regions. This multicenter, probabilistic sampling approach enhances the external validity of our estimates and allows for meaningful comparisons between manners of death and regions.
Despite these strengths, the study also has limitations. Because the locations were selected based on mortality rate data, this could introduce selection bias; however, since cities with large social differences were included, it is believed that generalization to other Brazilian locations is still feasible. Moreover, the lack of medical information in suicide cases makes it impossible to assess whether the benzodiazepines identified were being used under medical supervision or deliberately without professional monitoring. Furthermore, the strategy of excluding cases with more than six hours of medical treatment may have contributed, for example, to the low number of cases resulting from traffic accidents. Therefore, this does not indicate that the selected cities have low traffic-related mortality rates.
As noted above, the cross-sectional design of the study also prevents establishing a causal relationship between drug use and deaths, and toxicological positivity cannot be equated with direct cause of the fatal event. Nevertheless, evidence points to a higher probability of victimization after the consumption of psychoactive substances, a fact supported by the present findings. Therefore, drug use is a reality in the Brazilian population that must be approached holistically, so that the associated morbidity and mortality can be effectively controlled, through a combination of prevention, harm reduction, treatment expansion, and criminal-justice reform.
The relationship between deaths from external causes and drug use was evident in the data presented in this study, with more than half of the victims having consumed psychoactive substances, mainly cocaine and alcohol. Despite extensive debate, alcohol remains the main actor in traffic crashes, whereas cocaine is more associated with homicides and benzodiazepines with suicides. The prohibitionist, criminalizing model of drug control creates parallel – and often violent – markets, which can contribute to drug-related mortality [27] and to environments characterized by systemic and structural violence, in addition to the racial and social injustices intrinsically associated with this perspective. [28]. There is, therefore, an urgent need to address drug consumption from a public health standpoint [29], recognizing that policies which prioritize treatment and social protection over punitive responses are more likely to reduce both substance-related harm and violent deaths. In addition, the geospatial patterns observed in this study, with Belém (PA) and Vitória (ES) showing higher relative involvement of illicit drugs, and Recife (PE) and Curitiba (PR) showing a more prominent role of alcohol, highlight that the burden of psychoactive substances on violent deaths is not homogeneous across the country. These regional differences suggest that prevention and control strategies must be tailored to local profiles of use and market dynamics, rather than relying on a single national model
In summary, the use of psychoactive substances is frequent among victims of violent deaths in Brazil, with more than half of the victims having consumed them, mainly cocaine and alcohol, and the combination of toxicological and geospatial analyses offers a crucial evidence base to guide region-specific, public-health-oriented responses.
Author Contributions
HSB: methodology, investigation, formal analysis, writing – original draft; VC: formal analysis, data curation; IDM: resources, writing – review & editing; HBC: conceptualization; writing – Review & editing, supervision; MY: writing – Review & editing; VL: conceptualization; writing – Review & editing, supervision, project administration, funding acquisition.
Funding
This study received financial support by the Brazilian National Secretary of Drug Policies (SENAD) from the Ministry of Justice (grant number 903126/2020) and was supported by the University of Sao Paulo Medical School (LIM 40/HC-FMSUP). HSB received scholarship by the São Paulo Research Foundation (FAPESP), Brazil. Process Number #2024/04999-7.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee at the Clinical Hospital of the University of Sao Paulo Medical School, Brazil (CAAE: 26797519.9.0000.0065).
Informed Consent Statement
As this study used an aliquot of blood samples that would be used for police investigation, informed consent was waived.
Data Availability Statement
Since this study used data from police reports, even anonymized, to ensure the integrity of the police data, and given that cases may still be under judicial review, the database will not be publicly available. Any questions related to the presented data can be addressed to the corresponding author (HSB: hbombana@usp.br), who will evaluate the possibility of providing any data that does not interfere with ongoing police investigations.
Acknowledgments
Authors are grateful for all staff from the Institutes of Legal Medicine involved in sample collection, specially the director of the institute for supporting the study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BAC | Blood alcohol concentration |
| DPR | Drug problem ratio |
| HDI | Human development index |
| OR | Odds ratio |
| PSA | Psychoactive substances |
| THC | Δ9-tetrahydrocannabinol |
References
- World Health Organization – WHO. Global health estimates: Leading causes of death. Cause-specific mortality, 2000-2021, 2022. Available online: https://www.who.int/data/gho/data/themes/mortality-and-global-health-estimates/ghe-leading-causes-of-death. (accessed on 03/12/2024).
- Brazil, Ministry of Health. External causes mortality data. Available online: https://datasus.saude.gov.br/mortalidade-desde-1996-pela-cid-10. (accessed on 25/11/2025).
- Pan American Health Organization – PAHO. Leading causes of mortality and health loss at regional, subregional, and country levels in the Region of the Americas, 2000-2019. Available online: https://www.paho.org/en/enlace/leading-causes-death-and-disability. (accessed on 03/12/2025).
- Goldstein, P.J. The drugs/violence nexus: a tripartite conceptual framework. J Drug Issues 1985, 15(4), 493-506. [CrossRef]
- Guimarães, R.A.; Mesquita, N.S.; Lopes, R.S; Lucchese, R.; de Felipe, R.L.;Vera, I; Fernandes, I.L.; de Castro, P.A.; Monteiro, L.H.B.; Silva, G.C. Prevalence and Factors Associated with Criminal Behavior Among Illicit Drug Users: A Cross-Sectional Study. Subst Use Misuse 2017, 52(11), 1393-1399. [CrossRef]
- Centro de Excelência para a Redução da Oferta de Drogas Ilícitas – CdE. Dinâmicas do mercado de drogas ilícitas no Brasil. Análise comparativa dos preços de maconha, cocaína e outras drogas em quatro estados. Available online: https://cdesc.org.br/publicacoes/. (accessed on 25/11/2025).
- Andreuccetti, A.; Cherpitel, C.J.; Carvalho, H.B.; Leyton, V.; Miziara, I.; Muñoz, D.R.; Reingold, A.L.; Lemos, N.P. Alcohol in combination with illicit drugs among fatal injuries in Sao Paulo, Brazil: An epidemiological study on the association between acute substance use and injury. Injury 2018, 49, 2186-2192. [CrossRef]
- Auckloo, M.B.K.M.; Davies, B.B. Post-mortem toxicology in violent fatalities in Cape Town, South Africa: A preliminary investigation. J Forensic Leg Med 2019, 63, 18-25. [CrossRef]
- Darke, S.; Duflou, J. Toxicology and circumstances of death of homicide victims in New South Wales, Australia 1996-2005. J Forensic Sci 2008, 53(2), 447-451. [CrossRef]
- Di Candia, D.; Giordano, G.; Boracchi, M.; Zoja, R. Postmortem forensic toxicology cases: A retrospective review from Milan, Italy. J Forensic Sci 2022, 67(4), 1640-1650. [CrossRef]
- De Holanda Júnior, W.P.; Maceno, R.H.M.; Ferreira, M.A.D. Fatores sociodemográficos de mortes violentas relacionadas a substâncias psicoativas lícitas ou ilícitas: estudo transversal, Ceará, 2015-2019. RESS 2024, 33:e2024152. [CrossRef]
- Lemos, Y.V.; Wainstein, A.J.A.; Savoi, L.M.; Drummond-Lage, A.P. Epidemiological and toxicological profile of homicide victims in a legal medicine unit in Brazil. J Forensic Leg Med 2019, 65, 55-60. [CrossRef]
- Sheehan, C.M.; Rogers, R.G.; Williams IV, G.W., Boardman, J.D. Gender differences in the presence of drugs in violent deaths. Addiction 2012, 108(3), 547-555.
- Weiner, M.D.; Sussman, S.; Sun, P.; Dent, C. Explaining the link between violence perpetration, victimization and drug use. Addict Behav 2005, 30(6), 1261-1266. [CrossRef]
- Dalgedan-Bueno, D.; Lindner, S.R.; Kovaleski, D.; Fischer, B. Cannabis use, risk behaviours and harms in Brazil: A comprehensive review of available data indicators. Drug Alcohol Rev 2023, 42(2), 318-336. [CrossRef]
- Stepjanovic, D.; Hall, W.; Leung, J. Illicit drug use and violence. In Handbook of Clinical Neurology, v 197 Brain and Crime; Swaab, H. Meynen, G., Ed.; Elsevier: Netherlands, 2023, 121-145.
- Boles, S.M.; Miotto, K. Substance abuse and violence: A review of the literature. Aggress Violent Behav 2003, 8(2), 155-174. [CrossRef]
- Dalgedan-Bueno, D.; Fischer, B. The association between cocaine product use and violence outcomes in Brazil: A comprehensive, systematized review. Aggress Violent Behav 2024, 101891. [CrossRef]
- Degenhardt, L.; Day, C.; Hall, W.; Conroy, E.; Gilmour, S. Was an increase in cocaine use among injectiong drug users in New South Wales, Australia, accompanied by an increase in violent crime? BMC Public Health 2005, 19:5:40. [CrossRef]
- Garrison, H.; Scholey, A.; Ogden, E.; Benson, S. The effects of alcohol intoxication on cognitive functions critical for driving: A systematic review. Accid Anal Prev 2021, 154:106052. [CrossRef]
- Borges, G.; Monteiro, M.; Cherpitel, C.J.; Orozco, R.; Ye, Y.; Poznyak, V.; Peden, M.; Pechansky, F.; Cremonte, M.; Reid, S.D.; Mendez, J. Alcohol and Road Traffic Injuries in Latin America and the Caribbean: A Case-Crossover Study. Alcohol Clin Exp Res 2017, 41(10), 1731-1737. [CrossRef]
- Bombana, H.S.; Bogstrand, S.T.; Gjerde, H.; Jamt, R.E.G.; Carvalho, H.B.; Andreuccetti, G.; Bernini, C.O.; Muñoz, D.R.; Leyton, V.; Greve, J.M.D. Use of alcohol and illicit drugs by trauma patients in Sao Paulo, Brazil. Injury 2022, 53(1), 30-36. [CrossRef]
- Pelição, F.S.; Peres, M.D.; Pissinate, J.F.; de Paula, D.M.L.; de Faria, M.G.C.; Nakamura-Palacios, E.M.; de Martinis, B.S. Predominance of alcohol and illicit drugs among traffic acidentes fatalities in an urban area of Brazil. Traffic Inj Prev 2016, 17(7), 663-667.
- Ponce, J.C.; Muñoz, D.R.; Andreuccetti, G.; de Carvalho, D.G.; Leyton, V. Alcohol-related traffic accidents with fatal outcomes in the city of Sao Paulo. Accident Anal Prev 2011, 43(3), 782-787. [CrossRef]
- Ponce, J.C.; Kawauti, M.C.P.; Andreuccetti, G.; Carvalho, H.B. Loaded dice: a game theory analysis of drunk driving laws in Brazil. Traffic Inj Prev 2018, 19(8), 794-798. [CrossRef]
- Centro de Excelência para a Redução da Oferta de Drogas Ilícitas – CdE. Tráfico de drogas na Amazônia. Achados iniciais. Available online: https://cdesc.org.br/publicacoes/. (accessed on 25/11/2025).
- Reuter, P. Systemic violence in drug markets. Crime Law Soc Change 2009, 52, 275-284. [CrossRef]
- Miron, J.; Partin, E. Ending the War on Drugs is an Essential Step Toward Racial Justice. Am J Bioeth 2021, 21(4), 1-3. [CrossRef]
- The Lancet. Editorial. Rethinking America’s “War on Drug” as a public-health issue. The Lancet 2001, 31, 357(9261),971.
Figure 1.
Calculated "drug problem ratio" (DPR) for each city included at the study.
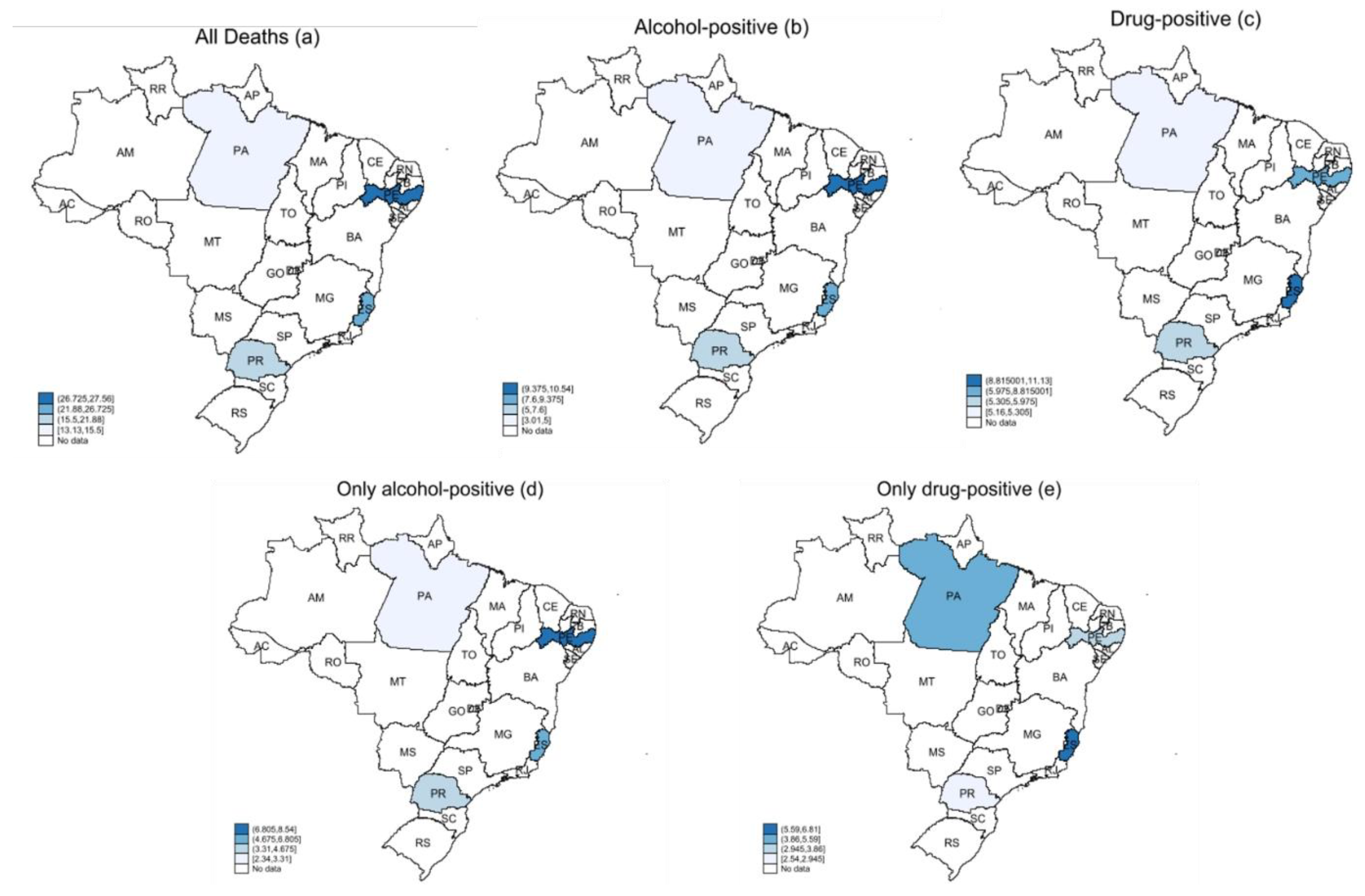

Table 1.
Cities included at the study and its social characteristics.
| City | State | Brazilian geographical region | HDI* | External causes mortality rate/100,000* |
|---|---|---|---|---|
| Belém | Pará (PA) | North | 0.746 | 43.5 |
| Recife | Pernambuco (PE) | Northeast | 0.772 | 143.8 |
| Vitória | Espirito Santo (ES) | Southeast | 0.845 | 197.0 |
| Curitiba | Paraná (PR) | South | 0.885 | 80.4 |
*data from 2021.
Table 2.
Analyzed substances and their analytical cutoffs limits.
| Analyte | Cutoff (ng/mL) | |
|---|---|---|
| Alcohol (g/L) | 0.2 | |
| Cannabis | ||
| ∆9-tetrahydrocannabinol (THC) | 1 | |
| Cocaine and metabolites | ||
| Cocaine | 20 | |
| Benzoylecgonine | 40 | |
| Cocaethylene | 20 | |
| Anhydroecgonine methyl ester (AEME – crack cocaine) | 20 | |
| Amphetamines | ||
| Amphetamine | 20 | |
| Methamphetamine | 20 | |
| MDMA (3,4-methylenedioxymethamphetamine - ecstasy) MDA (3,4-methylenedioxyamphetamine) |
20 | |
| 20 | ||
| Benzodiazepines | ||
| Clonazepam | 5 | |
| 7-aminoclonazepam | 5 | |
| Alprazolam | 5 | |
| Diazepam | 10 | |
| Bromazepam | 20 | |
| Oxazepam | 10 | |
Table 3.
Substance use confirmed among victims by manner of death.
| All deaths | Traffic-related | Homicides | Suicides | Poisoning | All others | |||||||
| % | (95% CI) | % | (95% CI) | % | (95% CI) | % | (95% CI) | % | (95% CI) | % | (95% CI) | |
| n | 3,577 | 524 | 2,406 | 330 | 52 | 265 | ||||||
| General positivity | ||||||||||||
| At least one | 53.0 | (51.3-54.6) | 46.0 | (41.8-50.2) | 55.7 | (53.7-57.7) | 54.6 | (49.1-60.0) | 65.4 | (51.3-77.2) | 37.7 | (32.1-43.7) |
| Only alcohol | 16.6 | (15.4-17.9) | 30.9 | (27.1-35.0) | 14.5 | (13.2-16.0) | 14.5 | (11.1-18.8) | 5.8 | (1.8-16.8) | 12.5 | (8.9-17.0) |
| Only drugs | 21.6 | (20.3-23.0) | 5.5 | (3.9-7.9) | 27.3 | (25.5-29.1) | 10.9 | (7.9-14.8) | 32.7 | (21.2-46.8) | 12.8 | (9.3-17.5) |
| Two or more | 10.9 | (9.9-12.0) | 7.1 | (5.2-9.6) | 11.7 | (10.5-13.1) | 14.8 | (11.4-19.1) | 13.5 | (6.4-26.0) | 6.0 | (3.7-9.6) |
| Specific positivity | ||||||||||||
| Alcohol | 27.7 | (26.2-29.2) | 38.0 | (33.9-42.2) | 26.4 | (24.7-28.2) | 29.4 | (24.7-34.6) | 19.2 | (10.5-32.5) | 18.5 | (14.2-23.7) |
| Cocaine | 29.6 | (28.1-31.1) | 9.9 | (7.6-12.8) | 36.0 | (34.1-38.0) | 21.2 | (17.1-26.0) | 44.2 | (31.2-58.1) | 17.7 | (13.6-22.8) |
| Cannabis | 2.2 | (1.2-2.7) | 0 | 3.2 | (2.5-4.0) | - | - | 0 | - | - | ||
| Benzodiazepines | 6.8 | (6.0-7.7) | 4.4 | (2.9-6.5) | 4.8 | (4.0-5.8) | 20.3 | (16.3-25.0) | 25.0 | (14.9-38.8) | 9.0 | (6.1-13.2) |
| Alcohol + Cocaine | 9.8 | (8.8-10.7) | 5.2 | (3.6-7.4) | 10.9 | (9.7-12.2) | 11.5 | (8.5-15.4) | 13.5 | (6.4-26.0) | 5.3 | (3.1-8.7) |
| Alcohol + Cannabis | - | - | 0 | - | - | 0 | 0 | 0 | ||||
| Alcohol + Benzodiazepines | 1.7 | (1.4-2.2) | 1.9 | (1.0-3.5) | 1.3 | (1.0-1.9) | 4.2 | (2.5-7.0) | 3.9 | (1.0-14.5) | 1.5 | (1.0-4.0) |
Note: - = <0.01.
Table 4.
Substance use according to each substance group by demographic and fatal event characteristics (n = 3,577).
Table 4.
Substance use according to each substance group by demographic and fatal event characteristics (n = 3,577).
| All victims | At least one | Any alcohol | Only alcohol | Only drugs | Two or more | |||||||
| % | (95% CI) | OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | OR | (95% CI) | |
| Sex | ||||||||||||
| Women | 10.9 | (9.9-11.9) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | |||||
| Men | 89.1 | (88.1-90.1) | 1.52 | (1.24-1.89)* | 1.06 | (0.85-1.31) | 1.16 | (0.87-1.57) | 1.92 | (1.42-2.61)* | 1.52 | (1.04-2.25)* |
| Age | ||||||||||||
| Less than 30 | 44.0 | (42.3-45.7) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | |||||
| More than 30 or equal | 56.0 | (54.3-57.8) | 1.09 | (0.95-1.26) | 1.42 | (1.23-1.63)* | 1.94 | (1.59-2.36)* | 0.53 | (0.45-0.63)* | 1.11 | (0.89-1.39) |
| Race | ||||||||||||
| Non-white | 80.8 | (79.4-82.0) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | |||||
| White | 19.2 | (18.0-20.6) | 1.17 | (0.98-1.40) | 2.52 | (2.12-3.03)* | 0.92 | (0.72-1.16) | 0.82 | (0.65-1.03) | 1.64 | (1.27-2.12)* |
| Injury type | ||||||||||||
| All others | 7.4 | (6.6-8.3) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | |||||
| Homicides | 67.3 | (65.7-68.8) | 2.00 | (1.51-2.66)* | 1.42 | (1.06-1.91)* | 1.38 | (0.93-2.08) | 1.98 | (1.32-2.95)* | 2.18 | (1.24-3.83)* |
| Traffic-related | 14.7 | (13.5-15.9) | 1.31 | (0.96-1.80) | 2.30 | (1.66-3.19)* | 3.27 | (2.13-5.02)* | 0.32 | (0.19-0.56)* | 1.22 | (0.64-2.32) |
| Suicide | 9.2 | (8.3-10.2) | 1.81 | (1.28-2.56)* | 2.12 | (1.49-3.02)* | 1.08 | (0.65-1.78) | 0.76 | (0.45-1.28) | 2.70 | (1.43-5.06)* |
| Poisoning | 1.4 | (1.1-1.9) | 2.78 | (1.40-5.51)* | 1.04 | (0.52-2.09) | 1.14 | (1.07-1.22) | 3.71 | (1.77-7.75)* | 2.62 | (0.94-7.27) |
| Death time | ||||||||||||
| Day | 46.1 | (44.3-47.9) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | |||||
| Night | 53.9 | (52.1-55.7) | 1.75 | (1.50-2.04)* | 1.36 | (1.17-1.59) | 2.00 | (1.61-2.48)* | 1.12 | (0.93-1.35) | 1.64 | (1.28-2.10)* |
| Death day | ||||||||||||
| Weekday | 62.6 | (61.0-64.2) | 1.0 | 1.0 | 1.0 | 1.0 | 1.0 | |||||
| Weekend | 37.4 | (35.8-39.0) | 1.52 | (1.32-1.76) | 1.52 | (1.31-1.76)* | 2.28 | (1.89-2.76)* | 0.84 | (0.70-1.01) | 1.41 | (1.13-1.78)* |
*p<0.005.
Table 5.
Mean death rates according to each positivity group and drug problem ratio (DPR = p drug / alcohol positivity) estimates among major regions in Brazil.
Table 5.
Mean death rates according to each positivity group and drug problem ratio (DPR = p drug / alcohol positivity) estimates among major regions in Brazil.
| Regions | All deaths | Alcohol-positive | Drug-positive | Only alcohol | Only drugs | DPR I | DPR II | |||||
| Mean | (95% CI) | Mean | (95% CI) | Mean | (95% CI) | Mean | (95% CI) | Mean | (95% CI) | |||
| PA - North | 13.13 | (5.48-20.78) | 3.01 | (1.55-4.48) | 5.16 | (1.12-9.20) | 2.34 | (1.03-3.66) | 4.37 | (0.66-8.09) | 1.57 | 1.95 |
| PE - Northeast | 27.56 | (21.90-33.23) | 10.54 | (7.92-13.15) | 6.50 | (4.62-8.38) | 8.54 | (6.41-10.67) | 3.35 | (2.26-4.44) | 0.80 | 0.57 |
| ES - Southeast | 25.89 | (21.77-30.01) | 8.21 | (6.21-10.21) | 11.13 | (8.05-14.20) | 5.07 | (2.51-7.63) | 6.81 | (3.47-10.16) | 1.39 | 1.39 |
| PR - South | 17.87 | (13.85-21.88) | 6.99 | (4.69-9.29) | 5.45 | (3.50-7.41) | 4.28 | (2.07-6.49) | 2.54 | (1.60-3.49) | 1.05 | 1.09 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



