
Submitted:
05 December 2025
Posted:
12 December 2025
Read the latest preprint version here
Abstract
Background: Treatment nonadherence in oncology is prevalent and often assessed by surveys that miss the qualitative reasons underpinning nonadherence or treatment discordance. We aimed to synthesize evidence from Natural Language Processing (NLP) studies, primarily sentiment analysis of patient-generated content (social media, forums, blogs, review platforms, and survey free text), to identify communication-related and relational factors linked to nonadherence/concordance. Methods: We conducted a scoping review following PRISMA-ScR. Searches of PubMed, CINAHL, and Scopus (2013–early 2024) targeted NLP studies of the cancer patient experience; conventional reports were included where they clarified communication/adherence constructs. Data were charted against source, cancer type, NLP technique, and inferred adherence/concordance factors, then synthesized using discourse analysis and narrative synthesis. Results: Four patient side themes consistently emerged: (1) unmet emotional needs; (2) suboptimal information and communication; (3) unclear treatment concordance within patient/person-centred care; and (4) online misinformation dynamics (and perceptions of clinician bias). Sentiment analysis detected fine grained emotions (fear, disgust, sadness, surprise), informational gaps and trust issues that are often less visible in structured surveys. Conclusions: Patient voice data offer actionable insights for nursing practice: routine distress screening, teach back strategies, misinformation countermeasures, and explicit concordance checks. Integrating these into person-centred workflows may improve adherence and shared decision making. Registration: Not registered.
Keywords:
discourse analysis
; medication concordance
; natural language processing
; nursing informatics
; oncology
; patient–clinician communication
; person-centred care
; sentiment analysis
; treatment adherence
1. Introduction
Treatment nonadherence in oncology remains a persistent challenge, especially with the growing use of oral anticancer medications (OAMs) administered outside the clinic, which shifts daily responsibility to patients and elevates adherence risk [1]. Although adherence is widely recognized as a multi-factorial construct involving patient and health system dimensions [2,3], the field has relied heavily on structured questionnaires and numeric scores that often fail to illuminate why patients deviate from recommended regimens.
Conventional patient-reported measures present several limitations. Many studies do not distinguish intentional from unintentional nonadherence, this has been described as a distinction that matters for the design of targeted interventions [4]. Survey instruments can be affected by recall bias and acquiescence, and closed-question formats compress experience into fixed categories, obscuring the nuanced reasons behind patient dissatisfaction or discordance with care [5,6,7]. In addition, small or selective samples reduce generalizability, while conceptualizations of “satisfaction” vary, and timelines for acting on feedback can be protracted [9,48]. These constraints limit visibility into the emotional, informational, and relational factors that shape concordance and adherence [10,11,12].
Natural Language Processing (NLP), particularly sentiment analysis of patient-generated narratives, offers a complementary lens on the lived experience of cancer care. Analyses of social media, online support groups, blogs, public review sites, and free-text responses can bring to the surface what have otherwise been “invisible” patient-reported concerns at scale, providing a crowd-validated window into what matters most to patients [13,14]. Compared with structured surveys, sentiment and related text analytics interrogate the tone, polarity, and emotion of language, capturing subtle affective states and informational gaps [15,16]. Prior work has leveraged these approaches to characterize longitudinal emotion dynamics and the role of emotions in adherence behaviors. Examples include hormonal therapy for breast cancer [17] and extraction of patient perspectives across platforms and conditions [18,19,20,21]. Recurrent emotional constructs (e.g., fear, sadness, disgust, surprise) and perceptions of clinician bias or conflicting information have been identified as salient correlates of dissatisfaction, discordance, or withdrawal [22,23,24]. At the same time, patient empowerment in online communities underscores substantial informational needs that may exceed generic emotional support, pointing toward specific communication targets for teams and services [25].
Placing these insights within patient/person-centred care (PCC) highlights the importance of shared decision-making, goal alignment, and relationship quality [26,27,28,29]. If emotions, information needs, and perceptions of communication are key determinants of whether recommendations are accepted, acted upon, and sustained, then synthesizing the “patient voice” from unstructured text should help reveal actionable levers for nursing practice, education, and service design.
Aim and research questions. This scoping review synthesizes evidence from NLP studies of patient-generated narratives (with an emphasis on sentiment analysis) to illuminate how emotions, information needs, and perceptions of communication relate to treatment nonadherence and concordance. Guided by discourse analysis, we address:
2. Method
2.1. Design and Reporting
We conducted a scoping review to map and synthesize evidence on patient generated oncology narratives analyzed using Natural Language Processing (NLP), with emphasis on sentiment analysis. Reporting follows the PRISMA-ScR guideline [30]. Given the anticipated heterogeneity of data sources, analytic pipelines, and outcomes, we complemented PRISMA-ScR with the SWiM guidance for transparent narrative synthesis (nine items). The review questions and eligibility criteria were defined a priori and aligned to the review aim (communication, relationship, and information related determinants of adherence/concordance detectable in the patient voice).
2.2. Eligibility Criteria
Inclusion. Studies were eligible if they: (i) analyzed patient generated text related to cancer using NLP or sentiment analysis (e.g., social media posts, online support communities, blogs, public review platforms, survey free text responses); (ii) reported findings relevant to treatment adherence, nonadherence, or treatment concordance/discordance (definitions below); (iii) were peer reviewed journal articles or full peer reviewed conference papers; and (iv) were published in English between 2013 and early 2024.
Operational definitions. Patient generated text refers to content authored by adult patients themselves (i.e., individuals self-identifying as living with cancer) in public or semi-public online environments or in survey free text fields. Content authored by caregivers, family members, clinicians, journalists, or institutions was excluded unless the text was explicitly written from the patient’s first person perspective and attributable as such. Relevance to adherence/concordance was established through a two step procedure: (a) keyword screening for concepts such as adherence, nonadherence, concordance, compliance, persistence, discontinuation, withdrawal, refusal, skipping doses, dose reduction, stopping treatment, shared decision making (SDM), goals/values alignment, and (b) contextual/thematic confirmation that the text or study findings linked these concepts to treatment taking behavior, decision making, or participation in recommended care.
Exclusion. We excluded studies that: (i) had no cancer focus; (ii) analyzed content produced primarily by carers/children/adolescents rather than adult patients (unless written from the patient’s perspective as defined above); (iii) were economic evaluations, editorials, protocols, or non empirical commentaries; (iv) were non English; or (v) constituted grey literature, with the exception of policy/ethics statements (e.g., WHO, ACSQHC) used for definitional clarity [2,31].
2.3. Information Sources and Search Strategy
We searched PubMed/MEDLINE, CINAHL, and Scopus for records from 2013 to mid 2024. The last search was performed on [15 June 2024]. To maximize sensitivity for studies where titles/abstracts may not co-list all constructs, we built concept blocks around (1) cancer/neoplasms, (2) NLP/sentiment/text mining, (3) patient generated narratives/platforms, and (4) adherence/concordance/SDM constructs, and combined them with Boolean operators. Database specific syntax and field tags were adapted accordingly. Full database strings are provided in Supplementary File S1, including example blocks such as:
- Concept A (cancer):(cancer* OR neoplasm* OR oncolog*)
- Concept B (NLP/SA):("natural language processing" OR "text mining" OR sentiment OR emotion* OR classifier* OR lexicon* OR transformer*)
- Concept C (patient voice/platforms):("social media" OR Twitter OR Reddit OR forum* OR blog* OR "patient review" OR "free text")
- Concept D (adherence/concordance):(adheren* OR nonadheren* OR concordan* OR complian* OR persistence OR discontinu* OR "shared decision*")
To identify additional applications or cross disciplinary work, we ran supplementary searches in Google Scholar and screened reference lists of included records (backward citation chasing) and citing articles where relevant (forward citation chasing). Search results were exported to a reference manager/spreadsheet, and duplicates were removed using automated matching and manual verification.
Automation sensitivity.
Because some platforms are susceptible to automated/bot content and because bot-detection performance varies by method and language, we recorded where source platforms might be affected and treated such findings cautiously, consistent with prior corpus work in oncology narratives [13,15]. When included studies reported bot-filtering or authenticity checks, we noted their approach in the characteristics table.
2.4. Study Selection
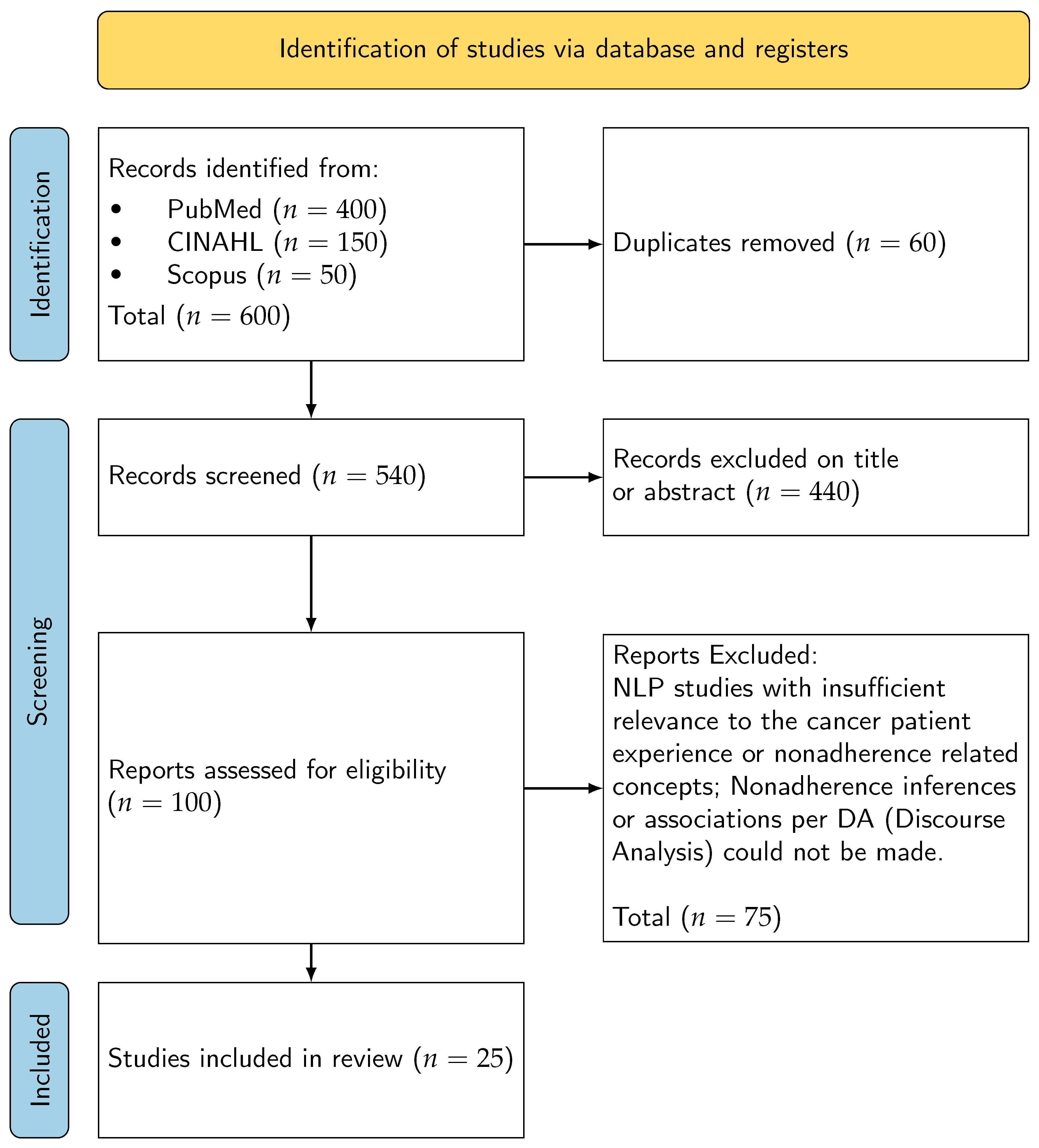
Two reviewers independently screened titles and abstracts against the eligibility criteria. We conducted a calibration exercise on an initial sample to standardize the application of inclusion/exclusion rules. Potentially eligible records underwent full text assessment by the same reviewers. Disagreements were resolved through discussion; a third reviewer was available for arbitration if consensus could not be reached. Reasons for exclusion at the full text stage were documented. The study selection process is depicted in the PRISMA-ScR flow diagram (Figure 1) [30].
2.5. Data Charting
We developed and piloted a standardized charting form aligned to the review questions. Extracted items included: author/year/country; cancer type/domain; data source and platform (e.g., Twitter, Reddit, forums, blogs, survey free text); sampling frame/size; NLP/sentiment methods (e.g., lexicon/rule based, supervised models, transformer architectures; emotion vs. polarity outputs); key analytic parameters (e.g., lexicons used, model transparency); reported adherence/concordance indicators and how they were operationalized; and main findings relevant to emotions, information, and relationships. The form was iteratively refined after piloting. Charted data informed a characteristics table and thematic synthesis of patient side constructs.
2.6. Critical Appraisal
Given the heterogeneity of study designs (observational NLP analyses; mixed methods; qualitative components), we used the Critical Appraisal Toolkit (CAT) to describe methodological rigor across sources [32]. Appraisal focused on clarity of research question, appropriateness and transparency of data sources and NLP pipelines, sampling limitations and platform biases, validity of adherence/concordance inferences, and ethical handling of online content. Ratings (e.g., low/medium/high) and brief justifications were recorded to inform interpretation rather than to exclude studies, consistent with scoping review practice [33,34].
2.7. Ethical Considerations for Online Patient Generated Data
We followed the Association of Internet Researchers’ ethics principles (contextual integrity, harm minimization) and relevant clinical communications guidance [31,34]. We restricted attention to public or clearly semi-public spaces; private groups or closed forums requiring membership approval were not targeted as primary sources. Where studies quoted user content, we favored paraphrased reporting in this review to reduce traceability via search engines. No attempts were made to identify or re-identify individuals. Platform terms of service and community guidelines cited by included studies were noted where available. The review used only published, aggregated findings from included sources and did not involve intervention or contact with users; institutional ethical review was therefore not required for this synthesis.
2.8. Synthesis Approach
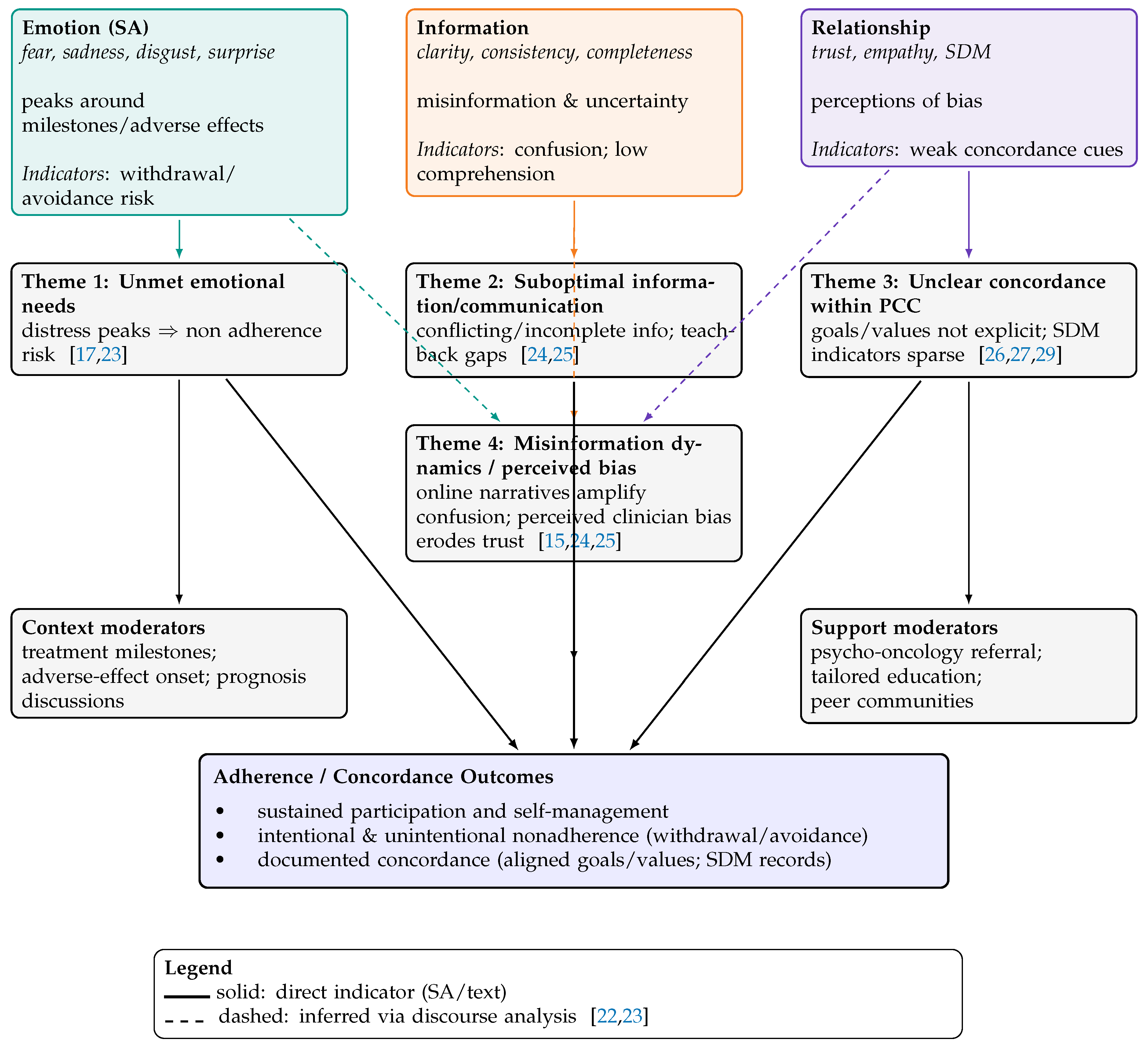
We employed a two stage synthesis. First, we mapped included studies by platform, cancer domain, and NLP approach to describe the evidence landscape. Second, we undertook narrative synthesis, integrating discourse analysis to link sentiment derived constructs (emotion, information clarity, relationship/trust/SDM) to adherence and concordance phenomena [22,23]. To enhance transparency (SWiM), we pre-specified groupings by platform (Twitter/X, Reddit, forums/blogs, survey free text), analytic family (lexicon/rule based vs. supervised/transformer), and cancer domain; we summarized outcomes using standardized polarity/emotion metrics where available and otherwise used structured textual summaries. We explored heterogeneity by platform and method and prioritized results by analytic transparency and sample size. Visual synthesis is provided via a conceptual map (Figure 2), indicating whether links were directly observed in sentiment outputs or inferred through discourse analysis.
2.9. Synthesis Without Meta Analysis (SWiM)
In line with SWiM, we: (i) specified the synthesis objective (identify communication, information, and relationship related determinants of adherence/concordance emergent from patient narratives); (ii) defined grouping variables (platform, cancer domain, NLP family); (iii) stated outcome handling (polarity/emotion classes, concordance/adherence indicators); (iv) described the synthesis method (structured narrative plus discourse analysis); (v) addressed limitations of combining diverse metrics (no quantitative pooling; emphasis on direction and consistency of effects/signals); (vi) examined heterogeneity qualitatively (by platform/method and appraisal ratings); (vii) considered study appraisal in interpretation (down weighting weakly reported inferences); (viii) used visual displays (PRISMA diagram; conceptual map); and (ix) documented decisions and deviations (in Supplementary File S4). Reporting complements PRISMA-ScR to support reproducible narrative synthesis [30].
3. Results
3.1. Study Selection and Overview
From an initial corpus spanning PubMed, CINAHL, and Scopus (2013–early 2024), 25 studies met the inclusion criteria for analysis of patient-generated cancer narratives using NLP or sentiment analysis. Reasons for exclusion included non-cancer focus, non-English language, content authored by carers or children, and grey literature outside defined exceptions. The study selection process is illustrated in the PRISMA flow diagram (Figure 1).
Figure 1.
PRISMA Flow Diagram [30].
Figure 1.
PRISMA Flow Diagram [30].
3.2. Characteristics of Included Studies
The included studies varied in cancer type, data source (e.g., Twitter, forums, blogs, survey free text), and NLP technique (e.g., rule-based filtering, transformer models, emotion classification). Table 1, Table 2, Table 3 and Table 4 summarizes these characteristics, highlighting the adherence or concordance indicators most relevant to nursing practice.
3.3. Emergent Patient-Side Themes
Narrative synthesis and discourse analysis revealed four recurrent patient-side themes:
- Unmet Emotional Needs: Emotions such as fear, sadness, disgust, and surprise peaked around treatment milestones and adverse effects, often correlating with withdrawal or intentional nonadherence.
- Suboptimal Information and Communication: Conflicting or incomplete information, including misleading framings (e.g., “good cancer”), contributed to confusion and reduced trust in care teams.
- Unclear Concordance within Person-Centred Care (PCC): Patient narratives often lacked explicit indicators of shared decision-making (SDM) or goal alignment, suggesting missed opportunities for concordance checks.
- Online Misinformation Dynamics and Perceived Clinician Bias: Online narratives amplified confusion and sometimes reflected perceived bias, further eroding trust and complicating adherence.
These themes are visualized in the conceptual map (Figure 2), which links sentiment-derived constructs (emotion, information, relationship) to adherence outcomes via direct and inferred indicators.
3.4. Theme Prevalence Across Studies
Table 5 reports the prevalence of each theme across the included studies. Suboptimal communication and unclear concordance were the most frequently observed, followed by emotional distress and misinformation dynamics.
3.5. Operational Definitions of Adherence and Concordance
To clarify key constructs:
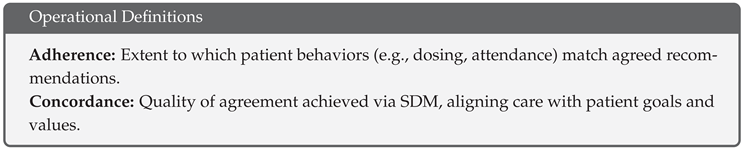
These definitions are mapped to the Three Talk SDM model (Team, Option, Decision talk) and inform the interpretation of patient voice data.
3.6. Emotion–Behavior–Response Framework
Table 6 presents a practical framework linking emotion signals to likely patient behaviors and concordance-oriented nursing responses. For example, fear may lead to dose skipping, which can be addressed through distress screening and values clarification.
3.7. Narrative Summary
Across platforms, emotional distress was a consistent signal of nonadherence risk. Informational gaps and conflicting messages undermined understanding and trust, while sparse evidence of SDM pointed to missed opportunities for concordance. Online misinformation and perceived bias further complicated the communication landscape. These findings suggest that integrating emotion detection, teach-back strategies, and concordance checks into nursing workflows may improve adherence and patient engagement.
4. Discussion
This scoping review synthesizes findings from 25 studies that used primarily NLP-based sentiment analysis to explore cancer patient treatment nonadherence and discordance. The review identifies four key themes: unmet emotional needs, suboptimal communication and information, unclear concordance in Patient Centred Care (PCC), and EHR barriers and compliance design.
4.1. Linking Findings to Review Questions
The review addressed two questions: (1) how secondary data from NLP studies can reveal insights hidden from traditional surveys, and (2) how oncologist narratives in EHRs reflect communication factors linked to nonadherence. The findings suggest that NLP techniques, particularly sentiment analysis, can uncover emotional and relational dimensions of the patient experience that are often overlooked in conventional research [13,14].
4.2. Conceptual Contributions
This review contributes to the understanding of treatment nonadherence by showing that discordance is more frequently inferred than directly measured. Emotional constructs such as fear, sadness, and spiritual pain were detected in patient authored content but rarely documented in EHRs [23,36]. The review also highlights the potential of NLP to detect fine grained emotional states and communication breakdowns that influence adherence.
4.3. Platform and Methodological Insights
Sentiment analysis of social media and online support groups revealed richer emotional content than text mining of EHRs, which often lacked adherence related notes. Studies suggest oncologists may avoid documenting adverse effects or emotional distress due to time constraints or EHR design limitations [52,53]. This discrepancy underscores the need for improved EHR systems that support narrative input and patient centred documentation.
4.4. Appraisal Informed Interpretation
Using the Critical Appraisal Toolkit (CAT) [32], studies were rated for methodological rigor. High quality studies provided clearer links between patient sentiment and adherence, while lower quality studies often lacked transparency in NLP pipelines or adherence definitions. This informed the weighting of evidence in the synthesis.
4.5. Implications for Practice
Findings suggest that oncologist communication, emotional support, and shared decision making are central to treatment concordance. NLP tools could be used to monitor patient sentiment and flag potential nonadherence risks. However, ethical considerations and interpretive caution are essential, especially when analyzing public online data [4,34].
4.6. Limitations
The review is limited by the interpretive nature of discourse analysis and the paucity of NLP studies directly addressing nonadherence. Economic factors were excluded, and the focus was primarily on oral anti cancer medication. Bias may arise from inferring nonadherence from related concepts, though this was mitigated by referencing prior work [4].
5. Conclusions
Despite limited direct evidence, this scoping review demonstrates that NLP studies of the cancer patient experience can infer treatment nonadherence and discordance through discourse analysis. Emotional needs may surpass informational needs, and oncologist attitudes and communication styles significantly influence concordance.
Most NLP studies focus on technical extraction rather than clinical application. However, sentiment analysis reveals unmet emotional needs and dissatisfaction that may impact adherence. EHR text mining shows that oncologist notes often lack detail on adverse effects, pain, or emotional distress, potentially due to time constraints or compliance oriented design [52,53].
Improved oncologist communication and shared narratives in EHRs could enhance health literacy and treatment concordance. Future research should develop lexicons and NLP models that detect oncologist patient communication barriers and treatment discordance. A combined qualitative and NLP approach may offer deeper insight into the patient experience and support the aims of Patient Centred Care [26,27].
Author Contributions
Conceptualization, L.W.; methodology, L.W., R.G. and X.Z; formal analysis, L.W.; investigation, L.W; writing original draft preparation, L.W; writing review and editing, L.W., R.G. and X.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive any funding.
Institutional Review Board Statement
Ethical review was not needed for this study.
Public Involvement Statement
There was no public involvement in any aspect of this research.
Guidelines and Standards Statement
This manuscript was drafted against the PRISMA-ScR checklist for reporting of scoping reviews.
Use of Artificial Intelligence
Generative AI tools were not used in drafting this manuscript. However, the study relies on AI based analytical methods such as Natural Language Processing (NLP) and sentiment analysis to examine patient generated narratives. Existing AI tools were employed strictly for data analysis, not for content creation.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Belcher; S. M. Mackler; E. Muluneh; B. Ginex; P. K. Anderson; M. K. Bettencourt; E. DasGupta; R. K. Elliott; J. Hall; E. Karlin; M. Kostoff; D. Marshall; V. K. Millisor; V. E. Molnar; M. Schneider; S. M. Tipton; J. Yackzan; S. LeFebvre; K. B. Sivakumaran; K.;Waseem; H. ONS Guidelines™ to Support Patient Adherence to Oral Anticancer Medications. Oncology Nursing Forum 2022, 49(4), 279–295. [CrossRef]
- Sabaté, W. H. O. Adherence to long-term therapies: evidence for action. World Health Organization, Switzerland 2003, 198. Available online: https://www.google.com.au/books/edition/Adherence_to_Long_term_Therapies/kcYUTH8rPiwC?hl=en&gbpv=0.
- Brown, M. T.; Bussell, J. K. Medication adherence: WHO cares? Mayo Clin Proc 2011, 86(4), 304–314. [Google Scholar] [CrossRef]
- Wreyford; L. Gururajan; R.; Zhou; X. When can cancer patient treatment nonadherence be considered intentional or unintentional? A scoping review. Unknown Journal 2023, 18(5), e0282180. [CrossRef]
- Chung; E. H. Mebane; S. Harris; B. S. White; E.; Acharya; K. S. Oncofertility research pitfall? Recall bias in young adult cancer survivors. F S Rep 2023, 4(1), 98–103. [CrossRef]
- Felipe; D. David; E. Mario; M.; Qiao; W. Bias in patient satisfaction surveys: a threat to measuring healthcare quality. BMJ Global Health 2018, 3(2), e000694. [CrossRef] [PubMed]
- Lindberg; P. Netter; P. Koller; M. Steinger; B.; Klinkhammer-Schalke; M. Breast cancer survivors’ recollection of their quality of life: Identifying determinants of recall bias in a longitudinal population-based trial. PLoS One 2017, 12(2), e0171519. [CrossRef]
- Shah, A. M.; Yan, X.; Tariq, S.; Ali, M. What patients like or dislike in physicians: Analyzing drivers of patient satisfaction and dissatisfaction using a digital topic modeling approach. Information Processing & Management 2021, 58(3), 102516. [Google Scholar] [CrossRef]
- Nawab; K. Ramsey; G.; Schreiber; R. Natural Language Processing to Extract Meaningful Information from Patient Experience Feedback. Appl Clin Inform 2020, 11(2), 242–252. [CrossRef]
- Ng, J.; Luk, B. Patient satisfaction: Concept analysis in the healthcare context. Patient education and counseling 2019, 102(4), 790–796. [Google Scholar] [CrossRef] [PubMed]
- Lasala, R.; Santoleri, F. Association between adherence to oral therapies in cancer patients and clinical outcome: A systematic review of the literature. British Journal of Clinical Pharmacology 2022, 88(5), 1999–2018. [Google Scholar] [CrossRef] [PubMed]
- Yoder; A. K. Dong; E. Yu; X. Echeverria; A. Sharma; S. Montealegre; J.; Ludwig; M. S. Effect of Quality of Life on Radiation Adherence for Patients With Cervical Cancer in an Urban Safety Net Health System. International Journal of Radiation Oncology, Biology, Physics 2023, 116(1), 182–190. [CrossRef] [PubMed]
- Clark, J.; Jones, T.; Alapati, A.; Ukandu, D.; Danforth, D.; Dodds, D. A Sentiment Analysis of Breast Cancer Treatment Experiences and Healthcare Perceptions Across Twitter. arXiv 2018, arXiv:1805.09959. [Google Scholar] [CrossRef]
- Turpen, T.; Matthews, L.; Matthews, S. G.; Guney, E. Beneath the surface of talking about physicians: A statistical model of language for patient experience comments. Patient Experience Journal 2019, 6(1), 51–58. [Google Scholar] [CrossRef]
- Lai; Rayson; P. Payne; S.; Liu; Y. Analysing Emotions in Cancer Narratives: A Corpus-Driven Approach. In Proceedings of the First Workshop on Patient-Oriented Language Processing (CL4Health) @ LREC-COLING 2024, Torino, Italia, 2024; pp. 73–83.
- Mishra, M. V.; Bennett, M.; Vincent, A.; Lee, O. T.; Lallas, C. D.; Trabulsi, E. J.; Gomella, L. G.; Dicker, A. P.; Showalter, T. N. Identifying barriers to patient acceptance of active surveillance: content analysis of online patient communications. PLOS ONE 2013, 8(9), e68563. [CrossRef]
- Yin; Z. Malin; B. Warner; J. Hsueh; P.; Chen; C. The Power of the Patient Voice: Learning Indicators of Treatment Adherence From An Online Breast Cancer Forum. Eleventh International AAAI Conference on Web and Social Media Montreal, Quebec, Canada, 2017. [CrossRef]
- Babel; R. Taneja; R. Mondello; M. Monaco; A.; Donde; S. Artificial Intelligence Solutions to Increase Medication Adherence in Patients With Non-communicable Diseases [Review]., Volume 3 - 2021. Frontiers in Digital Health 2021, 3. [CrossRef]
- Robinson, S.; Vicha, E. Twitter Sentiment at the Hospital and Patient Level as a Measure of Pediatric Patient Experience. Open Journal of Pediatrics 2021. [Google Scholar] [CrossRef]
- Sim; J. A. Huang; X. Horan; M. R. Baker; J. N.; Huang; I. C. Using natural language processing to analyze unstructured patient-reported outcomes data derived from electronic health records for cancer populations: a systematic review. Expert Rev Pharmacoecon Outcomes Res 2024, 24(4), 467–475. [CrossRef]
- Babel; R. Taneja; R. Mondello; M. Monaco; A.; Donde; S. Artificial Intelligence Solutions to Increase Medication Adherence in Patients With Non-communicable Diseases [Review]. Frontiers in Digital Health 2021, 3. [CrossRef]
- Li, C.; Fu, J.; Lai, J.; Sun, L.; Zhou, C.; Li, W.; Jian, B.; Deng, S.; Zhang, Y; Guo, Z.; Liu, Y.; Zhou, Y.; Xie, S.; Hou, M.; Wang, R; Chen, Q.; Wu, Y. Construction of an Emotional Lexicon of Patients with Breast Cancer: Development and Sentiment Analysis. Journal of Medical Internet Research 2023, 25, e44897. [Google Scholar] [CrossRef] [PubMed]
- Chichua, M.; Filipponi, C.; Mazzoni, D.; Pravettoni, G. The emotional side of taking part in a cancer clinical trial. PLOS ONE 2023, 18(4), e0284268. [Google Scholar] [CrossRef]
- Freedman, R. A.; Viswanath, K.; Vaz-Luis, I.; Keating, N. L. Learning from social media: utilizing advanced data extraction techniques to understand barriers to breast cancer treatment. Breast Cancer Research and Treatment 2016, 158(2), 395–405. [Google Scholar] [CrossRef]
- Verberne, S.; Batenburg, A.; Sanders, R.; van Eenbergen, M.; Das, E.; Lambooij, M. S. Analyzing Empowerment Processes Among Cancer Patients in an Online Community: A Text Mining Approach. JMIR Cancer 2019, 5(1), e9887. [Google Scholar] [CrossRef]
- Greene; S. M. Tuzzio; L.; Cherkin; D. A framework for making patient-centered care front and center. Perm J 2012, 16(3), 49–53. [CrossRef]
- Robinson; J. H. Callister; L. C. Berry; J. A.; Dearing; K. A. Patient-centered care and adherence: definitions and applications to improve outcomes. J Am Acad Nurse Pract 2008, 20(12), 600–607. [CrossRef] [PubMed]
- Fix; G. M. VanDeusen Lukas; C. Bolton; R. E. Hill; J. N. Mueller; N. LaVela; S. L.; Bokhour; B. G. Patient-centred care is a way of doing things: How healthcare employees conceptualize patient-centred care. Health Expect 2018, 21(1), 300–307. [CrossRef]
- Mead, H.; Wang, Y.; Cleary, S.; Arem, H.; Pratt-Chapman, L. M. Defining a patient-centered approach to cancer survivorship care: development of the patient centered survivorship care index (PC-SCI). BMC Health Services Research 2021, 21(1), 1353. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann Intern Med 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Australian Commission on Safety and Quality in Health Care. Australian Charter of Healthcare Rights (Second Edition). Australian Commission on Safety and Quality in Health Care. 2020. Available online: https://www.safetyandquality.gov.au/publications-and-resources/resource-library/australian-charter-healthcare-rights-second-edition-a4-accessible.
- Moralejo, D.; Ogunremi, T.; Dunn, K. Critical Appraisal Toolkit (CAT) for assessing multiple types of evidence. Can Commun Dis Rep 2017, 43(9), 176–181. [Google Scholar] [CrossRef]
- Skeat, J.; Roddam, H. The qual-CAT: Applying a rapid review approach to qualitative research to support clinical decision-making in speech-language pathology practice. Evidence-Based Communication Assessment and Intervention 2019, 13(1-2), 3–14. [Google Scholar] [CrossRef]
- CASP. Critical Appraisal Skills Programme; CASP UK - OAP Ltd, 2023; Available online: https://casp-uk.net/casp-tools-checklists/ (accessed on 23 September 2024).
- Cho, J. E.; Tang, N.; Pitaro, N.; Bai, H.; Cooke, P. V.; Arvind, V. Sentiment Analysis of Online Patient-Written Reviews of Vascular Surgeons. Ann Vasc Surg 2023, 88, 249–255. [Google Scholar] [CrossRef]
- Masiero, M.; Spada, G. E.; Fragale, E.; Pezzolato, M.; Munzone, E.; Sanchini, V.; Pietrobon, R.; Teixeira, L.; Valencia, M.; Machiavelli, A.; Woloski, R.; Marzorati, C.; Pravettoni, G. Adherence to oral anticancer treatments: network and sentiment analysis exploring perceived internal and external determinants in patients with metastatic breast cancer. Supportive Care in Cancer 2024, 32(7), 458. [Google Scholar] [CrossRef]
- Li, C.; Ure, C.; Zheng, W.; Zheng, C.; Liu, J.; Zhou, C.; Jian, B.; Sun, L.; Li, W.; Xie, L.; Mai, Y.; Zhao, H.; Liu, Y.; Lai, J.; Fu, J.; Wu, Y. Listening to voices from multiple sources: A qualitative text analysis of the emotional experiences of women living with breast cancer in China. Frontiers in Public Health 2023, 11, 1114139. [Google Scholar] [CrossRef]
- Meksawasdichai, S.; Lerksuthirat, T.; Ongphiphadhanakul, B.; Sriphrapradang, C. Perspectives and Experiences of Patients with Thyroid Cancer at a Global Level: Retrospective Descriptive Study of Twitter Data. JMIR Cancer 2023, 9, e48786. [Google Scholar] [CrossRef] [PubMed]
- Podina, I. R.; Bucur, A.-M.; Todea, D.; Fodor, L.; Luca, A.; Dinu, L. P.; Boian, R. F. Mental health at different stages of cancer survival: a natural language processing study of Reddit posts. Frontiers in Psychology 2023, 14, 1150227. [Google Scholar] [CrossRef]
- Mazza, M.; Piperis, M.; Aasaithambi, S.; Chauhan, J.; Sagkriotis, A.; Vieira, C. Social Media Listening to Understand the Lived Experience of Individuals in Europe With Metastatic Breast Cancer: A Systematic Search and Content Analysis Study. Frontiers in Oncology 2022, 12, 863641. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Yada, S.; Aramaki, E.; Yajima, H.; Kizaki, H.; Hori, S. Extracting Multiple Worries From Breast Cancer Patient Blogs Using Multilabel Classification With the Natural Language Processing Model Bidirectional Encoder Representations From Transformers: Infodemiology Study of Blogs. JMIR Cancer 2022, 8(2), e37840. [Google Scholar] [CrossRef] [PubMed]
- Cercato, M. C.; Colella, E.; Fabi, A.; Bertazzi, I.; Giardina, B. G.; Di Ridolfi, P.; Mondati, M.; Petitti, P.; Bigiarini, L.; Scarinci, V; Franceschini, A.; Servoli, F.; Terrenato, I.; Cognetti, F.; Sanguineti, G.; Cenci, C. Narrative medicine: feasibility of a digital narrative diary application in oncology. Journal of International Medical Research 2021, 50(2), 1–12. [Google Scholar] [CrossRef]
- Vehviläinen-Julkunen, K.; Turpeinen, S.; Kvist, T.; Ryden-Kortelainen, M.; Nelimarkka, S.; Enshaeifar, S.; Faithfull, S. Experience of Ambulatory Cancer Care: Understanding Patients’ Perspectives of Quality Using Sentiment Analysis. Cancer Nursing 2021, 44(6), E331–E338. [Google Scholar] [CrossRef]
- Law, E. H.; Auil, M. J.; Spears, P. A.; Berg, K.; Winnette, R. Voice Analysis of Cancer Experiences Among Patients With Breast Cancer: VOICE-BC. Journal of Patient Experience 2021, 8, 23743735211048058. [Google Scholar] [CrossRef]
- Yerrapragada, G.; Siadimas, A.; Babaeian, A.; Sharma, V.; O’Neill, T. J. Machine Learning to Predict Tamoxifen Nonadherence Among US Commercially Insured Patients With Metastatic Breast Cancer. JCO Clinical Cancer Informatics 2021, 5, 814–825. [Google Scholar] [CrossRef]
- Moraliyage, H.; De Silva, D.; Ranasinghe, W.; Adikari, A.; Alahakoon, D.; Prasad, R.; Lawrentschuk, N.; Bolton, D. Cancer in Lockdown: Impact of the COVID-19 Pandemic on Patients With Cancer. The Oncologist 2021, 26(2), e342–e344. [Google Scholar] [CrossRef]
- Balakrishnan, A.; Idicula, S. M.; Jones, J. Deep learning-based analysis of sentiment dynamics in online cancer community forums: An experience. Health Informatics Journal 2021, 27(2), 14604582211007537. [Google Scholar] [CrossRef]
- Shah, A. M.; Yan, X.; Tariq, S.; Ali, M. What patients like or dislike in physicians: Analysing drivers of patient satisfaction and dissatisfaction using a digital modelling approach. Information Processing & Management 2021, 58(3), 102516. [Google Scholar] [CrossRef]
- Arditi, C.; Walther, D.; Gilles, I.; Lesage, S.; Griesser, A.-C.; Bienvenu, C.; Eicher, M.; Peytremann-Bridevaux, I. Computer-assisted textual analysis of free-text comments in the Swiss Cancer Patient Experiences (SCAPE) survey. BMC Health Services Research 2020, 20, 1029. [Google Scholar] [CrossRef]
- Adikari, A.; Ranasinghe, W.; de Silva, D.; Alahakoon, D.; Prasad, R.; Lawrentschuk, N.; Bolton, D. Can online support groups address psychological morbidity of cancer patients? An AI-based investigation of prostate cancer trajectories. PloS one 2020, 15(3), e0229361. [Google Scholar] [CrossRef]
- Mikal, J.; Hurst, S.; Conway, M. Codifying Online Social Support for Breast Cancer Patients: Retrospective Qualitative Assessment. J Med Internet Res 2019, 21(10), e12880. [Google Scholar] [CrossRef]
- Elbers, L.A.; Minot, J.R.; Gramling, R.; Brophy, M.T.; Do, N.V. Sentiment analysis of medical record notes for lung cancer patients at the Department of Veterans Affairs. PLOS ONE 2023, 18(1), e0280931. [Google Scholar] [CrossRef]
- Patel, M. R.; Friese, C. R.; Mendelsohn-Victor, K.; et al. Clinician Perspectives on Electronic Health Records, Communication, and Patient Safety Across Diverse Medical Oncology Practices. J Oncol Pract 2019, 15(6), e529–e536. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Summary of cancer patient studies (Part 1 of 4)
| Author & Title | Method | Data Sources | Sample | Results | NLP Technique | Nonadherence/ Inference |
|---|---|---|---|---|---|---|
| Clark et al., 2018. [13] A Sentiment Analysis of Breast Cancer Treatment Experiences and Healthcare Perceptions Across Twitter |
Quantitative | ∼5.3 million “breast cancer” related tweets. CAT: Strength=Moderate; Quality = Medium |
Invisible patient-reported outcomes (iPROs) captured; positive experiences shared; fear of legislation causing loss of coverage. | Supervised machine learning combined with NLP | US context: fear of not receiving care salient; analogous issues elsewhere may include lack of insurance and long waiting periods. | |
| Turpen et al., 2019. [14] Beneath the surface of talking about Physicians: A statistical model of language for patient experience comments |
Analysis of patient comments from surveys | Anonymous patient satisfaction surveys | 25,161 surveys. CAT: Strength=Moderate; Quality = Medium |
Statistically significant differences in language used for higher- vs lower-rated physicians. | Frequency of 300 pre-selected n-grams | Time spent with patients matters; longer physician times can enhance treatment adherence. |
| Mishra et al., 2013. [16] Identifying barriers to patient acceptance of active surveillance: Content analysis of online patient communications |
Qualitative | Online conversations (prostate cancer patients) | 34 websites; 3,499 online conversations. CAT: Strength = Weak; Quality = Low |
Patients often believed specialist information was biased. | NLP to identify content & sentiment; ML; internal data dictionary | Perceived physician bias undermines trust and concordance; may influence treatment nonadherence; “suspicion of bias” emerged as a new theme. |
| Yin et al., 2017. [17] The Power of the Patient Voice: Learning Indicators of Treatment Adherence from an Online Breast Cancer Forum |
Quantitative | Breastcancer.org | Retrospective study of 130,000 posts from 10,000 patients over 9 years. CAT: Strength=Moderate; Quality = Medium |
Results correlated with traditional adherence surveys; emotions/personality readily detected online; scale increases relevance. | Logistic Regression (ML); emotion analysis | Treatment completion associated with joy (and some disgust/sadness); fear, especially of side effects, persistent and sometimes overlooked. |
| Li J et al., 2023. [22] Construction of an Emotional Lexicon of Patients with Breast Cancer: Development and Sentiment Analysis |
Qualitative | Weibo (Chinese social media platform) | 150 written materials; 17 interviews; 6,689 posts/comments. CAT: Strength = Weak; Quality = Low |
Emotional lexicon with fine-grained categories; new perspective for recognizing emotions/needs; enables tailored emotional management plans. | Emotional lexicon; manual annotation (two general lexicons + BC-specific) | Emotional expressions may predict adherence; effective emotional management may be as important as information; without support, intentional nonadherence influenced by poor provider relationships. |
| Chichua et al., 2023. [23] The emotional side of taking part in a cancer clinical trial |
Quantitative | Public posts re: clinical trials; Reddit communities | 129 cancer patients; 112 caregivers. CAT: Strength=Moderate; Quality = Medium |
Fear identified as the highest emotion. | Keywords; NRC Emotion Lexicon; sentiment analysis | Sharing emotional experiences may increase fear of treatment withdrawal; trust in the physician is an important factor (potential barrier) in clinical trials. |
| Freedman et al., 2016. [24] Learning from social media: utilizing advanced data extraction techniques to understand barriers to breast cancer treatment |
Qualitative | Message boards; blogs; topical sites; content-sharing sites; social networks | 1,024,041 social media posts about breast cancer treatment. CAT: Strength=Moderate; Quality = Medium |
Fear was the most common emotional sentiment expressed. | Machine Learning (ConsumerSphere software) | Fear of side effects dominant; links to poor physician relationships and lack of treatment concordance; rudeness a factor in poor communication. |
| Verberne et al., 2019. [25] Analysing empowerment Processes Among Cancer Patients in an Online Community: A Text Mining Approach |
Posts labelled for empowerment and psychological processes | Forum for cancer patients and relatives | 5,534 messages in 1,708 threads by 2,071 users. CAT: Strength = Weak; Quality = Medium |
The need for informational support exceeded emotional support. | LIWC | Lack of information may result in unintentional treatment nonadherence. |
Table 2.
Summary of cancer patient studies (Part 2 of 4)
| Author & Title | Method | Data Sources | Sample | Results | NLP Technique | Nonadherence/ Inference |
|---|---|---|---|---|---|---|
| Cho et al., 2023. [35] Sentiment Analysis of Online Patient-Written Reviews of Vascular Surgeons | Quantitative (sentiment analysis and machine learning) | SVS member directory cross-referenced with a patient–physician review website | 1,799 vascular surgeons.CAT: Strength = Weak; Quality = Medium | The positivity/negativity of reviews largely related to words associated with the patient–doctor experience and pain. | Word-frequency assessments; multivariable analyses | Physician communication is a key factor influencing patient dissatisfaction and potentially nonadherence. |
| Masiero et al., 2024. [36] Adherence to oral anticancer treatments: network and sentiment analysis exploring perceived internal and external determinants in patients with metastatic breast cancer | Qualitative | Division of Senology, European Institute of Oncology | 19 female metastatic breast cancer patients.CAT: Strength=Moderate; Quality = Medium | Themes: individual clinical pathway; barriers to adherence; resources to adherence; perception of new technologies. | Word-cloud plots; network analysis; sentiment analysis | Patients experience fear related to clinical values; ineffective communication; discontinuity of patient care. |
| Li C et al., 2023. [37] Listening to voices from multiple sources: A qualitative text analysis of the emotional experiences of women living with breast cancer in China | Qualitative | (1) Six tertiary hospitals (expressive writing);(2) Semi-structured interviews;(3) Weibo | 5,675 Weibo posts.CAT: Strength=Moderate; Quality = Medium | Breast cancer patients require benefit finding and cognitive re-appraisal with strong social support; patients require screening for emotional support. | Python web crawler (Weibo posts/comments) | Emotional distress is an unmet need; healthcare professionals should provide multiple support channels; peer support may alleviate distress. |
| Meksawasdichai et al., 2023. [38] Perspectives and Experiences of Patients with Thyroid Cancer at a Global Level: Retrospective Descriptive Study of Twitter Data | Quantitative | Retrospective tweets relevant to thyroid cancer | 13,135 tweets.CAT: Strength=Moderate; Quality = Low | Twitter may provide an opportunity to improve patient–physician engagement or serve as a research data source. | Twitter scraping; sentiment analysis | Support in self-management is a main topic; physicians may need to recommend online resources; lack of support may lead to unintentional nonadherence. |
| Podina et al., 2023. [39] Mental Health at Different Stages of Cancer Survival: A Natural Language Processing Study of Reddit Posts | Mixed methods | 187 users; 72,524 posts.CAT: Strength=Moderate; Quality = Medium | Short-term survivors are more likely to suffer depression than long-term; support in daily needs is lacking. | Lexicon and machine learning | Need for online social media support; patients do not typically discuss aspects of their disease with health professionals; lack of trust and concordance influence treatment nonadherence. | |
| Manuelita Mazza et al., 2022. [40] Social media Listening to Understand the Lived Experience of Individuals in Europe with Metastatic Breast Cancer: A Systematic Search and Content Analysis Study | Non-interventional retrospective analysis of public social media | Social media posts (Twitter; patient forums) | 76,456 conversations during 2018–2020.CAT: Strength=Moderate; Quality = Medium | Twitter was the most common platform; 61% authored by patients, 15% by friends/family, 14% by caregivers. | Predefined search string; content analysis | Poor communication and suboptimal relationships may influence treatment nonadherence. |
| Watanabe et al., 2022. [41] Extracting Multiple Worries from Breast Cancer Patient Blogs: Infodemiology Study of Blogs | Quantitative | Blog posts by patients with breast cancer in Japan | 2,272 blog posts.CAT: Strength=Moderate; Quality = Medium | Results helpful to identify worries and give timely social support. | BERT (context-aware NLP) | Concerns of patients change over time; a potential physician factor that may influence treatment nonadherence. |
| Cercato et al., 2021. [42] Narrative Medicine: feasibility of a digital narrative diary application in oncology | Qualitative (focus groups; thematic qualitative analysis) | National Cancer Institute (Rome) | 31 cancer patients.CAT: Strength = Weak; Quality = Medium | Digital narrative medicine could improve oncologist relationship with greater patient input. | Narrative prompts for patients | Lack of patient-centred care; therapeutic alliance will promote adherence and improve treatment concordance; neglect could result in unintentional nonadherence. |
Table 3.
Summary of cancer patient studies (Part 3 of 4)
| Author & Title | Method | Data Sources | Sample | Results | NLP Technique | Nonadherence/ Inference |
|---|---|---|---|---|---|---|
| Vehviläinen-Julkunen et al., 2021. [43] Experience of Ambulatory Cancer Care. Understanding Patients’ Perspectives of Quality Using Sentiment Analysis | Mixed methods qualitative analysis (survey sentiment + focus groups) | National Cancer Patient Survey data; focus groups | 92 participants (>65 years avg) and 7 focus groups (31 patients).CAT: Strength=Moderate; Quality = Medium | NLP automated sentiment analysis supported with focus groups informed the initial thematic analysis. | Automated sentiment analysis algorithm + focus groups | Communication is vital to quality of care (and in enhancing treatment adherence); not actively soliciting patient feedback could result in nonadherence. |
| Law et al., 2021. [44] Voice Analysis of Cancer Experiences among Patients with Breast Cancer: VOICE BC | Observational (voice/text analysis) | Online breast cancer forums | ∼15,000 posts; 3,906 unique users.CAT: Strength=Moderate; Quality = Medium | Engagement scores ranked relationships with HCPs as high; information needs are extremely high. | Lexicon-based analysis | Lack of information may result in unintentional treatment nonadherence; emotional needs may be of greater concern than informational needs. |
| Yerrapragada et al., 2021. [45] Machine Learning to Predict Tamoxifen Nonadherence among US Commercially Insured Patients with Metastatic Breast Cancer | Machine learning (insurance claims; population-based) | Commercial claims & encounters; Medicare claims | 3,022 breast cancer patients.CAT: Strength=Moderate; Quality = High | 48% of patients were tamoxifen nonadherent. | Algorithms trained to predict nonadherence from claims features | High rates of nonadherence confirmed via ML; results correlate with traditional surveys. |
| Moraliyage et al., 2021. [46] Cancer in Lockdown: Impact of the COVID-19 Pandemic on Patients with Cancer | Mixed methods (Quant ML / Qual NLP) | Online support groups; Twitter | 2,469,822 tweets and 21,800 patient discussions.CAT: Strength=Moderate; Quality = Medium | Cancer patient information needs, expectations, mental health, and emotional wellbeing states can be extracted. | PRIME on Twitter; machine learning algorithms | Fear underestimated in traditional surveys; may give rise to unintentional treatment nonadherence. |
| Balakrishnan, 2021. [47] Deep learning-based analysis of sentiment dynamics in online cancer community forums | Quantitative | Breastcancer.org (3 OHS forums) | 150,000 posts.CAT: Strength=Moderate; Quality = Medium | Deep learning more effective than machine learning. | Co-training: word embedding & sentiment embedding; domain-dependent lexicon | Patients need current information; emotions highest during the treatment phase; information needs change along the disease trajectory. |
| Shah et al., 2021. [48] What Patients like or dislike in physicians: Analysing drivers of patient satisfaction and dissatisfaction using a digital modelling approach | Quantitative | National Health Service subsidiary website | 53,724 online reviews of 3,372 doctors.CAT: Strength=Moderate; Quality = Medium | Unstructured text mining identified key topics of satisfaction and dissatisfaction. | Sentic-LDA topic model; text mining | Functional quality (communication; waiting times) may outweigh empathy; attitude & communication dominate dissatisfaction. |
| Arditi et al., 2020. [49] Computer-Assisted Textual Analysis of free-text comments in the Swiss Cancer Patient Experiences (SCAPE) survey | Cross-sectional survey (free-text comments) | Swiss Cancer Patients survey | 844 patient comments.CAT: Strength=Moderate; Quality = Medium | Free text allows patients greater expression “in their own words”; enhances patient-centred care. | Computer-assisted textual analysis; manual expert corpus formatting | Poor communication and lack of information most common; loneliness emerges as hidden factor—unmet support need. |
Table 4.
Summary of cancer patient studies (Part 4 of 4)
| Author & Title | Method | Data Sources | Sample | Results | NLP Technique | Nonadherence/ Inference |
|---|---|---|---|---|---|---|
| Adikari et al., 2020. [50] Can online support groups address psychological morbidity of cancer patients? An AI-based investigation of prostate cancer trajectories | Quantitative / Qualitative | Conversations in ten international OCSGs | 18,496 patients; 277,805 conversations.CAT: Strength=Moderate; Quality = Medium | Patients joining pre-treatment had improved emotions; long-term participation increased wellbeing; lower negative emotions after 12 months vs post-treatment. | Validated AI techniques and NLP framework | Most patients sought treatment information initially; transitioned to emotional support over time. |
| Mikal et al., 2019. [51] Codifying Online Social Support for Breast Cancer Patients: Retrospective Qualitative Assessment | Qualitative | 30 breast cancer survivors; ∼100,000 lines of data.CAT: Strength = Weak; Quality = Medium | Coding schema identified social support exchange at diagnosis and transition off therapy; social media support buffers stress. | Systematic coding (retrospective) | Emotional support prioritized over informational support; greater focus on emotional support may enhance adherence. |
Table 5.
Key patient side themes and prevalence.
| Theme | % of selected sources |
|---|---|
| Unmet emotional needs (distress, fear, sadness, disgust, surprise) [15,17,23,24] | 41% |
| Suboptimal information and communication (conflicting/insufficient info; perceived bias) [21,24,25] | 50% |
| Concordance within PCC unclear (goal alignment, shared decision making indicators limited) [26,27,29] | 55% |
| Online misinformation dynamics / perceived clinician bias [24,25,38] | (subset; qualitatively frequent) |
Note: Percentages reflect proportions reported in the master review’s patient voice subset; they derive from instances/inferences across included studies (see Table 1 for study characteristics).
Table 6.
Emotion signals, likely behaviors, and concordance oriented responses
| Emotion signal | Likely behavior | Concordance oriented response |
|---|---|---|
| Fear/ anxiety | Delay, dose skipping | SDM Team talk: acknowledge fear; distress screen; Option talk: clarify risks; Decision talk: values clarification. |
| Sadness/ hopelessness | Withdrawal from self care | Psycho-oncology referral; follow up within 72 h; problem solving supports. |
| Disgust (AEs) | Refusal/cessation | AE management options; normalize toxicity; reframe goals. |
| Confusion/ surprise | Inconsistent adherence | Teach back; simplified plan; bilingual materials. |
| Positive emotions | Sustained engagement | Reinforce self efficacy; document concordance; milestone planning. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



