
Submitted:
22 August 2025
Posted:
26 August 2025
You are already at the latest version
Abstract
Adolescent pregnancy remains a significant global public health issue, particularly in low- and middle-income countries, and is associated with health, social, and economic challenges for both mothers and children. Although parenting programs improve outcomes globally, there is a critical gap in tailored interventions for adolescent parents. This mixed methods systematic review aimed to address these gaps by conducting a global search of parenting programs designed or adapted for adolescent parents and making recommendations for future intervention development and research. The review examined participant characteristics, program characteristics and components, intervention results, and study quality. Thirty-six studies published between 2010 and 2024 were included, representing 34 unique samples. Most studies were from high-income countries, limiting generalizability, and only nine were rated as high-quality. Existing programs were almost entirely face-to-face, highlighting a gap in hybrid or app-based delivery. Additionally, there was a substantial lack of qualitative research exploring adolescent parenting needs and experiences. Overall, the findings indicate an urgent need for further development and evaluation of parenting programs for adolescents, particularly those implementable in low-resource settings, and for improved research quality to build an evidence base for effective, scalable interventions for this vulnerable population.
Keywords:
adolescent parents
; intervention
; mixed methods
; parenting program
; systematic review
Introduction
Adolescent pregnancy, defined as pregnancy in youth aged 13 to 19 years old, is a significant global public health issue (WHO, 2024). It is estimated that approximately 11% of global births annually are from mothers aged between 15 and 19 years old, with 95% of these births taking place in low- and middle-income countries (Abebe, 2020; WHO, 2012). Adolescent motherhood increases the risk of birth-related complications, maternal and neonatal mortality, repeat pregnancies, intimate partner violence, and sexually transmitted infections (Govender et al., 2019; Nyemgah et al., 2024; UNFPA, 2022). According to the World Health Organization (WHO, 2014), pregnancy and childbirth complications are the second-leading cause of death among women in this age group worldwide.
Low socioeconomic status, gender inequality, and young age put adolescent mothers and their children at risk for multiple deprivations and lifelong poverty (Kilburn et al., 2020). However, many adolescent mothers and their children fall into a service gap in health, social security, and educational sectors, as well as in their communities, due to a lack of age-appropriate engagement and retention strategies or tailored services (Li et al., 2020; Sewpaul, 2023). Despite the limited services tailored to adolescent parents and their children, adolescent parenthood is a key point for engagement with health and support services. Recruiting adolescent parents for parenting programs during prenatal clinic visits or child immunisation clinic visits could provide an opportunity to integrate parenting interventions with health care (Save the Children, 2022).
Global Evidence for Parenting Programs
Parenting programs are structured interventions designed to support caregivers in raising their children in healthy, safe, and developmentally appropriate ways (Barlow & Coren, 2018). They may be targeted to a particular parenting group or to a particular stage of child development. These programs are typically grounded in psychological, educational, or public health principles and aim to strengthen parenting skills, improve parent-child relationships, and promote child well-being. They might be delivered one-on-one in home settings or in groups in community or hospital settings. There is substantial global evidence on the effectiveness of parenting programs for advancing child, parent, and family health and well-being in the general population (e.g., Barlow & Coren, 2018; Burkey et al., 2018; Jeong et al.,. 2021; Knerr et al., 2013; McCoy et al., 2020). Positive parenting outcomes include a reduction in parenting stress and better social-emotional functioning, while positive child outcomes include improved emotional and behavioural functioning (Barlow & Coren, 2018; Burkey et al., 2018; Jeong et al., 2021; Knerr et al., 2013; McCoy et al., 2020). There are now hundreds of trials on parenting programs, which find that parenting programs are beneficial in improving child and parent outcomes (Kaminski et al., 2008; Leijten et al., 2022; Melendez-Torres et al., 2019; WHO, 2023).
Parenting programs have some common components, including supporting parents to notice and reinforce positive child behaviors; use consistent, non-violent discipline; be sensitive and responsive in parent-child interactions; be understanding, naming and validating child expressions of emotion; practice and model key parenting skills such as through role-plays and home activities, and build parenting confidence (England-Mason, et al., 2023; Jeong, et al., 2021; Leitjen et al., 2019). These elements, often grounded in social-learning and attachment theory, are consistently linked to better child outcomes across behavior, emotional health, cognition, and attachment (Leitjen, et al., 2019). In practice, successful programs combine multiple components (e.g., blending play/learning activities with behavior management training) tailored to child age and family context. The strongest evidence comes from multi-year randomized controlled trials (RCTs) of manualized programs, but systematic reviews of the parenting program literature suggest the techniques themselves – rather than any one branded curriculum – are what drive successful family outcomes (Jeong, et al., 2021).
Due to evidence of their effectiveness, parenting programs have received international attention and calls to action from organizations such as the WHO. For instance, the multi-agency INSPIRE: Seven Strategies to End Violence Against Children and the recently published WHO Guidelines on Parenting Interventions to Prevent Maltreatment and Enhance Parent-Child Relationships with Children 0-17 Years recommend parenting programs as a key strategy to prevent child abuse (WHO, 2016, 2023). While there is plenty of evidence that programs are beneficial for parents and their children, the evidence base on parenting programs targeted at adolescent parents is more limited. In particular, there appear to be fewer programs specifically designed or tailored to address the specific, age-appropriate parenting needs of adolescent parents and their children, and fewer studies investigating the effectiveness of these interventions (Barlow et al., 2011).
Parenting Programs for Adolescent Parents
Adolescence is a phase of ongoing brain maturation, identity formation, and emotional development (Arain et al., 2013), meaning adolescents are growing and developing in ways that adult parents are not. As a result, general adult-focused programs are often ill-suited for them (Harding et al., 2020). Parenting during adolescence adds to the developmental challenges already faced at this life stage, such as completing school and negotiating peer and romantic relationships (DeVito, 2010; (McGirr et al., 2020). Adolescent parents need emotional support, knowledge about child development, assistance in meeting their own developmental needs, and information on fostering positive relationships with the fathers of their children (DeVito, 2010).
Adolescent fathers often face stigma, marginalisation, and reduced awareness of support services (McGirr et al., 2020). Engaging adolescent fathers is critical, as father involvement positively impacts child cognitive and social-emotional development (Henry et al., 2020). For example, fathers who attend the first antenatal clinic appointment are more likely to remain engaged in their child’s life and to support the mother and child financially (Steventon-Roberts et al., 2025).
Children of adolescent parents also face poorer outcomes compared to those of older parents. Studies have found that they are more likely to experience lower cognitive development, difficulties with school progression, reduced long-term economic outcomes (Cresswell et al., 2022; Jutte et al., 2010; Lee et al., 2020), higher risks of unemployment, school dropout, criminal offences, and young parenthood themselves (Jaffee et al., 2001). Additionally, they are more likely to have poor access to food and food diversity and to experience more frequent hospitalisation.
The bio-medical challenges of pregnancy and childbirth for adolescents are generally well acknowledged, and interventions exist to support pregnant adolescents (e.g., Harding et al., 2020). However, very few postpartum programs are available for adolescent mothers and their children, although they face unique risks and challenges not experienced by older mothers. Parenting programs that specifically address the context, needs, and challenges of adolescent parents are needed.
There is only one prior synthesis of parenting programs for adolescent parents in the academic literature. A systematic review and meta-analysis by Barlow et al. (2011) found eight studies reporting on individual- and group-based parenting programs for adolescent parents investigated via RCTs. Of the eight studies, two were conducted in Canada and six were conducted in the United States (Barlow et al., 2011). The systematic review found that parenting programs can improve parental responsiveness to the child and infant responsiveness to the mother in both the short and long term. However, a substantial amount of the data from the trials could not be included in the analyses, including outcomes measured at different timepoints and lack of consistency in outcome measures (Barlow et al., 2011).
As a result, there are several gaps in the academic literature on parenting programs for adolescent parents that need to be addressed. The only published systematic review synthesizes only RCTs. While they are recognized as the gold standard for establishing efficacy, they lack understanding of real-world effectiveness, implementation and contextual relevance, particularly in resource-scarce settings. A review of other quantitative designs, such as the results of pre-post studies, as well as qualitative designs that illuminate parent and provider perspectives on these programs, is missing. Policymakers and practitioners need more than proof of efficacy. For instance, details on the characteristics of existing programs would be valuable in creating new programs. Further, policymakers and practitioners need to know how programs can be delivered effectively, with fidelity and acceptability. Additionally, the Barlow (2011) review included papers only up to 2010 and is in need of updating to gather an understanding of what parenting programs have been delivered for adolescent parents in the last 15 years and the evidence on their effectiveness.
Current Study
This mixed methods systematic review aimed to address the gaps in our knowledge of parenting programs designed or adapted for adolescent parents aiming to improve adolescent parenting attitudes, practices, knowledge skills, and or well-being. The programs need to be designed or adapted for adolescent parents. Many programs included child outcomes such as promotion of well child visits, reduction in maltreatment, improved cognitive or behavioural outcomes. When included this formed part of our outcomes framework but they were not an essential criteria. As we expected the results to be limited, we were more likely to be inclusive than exclusive, in the hopes of garnering any relevant evidence. By conducting a global search of studies published in any language with any parenting outcomes including the adolescent, the adolescent and her child, and the child. Any setting and intervention format were included. We did not place restrictions on the characteristics of the adolescent however we noted this in order to comment on generalisability. This review aimed to answer the following research questions:
(1) According to the academic literature, what parenting programs are available to adolescent parents globally?
(2) What are the characteristics and components of these programs?
(3) What are the characteristics of adolescent parents participating in these programs?
(4) How have parenting programs for adolescent parents been evaluated, and what are the results?
(5) What is the quality of the academic literature?
Method
Study Design
The plans for this study were pre-registered on the International Prospective Register of Systematic Reviews (Martin, et al., 2024). There are three differences between the protocol and how we carried out the study. First, while we planned to conduct a qualitative meta-synthesis, there was an insufficient number of qualitative papers arising in the review to conduct such an analysis. Second, while we planned to screen the articles included in Murphy et al.’s forthcoming qualitative systematic review of the parenting program literature globally, this review was not far enough along for us to incorporate in the present review. Finally, we added the fifth research question to describe the quality of academic literature, rather than setting an exclusion metric for papers that did not meet specific metrics.
Search Strategy
A search string was developed for six electronic bibliographic databases: Academic Search Complete (EBSCOhost), MEDLINE (Ovid), PsycINFO (Ovid), CINAHL, Embase (EBSCOhost), and ERIC (EBSCOhost). This search string was developed by a team of researchers with experience conducting searches on parenting programs. A librarian was also consulted. The resulting search string was adapted for each database (see Supplementary File 1). The search was implemented in the six databases without language and geographic restrictions. However, the date of publication was limited to January 1, 2010, to the date of the searches, which were conducted in May of 2024; as a follow-on to the previous systematic review on this topic (Barlow et al., 2013). As all published works included in electronic bibliographic databases have an English language abstract, we did not limit the search by language so that we could include and review any relevant abstracts. We also conducted backward citation tracking using the reference lists of included studies as well as forward citation tracking using Google Scholar. After removing duplicates, the articles found were uploaded to Covidence software for screening (Covidence, 2024).
Study Selection, Data Extraction, and Analysis
To be included in the review, articles must have reported on a parenting program specifically designed or adapted for and delivered to adolescent mothers and/or adolescent fathers before and/or after pregnancy. Adolescent parents were defined as those younger than 20 years old, in alignment with the WHO definition of adolescence (WHO, INSERT). Articles must have reported a mean parent age of under 20. Programs must have focused on improving parenting attitudes, practices, knowledge, skills, and/or well-being. Program topics were categorised as 1. child maltreatment; 2. positive parenting strategies; 3. parent-child attachment or bonding; 4. Program outcomes included all listed parenting outcomes for parents and/or children; 5. positive parent-child relationships and interactions; 6. parent mental health; 7. child development; 8. parent health and wellbeing. Programs narrowly focusing on specific child risks (e.g., poisoning, accidents) or on skills training for specific medical conditions, physical disabilities, and care for neonates (the first 6 weeks) were not included. Programs primarily aiming to deliver financial support, such as conditional cash transfer programs, were excluded. Programs could be delivered in any format, such as to individuals, groups, hybrid, online, home visiting, resource kits, and the like. Finally, articles were only included if they were academic publications, including peer-reviewed articles and theses/dissertations, reporting on primary research using any method. Systematic reviews were saved for the purpose of hand searching but were not included in the final count of included studies.
The review’s main outcomes are the characteristics and components of parenting programs for adolescent parents; the characteristics of adolescent parent participants and the evaluation; and results of evaluations or research on these programs. Regarding the characteristics and components of parenting programs, the Template for Intervention Description and Replication (TIDieR) (Hoffman, 2014) was drawn upon to extract information about the characteristics and components of parenting programs - including the study authors, country of program delivery, program name, program rationale, procedures, modes of delivery (group, individual hybrid), location (online, in-person, hybrid), number of sessions, length of delivery, and parenting techniques taught. Regarding the characteristics of adolescent parent participants, data were extracted on parent gender, average parent age, parent age range, parent socioeconomic status, parent ethnicity, and parent sample size. Information on the studies was also extracted including outcomes of interest, study method, level of prevention (universal, selective, indicated, treatment), and main study findings and conclusions.
The quality of each included study was assessed and summarized by the first and third author. Both authors assessed all papers and resolved conflicts verbally. When they were unable to come to an agreement the other authors were consulted. Quality was assessed using a modified version of the Mixed Method Appraisal Tool (MMAT), version 2018 (Nha Hong et al., 2018). The MMAT offers two screening questions -S1. Are there clear research questions? S2. Do the collected data address the research questions? We did not exclude studies based on these questions (Nha Hong et al., 2018). We also added two screening questions pertinent to replication and development of new interventions: S3. Is the description of the method sufficient to allow replication? S4. Does the intervention have sufficient standardisation to enable replication (is it manualised)? These questions were specific to our intention to be able to make informed recommendations about adolescent parent interventions. Beyond the screening questions, the MMAT has a range of questions that are explained in detail and selected depending on the type of methodological approach being assessed. A score out of 5 was then calculated.
Coder Inter-Rater Reliability
Prior to conducting screening, coders pilot tested screening at all stages and worked to establish reliability. At the title/abstract stage, coders must have met 90% agreement prior to screening independently. At the full-text stage, all articles were screened by two coders. Initial data extraction was completed using two Artificial Intelligences (AIs) - Claude AI and ChatGPT 4.0. Extracted data were crosschecked by the first author to ensure convergence, compiled by the third author, and final checks were completed by the first author. The AI extraction had a 100% convergence. The first author confirmed the AI extractions. Gaps in content were hand searched by the first and third authors and any conflicts were resolved verbally between the two authors.
Results
The systematic search identified 11,814 articles, of which 3,282 duplicates were removed. After screening the titles and abstracts of 8,532 studies, 150 were selected for full-text review. Following this, 34 studies were included. Forward and backward citation tracking led to the inclusion of a further two papers, bringing the total to 36. A PRISMA flow diagram summarizing the study selection process is provided in Figure 1.
- 1.
- What Programs are Available?
There were 29 unique programs described in the selected studies with multiple papers from several parenting programs, including Promoting Responsiveness, Emotional Regulation and Attachment in Young Mothers and Infants (PRERAYMI), (Riva Crugnola et al., 2016 & 2021); Primerios Laços (Fatori et al., 2020 & 2021; Alarcão, 2021); Steps Towards Effective Enjoyable Parenting (STEEP-b), (Firk et al., 2021; Suess et al., 2016); Family Nurse Partnership (FNP), (Cavallaro et al., Paine et al., 2020, Robling et al.,. 2016); and The Baby Elmo Program (Barr et al., 2011 & 2014). The interventions were almost all either designed specifically for adolescent parents, with one adapted for adolescent parents (Valades et al., 2021).
Eighteen interventions were universal, generally targeting adolescent mothers or couples. Six interventions were selective, targeting parents with specific risk factors including poverty (Fatori et al., 2020; Barr et al., 2011 & Alarcão et al., 2021); incarcerated fathers (Fatori et al., 2021 & Williams et al., 2013); low income (Demeusy et al., 2021); and school dropout and unemployment (MacKinnon, 2014 & Tua, 2018). Two programs were indicated as parents had a concern about their child’s behaviour (Long, 2018) or the child welfare system had a concern about family functioning (Hasani et al., 2024). One program was a treatment intervention for families under contract with the child welfare system (Hubel et al., 2019). Four programs did not provide sufficient detail to assess their prevention level. These results are presented in Table 1.
- 2.
- What are the characteristics and components of these programs?
The programs draw on a range of theoretical models, predominantly attachment theory aimed at fostering positive parent-child interactions or maternal sensitivity and decreasing child maltreatment in at-risk populations.
Delivery modes predominantly involved in-person sessions (n=20), with three programs offering a hybrid in-person and online model, (Elliot, 2020; Hasani et al., 2024; Hans et al., 2013) and four offering in-person, group sessions (Berry et al., 2022; Bohr et al., 2014; Kachingwe et al., 2021; Mackinno et al., 2014). Venues for in-person sessions included the home, community settings, juvenile detention facility, school and the hospital or a combination of these.
The timing of intervention delivery varied covering prenatal, perinatal, and postnatal periods. Session frequencies ranged from weekly to biweekly or monthly, reflecting the tailored nature of these initiatives to meet the developmental needs of adolescent parents and their children. Sessions were delivered over eight to 64 weeks (see Table 1).
- 3.
- What are the characteristics of adolescent parents participating in these programs?
The range of adolescent parent participants was between 12-23 years however, the average age of recruited parents was 17 years and 7 months. Children, when included in the program, ranged in age from 0 to 7 years, with most studies focusing on the earliest years of life. Almost all studies focused on mothers; however, study focused on incarcerated fathers, (Barr et al., 2011; Barr et al., 2014) and three studies included both mothers and fathers (Hasani et al., 2024; Rispoli & Sheridan, 2017; Florsheim et al., 2012).
Most studies (n = 27) were conducted in high-income countries. Eighteen studies were from the USA, and participants tended to include racial minorities, predominantly African American and Latino. Eight studies were from low- and middle-income countries: Brazil, South Africa, Thailand, Malawi, Russia, Iran, Indonesia, and El Salvador. A summary of the participants and their country of origin and ethnicity is included in Table 2.
- 4.
- Study Methods and Results
Program methods and results are summarized in Table 3. Out of the 36 included studies, one used a qualitative design, seven used mixed methods, eight used RCTs (generating 10 papers), 16 used other quantitative designs, and two were descriptive.
Child outcomes measured included attachment and bonding (n=4); emotional and behaviour development (n=4); social development and interaction quality (n=3); cognitive and physical development (n=3); health and safety outcomes (n=3); home environment quality (n=1); and welfare and protection outcomes (n=2). Parent outcomes measured included parenting skills and behaviour (n=9); parenting sensitivity and attunement (n = 10); and parent-child interaction quality (n=3). Other parent outcomes included psychological well-being consisting of self-esteem and parenting stress (n=5); maternal depression (n=4); and parenting confidence and attitudes (n=8).
Eight RCTs reported positive effects, two reported mixed effects, and two had a null effect. The RCTs for Primeiros Laços (Alarcão et al., 2021; Fatori et al., 2020 & 2021), Family Spirit Program (Barlow et al., 2015), Thula Sana (Valades et al., 2021), Thrive - Healthy Families Massachusetts, (McKelvey, 2012), and the Office of Adolescent Pregnancy Programs (Cox et al., 2019) showed positive benefits for mother-infant attachment, infant self-regulation, reduced parenting stress, and improved parenting confidence. The Chicago Doula Project (Hans et al., 2013) showed initial positive effects for parent-infant interactions, parenting attitudes and parenting stress, but these were not sustained beyond the life of the program. The RCTs indicated no benefit from the FNP on a variety of measures (Paine et al., 2020 & Robling et al., 2016); or for STEEP-b (Firk et al., 2021 & Suess et al., 2016) on emergency attendance or maternal sensitivity and non-intrusiveness.
Twelve quantitative studies reported positive effects, four reported mixed results and one reported no effect for the FNP, as noted above (Cavallaro, 2023). Five mixed methods papers reported positive effects and three reported mixed results. The one qualitative paper reported positive results. Program study method and results are reported in Table 3.
Study Quality
The 36 included studies were published between 2010 and 2021 representing 34 unique samples (three papers were generated from the same sample; Alarco et al., 2021, Fatori et al., 2020 & Fatori et al., 2021). Sample sizes ranged from one (Barr et al., 2011) to 130,415 (Cavallaro et al., 2023). Slightly over 25% (n = 10) of studies were small pilots with sample sizes less than 40 (Barr et al.l, 2011; Bohr & BinNoon, 2014; Elliot, 2020; Hasani et al., 2024; MacKinnon, 2014; McHugh et al., 2017; Rispoli & Sheridan, 2017; Stiles et al., 2010; Williams et al., 2013).
The MMAT results are represented in Table 4. The nine studies that met all screening criteria and scored 4/5 or 5/5 for quality are shaded for easy identification. These high-quality studies used manualized programs, which is an important factor in intervention replicability and for the further development of Parenting Interventions for Adolescents: Primeiros Laços, FNP, Thula Sana, Building Healthy Children (BHC), PRERAYMI, and The Baby Elmo Program.
Half of the papers did not meet one or more quality screening criteria. Two papers did not have research questions. Eight papers had methods that did not allow them to address the research questions. Eight papers had unclear methodology that could not be replicated. Twelve papers used non-standardized or non-manualized interventions. Hence, results from these papers need to be interpreted with due caution.
The average quality score for all papers was 3/5. The single qualitative paper had no research questions and did not describe the intervention with a level of detail that would make it replicable. The 17 quantitative papers had a broad range of quality, including ratings of one through five, but in many studies (12/17) the researchers failed to implement the intervention as planned or did not report on their implementation. The 10 RCTs were generally strong across quality metrics. While these studies all had clear methodology and were likely to use standardized interventions (9/10), they often reported poor intervention adherence. No mixed methods papers had samples that were representative of their target population.
Discussion
Summary of Findings
Substantial literature exists on adolescent pregnancy, acknowledging the unique life stage of adolescence and its impact on social-emotional and physical well-being and pregnancy outcomes (WHO, 2024). There is also extensive literature on interventions to prevent pregnancies and rapid-repeat pregnancies, sufficient to complete rapid overviews of systematic reviews (Mohamed et al., 2023). To support adolescent parents, parenting programs specifically designed or adapted to meet their needs are necessary. This study conducted a systematic review of the global literature, resulting in three overarching findings.
First, there is surprisingly little literature on parenting programs specifically designed or adapted for adolescent parents. Some of the more credible programs that do exist are resource-intensive and may be impractical for implementation in resource-scarce and rural settings. For example, the BHC program requires weekly visits for up to three years (Demeusy et al., 2021).
Second, among the parenting programs that have been studied, most are for adolescent parents in high-income contexts. Parenting in urban or peri-urban middle-class suburbs is not the same as parenting in rural sub-Saharan Africa, highlighting the need for contextual adaptation. Only two studies conducted in low- and middle-income country settings had strong quality ratings: Primerios Laços in Brazil (Alarcão et al., 2021) and Thula Sana, developed in South Africa and implemented in El Salvador (Valades et al., 2021). To date, there are no studies of adolescent parenting programs that lend themselves to affordable, at-scale implementation. There is a clear gap for hybrid or app-based delivery models that could potentially achieve universal coverage while addressing affordability and scalability constraints. Furthermore, there is a substantial gap in qualitative literature to deepen understanding of adolescent parenting needs and experiences of interventions.
Third, although the evidence is limited, the available studies on parenting programs for adolescent parents are of generally low-quality, making it difficult to reliably interpret and apply the findings. Many published papers are pilots, preliminary studies, or small master’s level studies, which limits their generalizability. Strengthening research quality will be critical to developing evidence-based interventions that are feasible, effective, and scalable.
Together, the findings of this review suggest that there is an urgent need for experienced researchers to design and oversee rigorous studies that can generate reliable and generalizable results on parenting programs for adolescent parents. However, several of the programs included in this review appear promising.
Promising Programs
Despite limited literature, the systematic review found several programs that appear promising for future research and implementation These include studies with the best quality data, according to their MMAT rating, availability of manualized interventions and yielding positive outcomes- specifically Primeiros Laços, The Baby Elmo Program, PRERAYMI, BHC, and Thula Sana. As potentially promising interventions, each of these are described below.
Primeiros Laços. Primeiros Laços (Fatori et al., 2021 & 2021; Florsheim et al., 2012) was designed to promote parent-child attachments and parent self-efficacy for impoverished, adolescent mothers in Brazil. Based on attachment theory, self-efficacy theory, and bioecological development theory, the program is delivered in the home via weekly to bi-weekly sessions from pregnancy until two years after birth. In this RCT and various sub-studies, infants in the intervention condition had higher scores on the Emotional Availability Scale (EAS) than infants in the control condition. Infants showed a significant effect for expressive language development but not on other areas of development. There was a significant effect on parental well-being, and some select maternal parenting behaviours such as singing and telling stories. This intervention showed promising effects for maternal well-being, parenting behaviors, and child outcomes for the general adolescent population, although in limited areas. However, the implementation is labor intensive, requiring individual home visits over an extended period which may be difficult to implement in rural and resource-scarce settings where professional service capacity is often already compromised.
The Baby Elmo Program. The Baby Elmo Program (Barr et al., 2011 & 2014) was developed to support incarcerated fathers aged 15-18 years in the USA to build a relationship with their child under 15 months of age. It was based on Sesame Beginnings, which is a product designed to build family interactivity and encourage fathers to follow the child’s lead as it relates to interests and play. Baby Elmo participants could attend four to 10 weekly sessions delivered in the juvenile detention facility. In this mixed methods study, fathers showed significant improvements in parenting behaviors and child engagement over time, with increases in parent support and infant engagement linked to more intervention sessions while correlations highlighted strong associations between key parenting skills and outcomes. The strength of this intervention is that it is delivered in a group setting reaching multiple people at once, reducing overall cost of implementation. Baby Elmo showed positive results after only four sessions. The Sesame Beginnings products are widely and freely available; however, it is American and therefore may not translate well to other settings. Additionally, as this program was implemented in a very specific setting (prison), it is uncertain whether it is generalizable to parents who are not institutionalized.
PRERAYMI. PRERAYMI (Riva Crugnola et al., 2016 & 2021) is an Italian intervention for adolescent mothers aged 14-21 with no psychopathology or birth complications. The program, based on attachment theory, aims to improve the mother-infant relationship, increase maternal responsiveness, and promote secure attachment. PRERAYMI participants attended bi-weekly appointments for up to six months in a hospital-based setting. In two mixed methods studies, PRERAYMI participants showed significantly improved maternal sensitivity and decreased controlling styles, with positive effects on infant cooperation, reduced passivity, and increased time spent in coordinated play and affective matches, especially within the first six months, when compared to control participants. Dyads in the intervention group demonstrated greater capacity for repairing mismatches and maintaining positive interactions. Additionally, they showed increases in sensitivity to the child and overall talking to the child. As this program was implemented in an urban high-income country hospital setting, the results may not translate to rural or low- and middle-income country settings. As the main effects are seen in the first six months of this program, future research might focus on reducing dosage to improve the cost-benefit ratio of implementation.
Building Healthy Children. BHC (Demeusy et al., 2021) is a home visiting intervention for first-time mothers under 21 years in the US with no psychopathology, child protective service reports, or severe medical illness or disability. BHC is based on attachment theory and interpersonal psychotherapy and aims to improve maternal sensitivity and foster secure parent-child attachment, reducing maternal depression, and mitigating risk factors for child maltreatment and poor development outcomes. BHC participants can receive weekly visits for up to three years. In a longitudinal, quasi-experimental study, BHC participants showed significant reductions in depressive symptoms at mid-intervention, which was associated with improvements in parenting self-efficacy and stress as well as decreased child internalizing and externalizing symptoms at post-intervention. Intervention mothers exhibited less harsh and inconsistent parenting and marginally less psychological aggression. Children of parents in the intervention group also exhibited less externalizing behavior and self-regulatory difficulties across parent and teacher reports. This intervention is important in illustrating the link between maternal depression and child internalizing and externalizing symptoms. It has promising results in improving sensitive parenting and child self-regulation; however, like Primeiros Laços, the individualized and intense session input is costly and may not transfer well to low-resource, rural settings. Future research could investigate the minimum dosage while still maintaining results.
Thula Sana. Thula Sana (Valades et al., 2021) was developed in South Africa for the general mothering population. The identified study was conducted in El Salvador and cultural and contextual adaptations were made for the adolescent parenting context. Participants were predominantly rural and low-resourced adolescents, primiparous, and aged 14 -19 years with no complicating medical conditions. The program aims to promote maternal sensitivity and secure attachment based on a socio-ecological model and attachment theory. Participants received weekly home visits from late pregnancy until the child was six months, with fewer visits as the child gets older. In an RCT pilot study, Thula Sana was found to have a positive impact on maternal sensitivity, and infants showed more regulated behaviour, more attempts to restore communication, and more social and goal-directed behaviour. Unlike the home visit models for BHC and Primerios Laços described above, Thula Sana has a relatively shorter implementation period whilst still maintaining the benefits of improved maternal sensitivity and secure infant attachment, which could make it more appropriate to implement in resource-scarce settings. While it was not originally designed for adolescent parents, it seems to have translated successfully to this population. Future research could look at the longitudinal impact of this program and ascertain whether these early gains are sustained through the following child development stages.
Strengths and Limitations
This review provides a novel contribution to the literature by synthesizing published research on parenting programs designed or adapted for adolescent parents worldwide. This review found that there are few rigorous studies of parenting programs for adolescent parents worldwide, with a particular gap in low- and middle-income countries. However, this study has several limitations. First, due to the poor quality of many of the included studies, it is difficult to assess the potential and effectiveness of many of the parenting programs. As a result, rigorous research is needed in future to address these gaps in the evidence base. In particular, studies should utilize higher sample sizes and clearly report all study details (such as for intervention replicability). Second, this review focused on only academic literature published in peer-reviewed journals and theses and dissertations. As a result, this review does not provide a comprehensive picture of all the parenting programs delivered for adolescent parents worldwide or included in evaluations or research (e.g., conference abstracts, grey literature). Third, due to finding so few qualitative studies, this review was not able to conduct a qualitative meta-synthesis.
Conclusion
Parenting programs have proven to be effective in supporting families worldwide. However, there remain significant gaps in programs tailored to adolescent parents, who face unique parenting challenges thereby requiring targeted support. This review highlights these gaps and underscores the need for further research to develop and evaluate interventions that are accessible, contextually relevant, and responsive to the specific needs of adolescent parent families. Strengthening the evidence base for such interventions will be critical in informing policy and practice, ultimately improving outcomes for adolescent parents and their children globally.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Funding
For authors at the University of Cape Town - This research was funded by the UKRI GCRF Accelerating Achievement for Africa’s Adolescents (Accelerate) Hub (Grant Ref: ES/S008101/1) and the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation programme (no. 771468). For the author at the University of Alberta - This research was funded by the Community-University Partnership for the Study of Children, Youth, and Families.
Pre-registration
The plans for this study were pre-registered on the International Prospective Register of Systematic Reviews (2024 CRD42024551584)
Acknowledgements
We acknowledge the units at our universities who supported this research. The Community-University Partnership for the Study of Children, Youth, and Families; at the University of Alberta and the Centre for Social Science Research at the University of Cape Town.
Declaration of Interests
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Abebe AM, Fitie GW, Jember DA, Reda MM, Wake GE. Teenage Pregnancy and Its Adverse Obstetric and Perinatal Outcomes at Lemlem Karl Hospital, Tigray, Ethiopia, 2018. Biomed Res Int. 2020 Jan 19;2020:3124847. [CrossRef]
- Alarcão, F. S. P., Shephard, E., Fatori, D., Amável, R., Chiesa, A., Fracolli, L.,... & Polanczyk, G. V. (2021). Promoting mother-infant relationships and underlying neural correlates: Results from a randomized controlled trial of a home-visiting program for adolescent mothers in Brazil. Developmental science, 24(6), e13113. [CrossRef]
- Arain, M., Haque, M., Johal, L., Mathur, P., Nel, W., Rais, A.,... & Sharma, S. (2013). Maturation of the adolescent brain. Neuropsychiatric disease and treatment, 449-461. [CrossRef]
- Barr, R., Morin, M., Brito, N., Richeda, B., Rodriguez, J., & Shauffer, C. (2014). Delivering Services to Incarcerated Teen Fathers: A Pilot Intervention to Increase the Quality of Father–Infant Interactions During Visitation. Psychological Services, 11(1), 10-21. [CrossRef]
- Barlow, J., Smailagic, N., Bennett, C., Huband, N., Jones, H., & Coren, E. (2011). Individual and group based parenting for improving psychosocial outcomes for teenage parents and their children. Campbell Systematic Reviews, 7(1), 1-77. [CrossRef]
- Baw, A., Mullany, B., Neault, N., Goklish, N., Billy, T., Hastings, R.,... & Walkup, J. T. (2015). Paraprofessional-delivered home-visiting intervention for American Indian teen mothers and children: 3-year outcomes from a randomized controlled trial. American Journal of Psychiatry, 172(2), 154-162. doi/pdf/10.1176/appi.ajp.2014.14030332.
- Barlow, J., & Coren, E. (2018). The effectiveness of parenting programs: A review of Campbell reviews. Research on Social Work Practice, 28(1), 99-102. [CrossRef]
- Barnet, B., Liu, J., DeVoe, M., Alperovitz-Bichell, K., & Duggan, A. K. (2007). Home visiting for adolescent mothers: Effects on parenting, maternal life course, and primary care linkage. The Annals of Family Medicine, 5(3), 224-232. [CrossRef]
- Barr, R., Brito, N., Zocca, J., Reina, S., Rodriguez, J., & Shauffer, C. (2011). The Baby Elmo Program: Improving teen father-child interactions within juvenile justice facilities. Children and Youth Services Review, 33(9), 1555-1562. [CrossRef]
- Berry, L., Mathews, S., Reis, R., & Crone, M. (2022). Mental health effects on adolescent parents of young children: reflections on outcomes of an adolescent parenting programme in South Africa. Vulnerable Children and Youth Studies, 17(1), 38-54. [CrossRef]
- Bohr, Y., & BinNoon, N. (2014). Enhancing sensitivity in adolescent mothers: Does a standardised, popular parenting intervention work with teens?. Child care in practice, 20(3), 286-300. [CrossRef]
- Burkey, M. D., Hosein, M., Morton, I., Purgato, M., Adi, A., Kurzrok, M.,... & Tol, W. A. (2018). Psychosocial interventions for disruptive behaviour problems in children in low-and middle-income countries: A systematic review and meta-analysis. Journal of Child Psychology and Psychiatry, 59(9), 982-993. [CrossRef]
- Cavallaro, F., Gilbert, R., van der Meulen, J., Kendall, S., Kennedy, E., & Harron, K. (2023). Evaluation of intensive home visiting for adolescent mothers in the family nurse partnership: a population based-data linkage cohort study in England. Available at SSRN 4337372.
- Covidence systematic review software 2024). Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org.
- Cox, J. E., Buman, M., Valenzuela, J., Joseph, N. P., Mitchell, A., & Woods, E. R. (2008). Depression, parenting attributes, and social support among adolescent mothers attending a teen tot program. Journal of pediatric and adolescent gynecology, 21(5), 275-281. [CrossRef]
- Cox, J. E., Harris, S. K., Conroy, K., Engelhart, T., Vyavaharkar, A., Federico, A., & Woods, E. R. (2019). A parenting and life skills intervention for teen mothers: a randomized controlled trial. Pediatrics, 143(3). 10.1542/peds.2018-2303.
- Cresswell, L., Faltyn, M., Lawrence, C., Tsai, Z., Owais, S., Savoy, C.,... & Van Lieshout, R. J. (2022). Cognitive and mental health of young mothers’ offspring: a meta-analysis. Pediatrics, 150(5), e2022057561. [CrossRef]
- Demeusy, E. M., Handley, E. D., Manly, J. T., Sturm, R., & Toth, S. L. (2021). Building healthy children: A preventive intervention for high-risk young families. Development and Psychopathology, 33(2), 598-613. https://.
- DeVito, J. (2010). How adolescent mothers feel about becoming a parent. The Journal of Perinatal Education, 19(2), 25. [CrossRef]
- Drummond, J. E., Letourneau, N., Neufeld, S. M., Stewart, M., & Weir, A. (2008). Effectiveness of teaching an early parenting approach within a community-based support service for adolescent mothers. Research in nursing & health, 31(1), 12-22. [CrossRef]
- Elliott, C. (2020). Supporting Adolescent Mothers Using Video Interaction Guidance (VIG) (Doctoral dissertation, Queen’s University Belfast).
- England-Mason, G., Andrews, K., Atkinson, L., & Gonzalez, A. (2023). Emotion socialization parenting interventions targeting emotional competence in young children: A systematic review and meta-analysis of randomized controlled trials. Clinical Psychology Review, 100, 102252. [CrossRef]
- Fatori, D., Argeu, A., Brentani, H., Chiesa, A., Fracolli, L., Matijasevich, A.,... & Polanczyk, G. (2020). Maternal parenting electronic diary in the context of a home visit intervention for adolescent mothers in an urban deprived area of São Paulo, Brazil: Randomized controlled trial. JMIR mHealth and uHealth, 8(7), e13686. [CrossRef]
- Fatori, D., Fonseca Zuccolo, P., Shephard, E., Brentani, H., Matijasevich, A., Archanjo Ferraro, A.,... & V. Polanczyk, G. (2021). A randomized controlled trial testing the efficacy of a nurse home visiting program for pregnant adolescents. Scientific reports, 11 (1), 14432. [CrossRef]
- Firk, C., Dahmen, B., Dempfle, A., Niessen, A., Baumann, C., Schwarte, R.,... & Herpertz-Dahlmann, B. (2021). A mother–child intervention program for adolescent mothers: Results from a randomized controlled trial (the TeeMo study). Development and Psychopathology, 33(3), 992-1005. [CrossRef]
- Florsheim, P., Burrow-Sánchez, J. J., Minami, T., McArthur, L., Heavin, S., & Hudak, C. (2012). Young parenthood program: Supporting positive paternal engagement through coparenting counseling. American Journal of Public Health, 102(10), 1886-1892. [CrossRef]
- Harding, J. F., Knab, J., Zief, S., Kelly, K., & McCallum, D. (2020). A systematic review of programs to promote aspects of teen parents’ self-sufficiency: Supporting educational outcomes and healthy birth spacing. Maternal and Child Health Journal, 24, 84-104. [CrossRef]
- Govender, D., Naidoo, S., & Taylor, M. (2019). Prevalence and risk factors of repeat pregnancy among South African adolescent females. African Journal of Reproductive Health, 23(1), 73-87. [CrossRef]
- Harding, J. F., Knab, J., Zief, S., Kelly, K., & McCallum, D. (2020). A systematic review of programs to promote aspects of teen parents’ self-sufficiency: Supporting educational outcomes and healthy birth spacing. Maternal and Child Health Journal, 24, 84-104. [CrossRef]
- Hans, S. L., Thullen, M., Henson, L. G., Lee, H., Edwards, R. C., & Bernstein, V. J. (2013). Promoting positive mother–infant relationships: A randomized trial of community doula support for young mothers. Infant mental health journal, 34(5), 446-457. [CrossRef]
- Hasani, M., Maleki, A., Mohebbi, P., & Ebrahimi, L. (2024). The effectiveness of the satir approach-based counseling on the parenting sense of competence in adolescent mothers. Preventive Care in Nursing & Midwifery Journal, 14(1), 54-63. [CrossRef]
- Henry, J. B., Julion, W. A., Bounds, D. T., & Sumo, J. N. (2020). Fatherhood matters: An integrative review of fatherhood intervention research. The Journal of School Nursing, 36(1), 19-32. [CrossRef]
- Hoffmann T, Glasziou P, Boutron I, Milne R, Perera R, Moher D, Altman D, Barbour V, Macdonald H, Johnston M, Lamb S, Dixon-Woods M, McCulloch P, Wyatt J, Chan A, Michie S. (2014). Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ, 348:g1687. [CrossRef]
- Hong, Q. N., Fàbregues, S., Bartlett, G., Boardman, F., Cargo, M., Dagenais, P.,... & Pluye, P. (2018). The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Education for information, 34(4), 285-291. [CrossRef]
- Hubel, G. S., Rostad, W. L., Self-Brown, S., & Moreland, A. D. (2018). Service needs of adolescent parents in child welfare: Is an evidence-based, structured, in-home behavioral parent training protocol effective? Child abuse & neglect, 79, 203-212. [CrossRef]
- In-Iw, S., Kosolruttaporn, P., & Chuwong, T. (2017). Outcomes of Caring Teenage Mothers and Their Children in Young Family Clinic, Siriraj Hospital. J Med Assoc Thai, 100(8), 872-5. PDF available.
- Jaffee, S., Caspi, A., Moffitt, T. E., Belsky, J. A. Y., & Silva, P. (2001). Why are children born to teen mothers at risk for adverse outcomes in young adulthood? Results from a 20-year longitudinal study. Development and psychopathology, 13(2), 377-397. [CrossRef]
- Jeong, J., Franchett, E. E., Ramos de Oliveira, C. V., Rehmani, K., & Yousafzai, A. K. (2021). Parenting interventions to promote early child development in the first three years of life: A global systematic review and meta-analysis. PLoS medicine, 18(5), e1003602. [CrossRef]
- Jutte, D. P., Roos, N. P., Brownell, M. D., Briggs, G., MacWilliam, L., & Roos, L. L. (2010). The ripples of adolescent motherhood: social, educational, and medical outcomes for children of teen and prior teen mothers. Academic Pediatrics, 10(5), 293-301. [CrossRef]
- Kachingwe, M., Chikowe, I., Van der Haar, L., & Dzabala, N. (2021). Assessing the impact of an intervention project by the young women’s christian association of Malawi on psychosocial well-being of adolescent mothers and their children in Malawi. Frontiers in public health, 9, 585517. [CrossRef]
- Kilburn, K., Ferrone, L., Pettifor, A., Wagner, R., Gómez-Olivé, F. X., & Kahn, K. (2020). The impact of a conditional cash transfer on multidimensional deprivation of young women: evidence from South Africa’s HTPN 068. Social Indicators Research, 151, 865-895. [CrossRef]
- Knerr, W., Gardner, F., & Cluver, L. (2013). Improving positive parenting skills and reducing harsh and abusive parenting in low-and middle-income countries: A systematic review. Prevention science, 14(4), 352-363. [CrossRef]
- Lee, J. O., Jeong, C. H., Yuan, C., Boden, J. M., Umaña-Taylor, A. J., Noris, M., & Cederbaum, J. A. (2020). Externalizing behavior problems in offspring of teen mothers: A meta-analysis. Journal of youth and adolescence, 49, 1146-1161. [CrossRef]
- Leijten, P., Gardner, F., Melendez-Torres, G. J., Van Aar, J., Hutchings, J., Schulz, S.,... & Overbeek, G. (2019). Meta-analyses: Key parenting program components for disruptive child behavior. Journal of the American Academy of Child & Adolescent Psychiatry, 58(2), 180-190. [CrossRef]
- Leijten, P., Melendez-Torres, G. J., & Gardner, F. (2022). Research Review: The most effective parenting program content for disruptive child behavior–a network meta-analysis. Journal of Child Psychology and Psychiatry, 63(2), 132-142. [CrossRef]
- Li, Z., Patton, G., Sabet, F., Subramanian, S. V., & Lu, C. (2020). Maternal healthcare coverage for first pregnancies in adolescent girls: a systematic comparison with adult mothers in household surveys across 105 countries, 2000–2019. BMJ global health, 5(10), e002373. [CrossRef]
- Long, M. (2018). Treating at-risk adolescent mothers and their children: family therapy delivered from the theraplay® model (Doctoral dissertation, Laurentian University of Sudbury). PDF available.
- MacKinnon, L. (2014). Evaluation of a parenting skills program in Russia. International Quarterly of Community Health Education, 34(4), 313-330. [CrossRef]
- McCoy, A., Melendez-Torres, G. J., & Gardner, F. (2020). Parenting interventions to prevent violence against children in low-and middle-income countries in East and Southeast Asia: A systematic review and multi-level meta-analysis. Child abuse & neglect, 103, 104444. [CrossRef]
- McGirr, S., Torres, J., Heany, J., Brandon, H., Tarry, C., & Robinson, C. (2020). Lessons learned on recruiting and retaining young fathers in a parenting and repeat pregnancy prevention program. Maternal and Child Health Journal, 24, 183-190. [CrossRef]
- McHugh, M. T., Kvernland, A., & Palusci, V. J. (2017). An adolescent parents’ programme to reduce child abuse. Child abuse review, 26(3), 184-195. [CrossRef]
- Kelvey, L. M., Burrow, N. A., Balamurugan, A., Whiteside-Mansell, L., & Plummer, P. (2012). Effects of home visiting on adolescent mothers’ parenting attitudes. American Journal of Public Health, 102(10), 1860-1862. [CrossRef]
- Martin, M., Kruyer R., Enwedo, J., Tatham. C., Morse K. Parenting programs for adolescent parents: A systematic review of existing interventions. PROSPERO 2024 Available from https://www.crd.york.ac.uk/PROSPERO/view/CRD42024551584.
- Melendez-Torres, G. J., Leijten, P., & Gardner, F. (2019). What are the optimal combinations of parenting intervention components to reduce physical child abuse recurrence? Reanalysis of a systematic review using qualitative comparative analysis. Child Abuse Review, 28(3), 181-197. [CrossRef]
- Mohamed, S., Chipeta, M. G., Kamninga, T., Nthakomwa, L., Chifungo, C., Mzembe, T.,... & Madise, N. (2023). Interventions to prevent unintended pregnancies among adolescents: a rapid overview of systematic reviews. Systematic Reviews, 12(1), 198. [CrossRef]
- Nicolson, S., Judd, F., Thomson-Salo, F., & Mitchell, S. (2013). Supporting the adolescent mother–infant relationship: Preliminary trial of a brief perinatal attachment intervention. Archives of women’s mental health, 16, 511-520. [CrossRef]
- Nyemgah, C. A., Ranganathan, M., Nabukalu, D., & Stöckl, H. (2024). Prevalence and severity of physical intimate partner violence during pregnancy among adolescents in eight sub-Saharan Africa countries: A cross-sectional study. PLOS global public health, 4(7), e0002638. https:// doi.org/10.1371/journal.pgph.0002638.
- Paine, A. L., Cannings-John, R., Channon, S., Lugg-Widger, F., Waters, C. S., & Robling, M. (2020). Assessing the impact of a family nurse-led intervention on young mothers’ references to internal states. Infant Mental Health Journal, 41(4), 463-476. [CrossRef]
- Patton, G. C., Coffey, C., Sawyer, S. M., Viner, R. M., Haller, D. M., Bose, K.,... & Mathers, C. D. (2009). Global patterns of mortality in young people: a systematic analysis of population health data. The lancet, 374(9693), 881-892. [CrossRef]
- Rispoli, K. M., & Sheridan, S. M. (2017). Feasibility of a school-based parenting intervention for adolescent parents. Advances in School Mental Health Promotion, 10(3), 176-194. [CrossRef]
- Riva Crugnola, C., Ierardi, E., Albizzati, A., & Downing, G. (2016). Effectiveness of an attachment-based intervention program in promoting emotion regulation and attachment in adolescent mothers and their infants: A pilot study. Frontiers in Psychology, 7, 195. [CrossRef]
- Riva Crugnola, C., Ierardi, E., Peruta, V., Moioli, M., & Albizzati, A. (2021). Video-feedback attachment based intervention aimed at adolescent and young mothers: effectiveness on infant-mother interaction and maternal mind-mindedness. Early Child Development and Care, 191(3), 475-489. [CrossRef]
- Robling, M., Bekkers, M. J., Bell, K., Butler, C. C., Cannings-John, R., Channon, S.,... & Torgerson, D. (2016). Effectiveness of a nurse-led intensive home-visitation programme for first-time teenage mothers (Building Blocks): a pragmatic randomised controlled trial. The Lancet, 388(10053), 1467-1476. [CrossRef]
- Rokhanawati, D., Salimo, H., Andayani, T. R., & Hakimi, M. (2023). The effect of parenting peer education interventions for young mothers on the growth and development of children under five. Children, 10(2), 338. [CrossRef]
- Rose, S. H., Chigusa, H., Sato, A., & Saito, T. (2016). Evaluation of a school-based parenting program: The effects of a preventive intervention in Japan. Journal of Child and Family Studies, 25(9), 2817-2826. [CrossRef]
- Save the Children (2022). Promising Directions and Missed Opportunities for Reaching First-time Mothers with Reproductive, Maternal, Newborn, and Child Health Services: Findings from formative assessments in two countries. PDF available.
- Schaffer, M. A., Goodhue, A., Stennes, K., & Lanigan, C. (2012). Evaluation of a public health nurse visiting program for pregnant and parenting teens. Public Health Nursing, 29(3), 218-231. [CrossRef]
- Sewpaul, R., Resnicow, K., Crutzen, R., Dukhi, N., Ellahebokus, A., & Reddy, P. (2023). A Tailored mHealth Intervention for Improving Antenatal Care Seeking and Health Behavioral Determinants During Pregnancy Among Adolescent Girls and Young Women in South Africa: Development and Protocol for a Pilot Randomized Controlled Trial. JMIR Research Protocols, 12(1), e43654. [CrossRef]
- Roberts, K. S., Smith, C., Cluver, L. D., Toska, E., Kelly, J., Thomas, A.,... & Sherr, L. (2025). Men matter: a cross-sectional exploration of the forgotten fathers of children born to adolescent mothers in South Africa. BMJ open, 15(7), e092723. [CrossRef]
- Stiles, A. S. (2010). Case study of an intervention to enhance maternal sensitivity in adolescent mothers. Journal of Obstetric, Gynecologic & Neonatal Nursing, 39(6), 723-733. [CrossRef]
- Toska, E., Saal, W., Chen Charles, J., Wittesaele, C., Langwenya, N., Jochim, J.,... & Cluver, L. (2022). Achieving the health and well-being Sustainable Development Goals among adolescent mothers and their children in South Africa: Cross-sectional analyses of a community-based mixed HIV-status cohort. PloS one, 17(12), e0278163. [CrossRef]
- Sanders, M. R., Kirby, J. N., Tellegen, C. L., & Day, J. J. (2014). The Triple P-Positive Parenting Program: A systematic review and meta-analysis of a multi-level system of parenting support. Clinical psychology review, 34(4), 337-357. [CrossRef]
- Suess, G. J., Bohlen, U., Carlson, E. A., Spangler, G., & Frumentia Maier, M. (2016). Effectiveness of attachment based STEEP™ intervention in a German high-risk sample. Attachment & human development, 18(5), 443-460. [CrossRef]
- Tua, A. I. (2018). Social Inclusion Outcomes for an Organization’s Adolescent Parent Intervention. PDF available.
- UNFPA (United Nations Population Fund) (2022). Motherhood in childhood—The untold story: UNFPA policy brief, 27 June 2022. PDF available.
- Valades, J., Murray, L., Bozicevic, L., De Pascalis, L., Barindelli, F., Meglioli, A., & Cooper, P. (2021). The impact of a mother–infant intervention on parenting and infant response to challenge: A pilot randomized controlled trial with adolescent mothers in El Salvador. Infant Mental Health Journal, 42(3), 400-412. [CrossRef]
- Wahlen, K., & Katja, H. (2018). Preventive parenting interventions: The role of involvement and consequences for adolescent mothers’ parenting outcomes. Journal of youth and adolescence, 47(2), 377-388. [CrossRef]
- Wageman, C. M., & Buch, H. D. (2014). Maternal attitudes and health outcomes in adolescent mothers participating in a community program. Journal of clinical psychology in medical settings, 21(1), 98-106. [CrossRef]
- Williams, T. H., Dumas, B. P., & Edlund, B. J. (2013). An evidence-based parenting intervention with inner-city teen mothers. Journal of National Black Nurses’ Association: JNBNA, 24(1), 24-30. PMID: 24218870. (No doi available).
- World Health Organization. (2012). Strengthening the role of the health system in addressing violence, in particular against women and girls, and against children: Report by the Secretariat (WHA65.13). World Health Organization. PDF available.
- World Health Organization. (2016). INSPIRE: Seven strategies for ending violence against children. World Health Organization. PDF available.
- World Health Organization. (2023). WHO guidelines on parenting interventions to prevent maltreatment and enhance parent–child relationships with children aged 0–17 years. World Health Organization. PDF available.
- World Health Organization. (2024). Adolescent pregnancy. World Health Organization. PDF available.
- Williams, A. L., & Lytle, L. M. (2017). Parenting interventions for adolescent mothers: A meta-analysis. Journal of Adolescent Health, 61(4), 431-438. [CrossRef]
- Woller, D. R., Ho, K. Y., & Schultz, L. R. (2017). Understanding parenting interventions with adolescent mothers: A systematic review. Psychological Services, 14(4), 490-501. [CrossRef]
- Wyatt Kaminski, J., Valle, L. A., Filene, J. H., & Boyle, C. L. (2008). A meta-analytic review of components associated with parent training program effectiveness. Journal of abnormal child psychology, 36, 567-589. PDF available.
- Zegers, J. A., & Gragnolati, M. (2017). A systematic review of programs that promote the maternal-infant relationship in adolescent mothers. Journal of Adolescent Health, 60(5), 541-547. [CrossRef]
Figure 1.
PRISMA Flow Diagram.
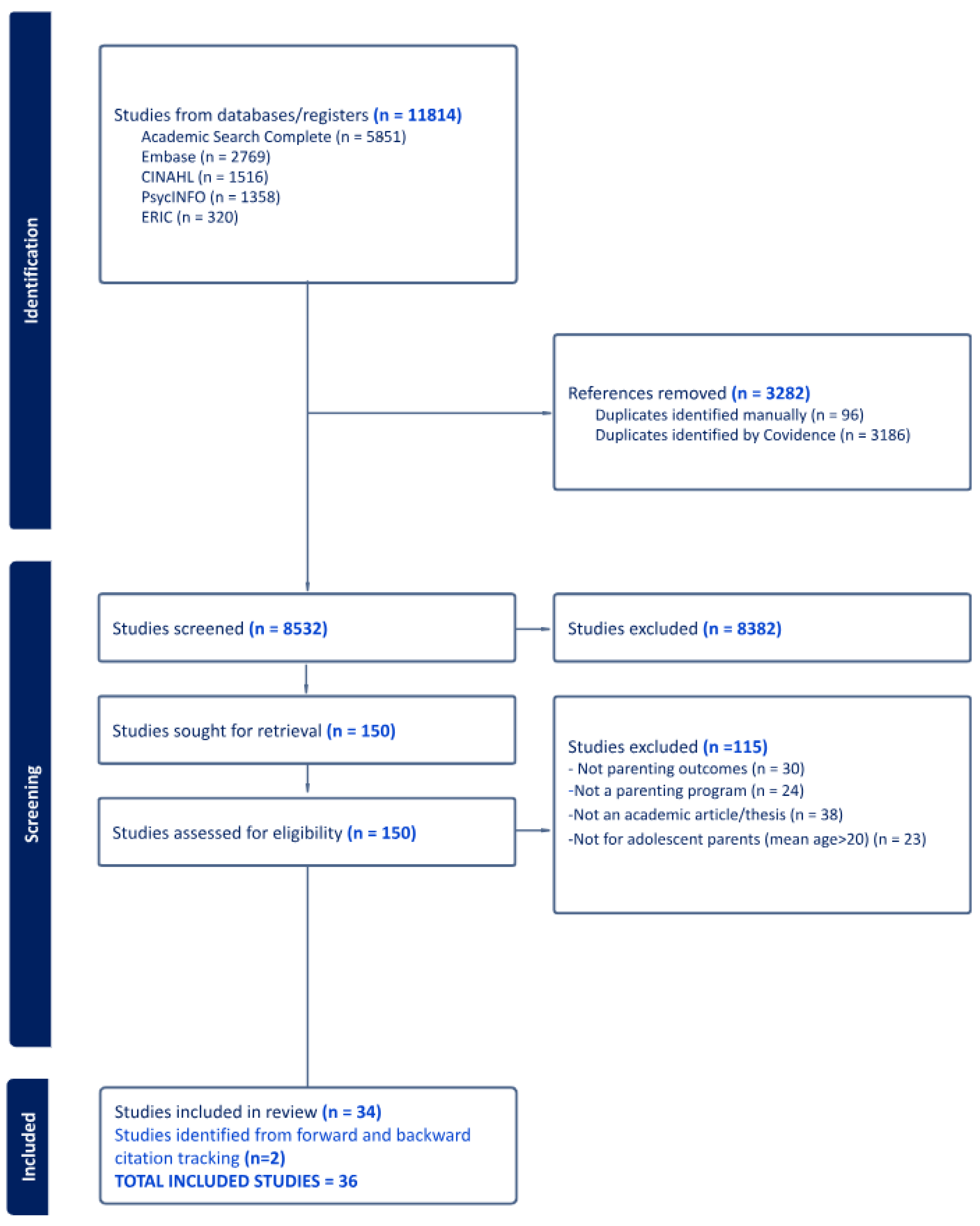

Table 1.
Description of Programs.
| Citation | Program Name | Design | Program Rationale | Parenting Topics | Program Timing | Mode | Target & Prevention Level1 | Setting | Number Sessions | Frequency | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Alarcão (2021); Fatori (2020) & Fatori (2021) |
Primeiros Lacos |
Designed for teen parents | Promotes parent-child attachments and interactions and parent self-efficacy based on attachment theory, self-efficacy theory and bioecological development theory | Mother-infant attachment relationships | During and after pregnancy (until 1 year of age) | In-person | Individual / Selective - living in poverty | Homes - Urban | 60-62 | Weekly for the first 16 weeks of pregnancy and then biweekly during pregnancy; weekly during the last month of pregnancy; monthly from 21-24 months | |
| Barlow (2013) | Family Spirit | Designed for teen parents | Promotes parent child attachments and advance social learning based on attachment theory and social-learning theory | Positive parenting strategies; parent mental health; parent knowledge and self-efficacy | During and after pregnancy | In-person | Individual / Selective- American Indian | Homes - Rural | 43 | Weekly | |
| Barr (2011) & Barr (2014) |
Baby Elmo Program | Designed for teen parents | Promotes attachment, infant exploration, and following the child’s lead among teen fathers based on Sesame Beginnings | Positive parenting strategies; parent-child attachment and interactions | After pregnancy | In-person | Individual / Selective -Incarcerated fathers | Juvenile detention facility | 10 | Weekly or bi-weekly | |
| Berry (2022) | None | Designed for teen parents | Supports parent-child interactions and attachments as well as reduce parental depression based on Bronfenbrenner’s ecological model of development | Parent attachment | After pregnancy | In-person | Group/ Universal |
Schools - Urban | 20 | Weekly | |
| Bohr (2014) | Right from the Start | Designed for teen parents | Enhances maternal sensitivity and infant attachment security by teaching specific parental skills based on the Coping Modeling Problem Solving Approach | Positive parenting strategies’ parent-attachment and bonding; positive parent-child relationships and interactions; maternal sensitivity | After pregnancy | In-person | Group/ Universal |
Community settings | 8 | Weekly | |
| Cavallaro (2023), Paine (2020) & Robling (2016) |
Family Nurse Partnership | Adapted for teen parents | Promotes reduction in child maltreatment and health and development outcomes for children through mother support through home visits from trained family nurses. | Positive parenting; parent-attachment or bonding; positive parent-child relationships and interactions; child maltreatment; child development; adolescent mother development skills; social support and social services | Early pregnancy until child’s second birthday | In-person | Individual / Universal | Home – Urban & Rural | Up to 64 |
Weekly or Bi-weekly | |
| Cox (2019) | Office of Adolescent Pregnancy Programs | Designed for teen parents | Improves teen parenting while enhancing youth and family development including positive, empathetic relationships as well as self-efficacy and self- based on Ansell-Casey Life Skills Assessment Curriculum, the Women’s Negotiation Project Curriculum for Teen Mothers, and the Nurturing Curriculum |
Positive parenting; adolescent development skills | After pregnancy | In-person | Individual / Universal | Pediatric hospital - Urban | 12 | Not reported | |
| Demeusy (2021) | Building Healthy Children | Designed for teen parents | Improves maternal sensitivity and fosters secure parent-child attachment, reducing maternal depression, and mitigating risk factors for child maltreatment and poor development outcomes, based on Child-Parent Psychotherapy (attachment theory) and interpersonal psychotherapy for adolescents. | Positive parenting; maternal mental health; child maltreatment (prevention) | After pregnancy for 3 years | In-person | Individual / Selective - low income | Homes - Urban | Unspecified number | Weekly | |
| Elliot (2020) | Video Interaction Guide | Adapted for teen parents | Enhances attuned interactions and maternal sensitivity in adolescent mothers, based on SATIR family therapy approach. | Positive parenting strategies; parent-child attachment or bonding | After pregnancy | Hybrid: in-person initially then online | Individual / Universal | Home or community, based on ppt choice | 3 cycles of recording, review and discussion | Bi-weekly | |
| Firk (2021) | Steps Toward Effective Enjoyable Parenting-Brief (STEEP-B) | Adapted for teen parents | Promotes secure parent-child attachment by enhancing sensitive parental care, parenting behaviours, and social support, based on attachment-based early intervention programs. | Positive parenting strategies | After pregnancy for 9 months | In-person | Individual / Universal | Homes | 12-18 | Monthly or bi-monthly | |
| Florsheim (2012) | Young Parenthood Program (YPP) | Designed for teen parents | Develops skills to maintain positive, supportive coparenting relationships and to create stable, nurturing environments, based on family systems theory. | Positive parenting; coparenting relationships | During pregnancy | In-person | Individual/ Universal |
Hospitals, homes, and community organizations - Urban | 10 | Weekly | |
| Hans (2013) | Chicago Doula Project | Designed for teen parents | Supports young mothers during childbirth and transition to parenting with empathetic care and understanding of the newborn. | Positive parenting strategies | During and after pregnancy to three months postpartum | In-person and via telephone | Individual / Universal | Homes and hospitals - Urban | 20-25 | Weekly | |
| Hasani (2024) | SATIR | Adapted for teen parents | Promotes parent-child attachment based on strengths-based approach. | Parent-child attachment or bonding | After pregnancy | Hybrid: first session in-person then WhatsApp | Individual/ Universal | Hospital for in-person then online | 6 | Weekly | |
| Hubel (2018) | SafeCare | Adapted for teen parents | Program for at-risk parents that aims to reduce child maltreatment recidivism by improving parent-child relationships and parent knowledge and skills. | Positive parenting strategies; positive parent-child relationships; child development; home safety; child healthcare | After pregnancy for 6 months | In-person | Individual/ Treatment - under contract with the child welfare system |
Homes – Rural and urban | 26 | Weekly | |
| In-iw (2017) | Young Family Clinic (YFC) | For teen parents | Clinic that provides a one-stop shop for teen mothers and their children with the objectives of preventing subsequent pregnancy, promoting child-rearing, and preventing child maltreatment. | Adolescent development; child development; child maltreatment | After pregnancy for 2 years | In-person | Individual/ Universal |
Hospitals | Appointments ongoing | ?? | |
| Kachingwe 2021 | Community Model for Fostering Health and Well-Being Amongst Adolescent Mothers and their Children | For teen parents | Empowers adolescent girls to prioritize the health and well-being of them and their children based on consultations with local stakeholders and a baseline needs assessment. | Positive parenting; child development; adolescent development skills | After pregnancy | In-person | Group/ Universal | Community - Rural | 36 | Two years | |
| Long (2018) | Theraplay | Adapted for teens | Promotes positive mother-child interactions in at-risk population based on Theraplay play-based, family-focused treatment grounded in attachment theory. | Parent-child attachment and bonding. | After pregnancy | In-person | Individual/ Indicated - parents have a concern in the child’s social, emotional or behavioral wellbeing | Community - Urban | 15 | Weekly | |
| Mackinnon (2014) | Pskov Positive Parenting | For teen parents | Strengthens parenting skills with the goal to prevent child abuse and neglect and to reduce the number of children abandoned to state-run orphanages. |
Positive parenting strategies | After pregnancy | In-person | Group/ Selective - dropped out of school and unemployed | Community Organization - Urban | 10 | Weekly | |
| McHugh (2017) | Bellevue Hospital Adolescent Parenting Program | For teen parents | Reduce child abuse reports and promote well-baby visits, immunizations and referrals for developmental delays in high-risk population. | Positive parenting strategies; child development; SRH and maternal education | First 12 months after birth | In-person | Individual/ Universal | Hospital - Urban | ? | Weekly | |
| McKelvey (2012) | Thrive Program | Adapted for teens | Reduces child maltreatment and improves parenting attitudes and beliefs based on Healthy Family Africa (HFA).. | Positive parenting; child development; parent health and wellbeing | From pregnancy until child’s third birthday | In-person | Individual/ Universal | Homes | ? | ? | |
| Nicolson (2013) | Adolescent Mothers’ Program: Let’s Meet Your Baby as a Person (AMPLE) | For teen parents | Aims to influence mothers’ interaction with their baby by helping them see their baby as a person from the beginning, based on attachment theory. | Parent-child attachment or bonding; positive parent-child relationships and interactions; child development | One session in late pregnancy and one after birth | In-person | First session – group; Second session - individual - Universal | Hospital | 2 | Before & after birth | |
| Rispoli (2017) | Parents Interacting with Infants – Teen Version (PIWI-T) | Adapted for teens | Teaches infant attachment, brain development, available community resources. | Parent-child attachment or bonding; positive parent-child relationships and interactions; child development; social support and social services | After pregnancy | In-person | Groups / Universal | School (daycare classroom) - Urban | 4 | Weekly | |
| Riva Crugnola (2016) & Riva Crugnola (2021) |
Promoting Responsiveness, Emotion Regulation and Attachment in Young Mothers and Infants (PRERAYMI) |
Designed for teen parents | Improves the mother-infant relationship, increase maternal responsiveness and reflectivity, and promote secure attachment between mothers and infants, based on attachment theory | Parent-child attachment or bonding; adolescent development skills; emotional regulation | After pregnancy for 6 months | In-person | Individual/ Universal | Hospital | 10- 15 | Bi-weekly | |
| Rokhanawati (2023) | Promoting First Relationship | For teen parents | Enhances maternal sensitivity through a Peer Education Program based on Social Learning Theory, Theory of Reasoned Action and Diffusion of Innovation Theory. | Positive parenting; parent-child attachment and bonding; positive parent-child relationships and interactions | After pregnancy | In-person | Individual/ Universal | Homes - Rural | 8 | Biweekly | |
| Schaffer (2012) | Home Visit Nurse Agency (MVNA) Pregnant and Parenting Teens Program | For teen parents | Promotes family and child health and family self-sufficiency through mentoring. | Positive parenting strategies; parent mental health; adolescent development skills | From pregnancy until two years old | In-person | Individual/ Universal | Home or other safe community setting- Urban | 16 |
Monthly | |
| Stiles (2010) | Promoting First Relationships Intervention | For teen parents | Promotes maternal sensitivity towards child, based on Barnard’s model of maternal/infant relationships. | Positive parenting strategies; parent-child attachment or bonding; positive parent-child relationships and interactions | After pregnancy | In-person | Individual / Universal |
Home - Rural | 8 |
Bi-weekly | |
| Suess (2016) | Steps Towards Effective and Enjoyable Parenting (STEEP) | Adapted for teen parents | Promotes secure attachment and maternal sensitivity, based on attachment theory and video feedback. | Parent-child attachment or bonding; adolescent development skills (social support) | Child aged 12-24 months | In-person | Individual & Group/ Indicated - within the Child Welfare System | Home & Community | 30 home visits; 12 video interventions; 4 family/ friends nights; 2 outings | Weekly | |
| Tua (2018) | Family Incubator Model | For teen parents | Promotes social inclusion based on complex systems theory. | Positive parenting strategies; adolescent development skills | Unspecified | In-person | Individual & Group/ Selective - without a high school diploma | Home & Community -Urban | Unspecified | Unspecified | |
| Valades (2021) | Thula Sana | Adapted for teen parents | Promotes maternal sensitivity and infant secure attachment based on socio-ecological model and attachment theory. | Positive parenting strategies; parent-child attachment or bonding | Late pregnancy to 6 months old | In-person | Individual/Universal | Home - Rural | 16 | Weekly until 2 months, bi-weekly until 4 months, monthly until 6 months | |
| Williams (2013) | Incredible Years Program (IYP) | Adapted for teen parents | Improves effective parenting skills through interactive play, parenting skills, problem solving-skills and non-violent discipline, | Child maltreatment prevention; positive parenting strategies; parent-child attachment or bonding; child development | After pregnancy | In-person | In-Person Group/ Universal | School - Urban | 8 | Weekly | |
1 Prevention levels: universal – any adolescent parent or adolescent parents without additional risks; selective – specific groups identified at-risk (beyond the risk that exists with being an adolescent parent); indicated – at-risk families demonstrating signs of dysfunctional parenting or dysfunctional child behaviour; treatment - targets reported abuse or dysfunctional parenting
Table 2.
Description of Participants.
| Citation | Country | Parent age, average (range) | Gender | Ethnicity | Child age range | Study Inclusion/Exclusion |
|---|---|---|---|---|---|---|
| Alarcão (2021) Fatori (2020) & Fatori (2021) |
Brazil | 17.11 (14 - 19 ) | Female | 31.3% White (only explicitly reported ethnicity breakdown) | 6-24 months | Adolescent mothers aged 14–19 years, First pregnancy, 8–16 weeks gestation, Low socioeconomic status (classified as classes C/D/E according to the Brazilian classification system, ABEP, 2007), Living in impoverished urban areas of São Paulo, Brazil. |
| Barlow (2013) | USA | 18.12 (12–19 ) | Female | American Indian (self-identified) | birth - 12 months | Pregnant and ≤32 weeks' gestation, 12–19 years of age at conception, American Indian (self-identified), and residing in one of four participating reservation communities. |
| Barr (2011) | USA | 17.1 (15 - 18 ) | Male | Fifteen of the 20 teen participants were Hispanic; four were African-American and one was of mixed racial descent. | 6-36 months | Teen fathers aged 15 to 18 years incarcerated in juvenile detention facilities. Fathers had to have children between the ages of 6 to 36 months.Participation was voluntary, and fathers needed to complete at least 4 out of 10 sessions of the Baby Elmo Program to be included in the final analysis. |
| Barr (2014) | USA | 16.89 ()i | Male | 66.19% Hispanic, 22.22% Black, 9.52% Mixed, and 1.59% White. | birth to 15 months | Incarcerated teen fathers with an infant under 15 months of age at enrolment. No direct involvement with child protection services for the target infant or any other infant. Consent from the caregiver to bring the infant into the facility to participate in the study. |
| Berry (2022) | South Africa | 16.38 (12-22) | Female | Peri-urban settlements near Cape Town metropole (Gugulethu, Khayelitsha, and Nyanga), which are predominantly populated by Black African communities. | 0-24 months | Adolescents aged 12-22 years. Participants had to have parental responsibility for at least one child and had substantial time spent on parenting duties. This included both biological and non-biological parents (e.g., siblings or relatives caring for children). Participants were recruited from three secondary schools in Cape Town. Self-selection: Adolescents self-selected into the parenting program. Exclusion: Grade 12 learners (final year of secondary school) were excluded from the study. |
| Bohr (2014) | Canada | 18.54 (17-22 ) | Female | Mixed (63% Canadian-born, others from Philippines, Jamaica, England, Peru) | 1-7 months | Adolescent mothers recruited through a young parent residential resource center |
| Cavallaro (2023) | UK | (13-19) | Female | Birth - 24 months | Retrospective cohort of all first-time mothers aged 13-19 years at last menstrual period with live births in England between 1 April 2010 and 31 March 2019 and their first-born child(ren). 136 Local Authorities in England had an active FNP site between 2010 and 2019 | |
| Cox (2019) | USA | 17.3 () | Female | African American: 33.3% Hispanic: 60.1% Other: 6.5% |
1 - 15 months | Maternal age 19 years at delivery and willingness to receive maternal and infant care in a teen-tot program.Exclusion: Teens with infants 12 months or older were excluded. |
| Demeusy (2021) | USA | 19.08 (15-23 ) | Female | 66.4% African-American 22.8% Caucasian 4.7% biracial 6.0% other race 17.8% Latina |
birth - 36 months | Mothers under 21 years of age at the birth of their first child. Eligible for Temporary Assistance for Needy Families (TANF). Maximum of two children under the age of 3 years. Resident of Monroe County. No previous Child Protective Services indication with her child. Exclusion: Severe maternal medical illness, severe maternal psychiatric conditions, IQ less than 70, and/or current incarceration. |
| Elliott (2020) | UK | (17-18) | Female | 5-18 months | First-time mother aged 16-19 years with child aged 0-5 years; adolescent is primary caregiver, English-speaking, has no mental health difficulties, child has no chronic illness, not on Child Protection Register. Exclusion: Under age 16, not first-time mother, known mental health difficulties, on Child Protection Register, child over age 5, not primary caregiver, non-English speaking, child has chronic illness | |
| Firk (2021) | Germany | 18.3 (14 -21) | Female | The majority of the mothers in the study were German (100% in the standard care group and 96.6% in the STEEP-b group) | 3-21 months | 21 years old or younger at the beginning of pregnancy, mother and child live together, sufficient verbal and intellectual capacity, child between 3 and 6 months old. Exclusion: Maternal criteria: Current substance abuse, current suicidal ideation, psychotic disorders, separation from the child (> 3 months). Child criteria: Preterm birth (< 36 weeks gestation), serious medical problems, and genetic syndromes. |
| Florsheim (2012) | USA | 16.5 (Mothers: 14-18 years; Fathers: 14-24 years) | Female and Male | The majority of the participants were either Latino or White. Specifically, 50% of the mothers were Latino, and 45% of the fathers were Latino, while the remainder identified as White or other ethnicities | Mothers had to be primiparous, at least 14 years old but not older than 18 years, less than 26 weeks pregnant, and have a coparenting partner (the biological father) who was also willing to participate in the study. The eligibility criterion for biological fathers was that he had to be at least 14 years old but not older than 24 years at the initial assessment. | |
| Hans (2013) | USA | 18.2 () | Female | African American | Pregnant women under the age of 22 and less than 34 weeks gestationExclusion: Plans to move from the area, plans to give up baby for adoption | |
| Hasani (2024) | Iran | (13-20) | Female and Male | Newborns | > 20years, low-risk pregnancy, spending at least 24h after childbirth, stabilization of the mother’s vital signs, access to a cell phone with WhatsApp, living with a sexual partner, and obtaining a score of less than 14.5 based on the GHQ-12, full-term infants without recognized abnormalities at birth. Exclusion: Unwillingness to continue cooperation, hospitalization of the infant in the NICU, and postpartum complications in the mother. | |
| Hubel (2018) | USA | 19.6 (< 21) | 98 % Female | 63% White, 12.9-18.6% American Indian, 10.6-11.4% African American, 6.1-6.2% Hispanic, 3.1-4.5% Other | Adolescent parents (21 years or younger) referred to community-based agencies under contract with the child welfare systemExclusion: Sexual abusers | |
| In-iw (2017) | Thailand | 17.2 () | Female | Teenage mothers and their children who attended the Young Family Clinic (YFC) at Siriraj Hospital and were followed up regularly for at least two yearsExclusion: Mothers and infants who did not complete the two-year program. | ||
| Kachingwe (2021) | Malawi | 17.56 (13-22) | Female | 1-37 months | Adolescent mothers 18 years of age and below | |
| Long (2018) | Canada | () | Female | Parents must have self-referred, aged 19 years of age or younger with child 5 years or younger, parents recognized a concern in their child’s psycho-social-emotional health and well-being or noted behavioral concerns in their child and/or parents had historical or present involvement with the Children’s Aid Society of the Districts of Sudbury and Manitoulin, Parents and/or their child were not experiencing abuse/violence and were not in an active crisis resulting from past experiences of trauma. | ||
| Mackinnon (2014) | Russia | (16-22) | Female | |||
| McHugh (2017) | USA | 17 (14–18 ) | Female | 89.7% Hispanic, 6.9% Bengali, 3.4% African American | birth - 12 months | Age of mother (less than 18 years), willingness to participate in the program |
| McKelvey (2012) | USA | 17.4 () | Female | 40.5% European American (White) 51.1% Black 7.0% Hispanic 1.3% Other |
Adolescent mothers | |
| Nicolson (2013) | Australia | 18.8 (15.7-20.9) | Female | Seventy-two participants (74.2 %) were born in Australia or New Zealand, of whom two were Aboriginal and Torres Strait Islanders (ATSI) (2.1 %) The remaining 25 were born in 16 different countries. Fourteen (14.4 %) were born in African countries and seven (7.2 %) in countries of the Asia Pacific region. | 4 months | Adolescents with viable pregnancies and deemed mature minors, competent to give informed consent and able to complete a questionnaire in English, recruited through the YWP clinic. |
| Paine (2020) | UK | 17.91 (13.82-19.98) | Female | When compared to the original Building Blocks trial, the BABBLE sample was significantly different in terms of maternal ethnicity (with fewer participants of black backgrounds), education (fewer with no qualifications), and more spoke only English in the home (all p < .05, available under request). |
22–33 months | Under the age of 19 and living within a catchment area of an FNP team. |
| Riva Crugnola (2016) | Italy | 18.75 (15-21 ) | Female | In the intervention group 26 mothers were Italian, 2 European and 4 Latin American and in the control group 14 were Italian and 2 Latin Americans. | 3 months | Adolescent mothers aged 14–21, having a first child, and being able to speak and understand the Italian language |
| Riva Crugnola (2021) | Italy | 17.33 (14-21) | Female | Majority Italian. The remaining were European or Latin American who knew the Italian language and were integrated into the Italian cultural context. | 3-9 months | Ability to speak and understand the Italian language; age range between 14 and 21; absence of maternal psychopathology, uneventful delivery, infants born at full term with no medical complications and physically healthy. Exclusion: Prematurity and twin birth. |
| Rispoli (2017) | USA | (15-19) | Female and Male | Of the 3 case study participants: 2 White, 1 Multiracial - the children were describe by the mothers as native american, multiracial and biracial. | 0-36 months | Adolescent parents whose children were enrolled in daycare classrooms in select high schools that provided programming for pregnant and parenting students and who had a history of problematic academic performance. |
| Robling (2016) | UK | 17.9 (< 19 ) | Female | White: 88%, Mixed: 5-6%, Asian: 1-2%, Black: 4-5%, Other: <1% | birth - 24 months | First-time mother, aged 19 or younger, living within the catchment area of a local FNP team, ess than 25 weeks pregnant at the time of recruitment, Able to provide consent, Able to speak English, Women expecting multiple births and those with a previous pregnancy ending in miscarriage, stillbirth.. Exclusion: Women who planned to have their child adopted or intended to move outside the FNP catchment area for more than three months. |
| Rokhanawati (2023) | Indonesia | () | Female | Young mothers from Gunung Kidul District, Yogyakarta | Young mothers aged <20 years, whose first child is aged 12–42 months and who have a minimum education level of Elementary School | |
| Schaffer (2012) | USA | 16.7 (13-19) | Female | Ethnicity included 45% African American and 27% Hispanic teens. Additional ethnic groups represented among teens in the program were American Indian (8%), Asian (7%), White (6%), African (3%), and other (3%) | Adolescent mothers need to be under age 20 and enroll before their child is 2 months of age. They may also enroll in the program if they have more than one child and are under 20 years of age. | |
| Stiles (2010) | USA | 17 (< 18) | Female | Hispanic mother with a black father | 3-6 months | First-time teen mother younger than age 18 years at recruitment who had delivered a healthy infant (≥ 37 weeks gestation, no birth anomalies, and no chronic illness) and who was the primary caregiver for her infant. Exclusion: Non-English-speaking mother, preterm birth (<37 weeks), newborn with birth anomalies, multiple births, infant with chronic illness, or a mother who lived outside of a 75-mile radius from the researcher. |
| Suess (2016) | Germany | 18.08 () | Female | 12-24 months | Participants were drawn from child welfare agencies serving mothers at risk for neglect and abuse. All mothers were eligible for child welfare support. |
|
| Tua (2018) | Puerto Rico | () | Female | The group of adolescent parents included in this study are Latinos/Hispanics, usually from Puerto Rico. | Adolescents who became pregnant with their first child before they were 19 years and 11 months of age, living in Bayamon and vicinities, lack a high school diploma but have achieved the 8th grade. | |
| Valades (2021) | El Salvador | 17 (14-19) | Female | Predominantly rural, low-resource communities in El Salvador | Primiparous women in their third trimester of pregnancy; between 14 and 19 years of age; without medical complications during pregnancy; residing in one of the four participating municipalities. | |
| Williams (2013) | USA | 16.7 (15-18) | Female | 60% African American 40% Hispanic/Latino |
1-16 months | Adolescent mothers, grades 9-12, enrolled in the school-based Early Head Start program, English-speaking. |
i 0 indicates that this data was not reported in the paper.
Table 3.
Programs Methods and Results.
| Citation | Methodology | Method - details | Relevant Outcomes | Results |
|---|---|---|---|---|
| Alarcão (2021) | RCT | RCT - with random blind assigned to intervention or care as usual (CAU) | Mother-infant attachment relationship at child age 12 months | At 12 months, infants in the Primierios Laços intervention group had higher EAS Child Involvement scores than those in the CAU group. A greater proportion of infants in the intervention group were classified as "Emotionally Available" compared to the CAU group. |
| Barlow (2013) | RCT | RCT - Participants randomly assigned to intervention or care as usual. | Parenting knowledge, self-efficacy, home safety, maternal psychosocial and behavioural risk, child emotional and behavioural functioning at 12 months. | Family Spirit Program mothers demonstrated increased parenting knowledge, self-efficacy, better home safety attitudes, and reduced externalizing behaviors, while their children had fewer externalizing problems. The impact was stronger for mothers with a history of substance use, with their children showing fewer externalizing and dysregulation problems and a lower likelihood of being clinically "at risk" for externalizing and internalizing issues. However, the intervention did not significantly affect HOME scale scores or maternal substance use. |
| Barr (2011) | Mixed | Mixed methods - quasi-experimental pilot with control and intervention group and one case study. | Joint attention, emotional engagement, child involvement, turn-taking and following the lead | Individual growth curve analyses showed significant gains in five of six measures of emotional responsiveness over time for Bably Elmo Program participants. These results indicate improvements in positive high quality interactions and communication during sessions between infants and their incarcerated parents. |
| Barr (2014) | Quantitative | Quants - Observational study and pre-post design | Father-baby activities and parenting skills | The Baby Elmo Program fathers showed significant improvements in parenting behaviors (e.g., praise, maintains and extends) and child engagement over time, with increases in parent support and infant engagement linked to more intervention sessions, while correlations highlighted strong associations between key parenting skills and outcomes. |
| Berry (2022) | Quantitative | Quants - quasi-experimental, longitudinal design with baseline-midline-endline. | Depression and parenting behaviours at 10-month follow-up. | Positive parenting and resilience improved for all participants suggesting that changes over time were not caused by the programme. Intervention participants with higher depression showed less change towards positive parenting indicating the importance of addressing adolescent parent depression. |
| Bohr (2014) | Quantitative | Quants - pre-post design pilot, no control group | Maternal sensitivity, parenting confidence, parenting stress, postnatal depression. | Maternal sensitivity significantly improved for Right from the Start participants but there was no significant difference for depression or parenting stress. |
| Cavallaro (2023) | Quantitative | Quants - secondary data analysis with linked cohort receiving intervention or CAU. | Child maltreatment and child health outcomes for up to 7 years after birth. | No evidence of FNP and indicators of child maltreatment; weak evidence for likelihood children achieving a good level of development by age 5. |
| Cox (2019) | RCT | RCT - random assignment | Maternal self-esteem, parenting attitudes, preparedness for mothering, acceptance of infant, expected relationship with infant at 36 months. | Significantly improved maternal self esteem, preparedness, acceptance and expected relationship in the Office of Adolescent Pregnancy Programs intervention group. |
| Demeusy (2021) | Quantitative | Quants - longitudinal, quasi-experimental with random assignment to intervention or care-as-usual. | Positive parenting, maternal mental health, prevention of child maltreatment and harsh parenting, child symptomatology and self-regulation. | BHC participants showed significant reductions in depressive symptoms at mid-intervention, which was associated with improvements in parenting self-efficacy and stress as well as decreased child internalizing and externalizing symptoms at postintervention. Intervention mothers exhibited less harsh and inconsistent parenting, and marginally less psychological aggression. Intervention children also exhibited less externalizing behavior and self-regulatory difficulties across parent and teacher report. |
| Elliott (2020) | Mixed | Mixed - Semi-structured interviews and quantitative observations with no control group. | Attuned interactions - being attentive, encouraging initiatives, receiving initiatives, developing attuned interactions, guiding and deepening discussion; maternal sensitivity. | There was no significant effect for the VIG participants. |
| Fatori (2020) | RCT | RCT - with random blind assignment to intervention or CAU. | Maternal parenting (singing a song, telling a story, going for a stroll, playing, talking, eating together, positive physical contact)) and parental well-being at 18 months. | Significant effect of Primeiros Laços on parental well-being and maternal parenting behaviour - singing and telling a story, but not on other behaviours. |
| Fatori (2021) | RCT | RCT - with random blind assignment to intervention or CAU, longitudinal design with assessment at 3, 6, 12, & 24 months. | Child development, home environment (emotional and verbal responsivity, avoidance of restriction and punishment, organisation of the physical environment, provision of play materials, parental involvement and variety in daily stimulation. | Significant effect of Primeiros Laços on child expressive language development, maternal emotional / verbal responsivity, variety in daily stimulation but not on other areas of development or home environment. |
| Firk (2021) | RCT | RCT with blind assessors assessing at baseline, midline and endline. | Maternal sensitivity and child responsiveness during free play and an age-appropriate stress situation. | No effect of STEEP-b program on maternal sensitivity, structuring, non-intrusiveness or non-hostility and child responsiveness or involvement. |
| Florsheim (2012) | Quantitative | Quants - quasi-experimental with random assignment to intervention or CAU. | Co-parenting skills and parental functioning second trimester, 3 months & 18 months. Paternal engagement at T3. | Fathers completing the Young Parenthood Program demonstrated more positive parenting. Positive outcomes in paternal functioning were mediated through mother's interpersonal skill development. This in turn predicted positive parenting and coparenting including higher rates of paternal nurturance and lower child abuse potential scores. |
| Hans (2013) | RCT | RCT - | Parent-infant interactions at 4, 12, & 24 months and parenting attitudes and stress. | Mothers in the Chicago Doula Project had more child-centred parenting values, more positive engagement with infants and were more likely to respond to infant distress at 4 months. Infants were less upset during interactions. Beyond the intervention which ceased at 3 months, effects were not sustained. |
| Hasani (2024) | Quantitative | Quants - quasi-experimental with pre-post-6wks post design, no control group. | Parent-child attachment - absence of hostility and pleasure in interaction. | Parenting attachment improved for quality of attachment, absence of hostility and pleasure in interaction for SATIR participants. |
| Hubel (2018) | Quantitative | Quants- quasi-experimental with intervention and CAU. | Child welfare recidivisim, depression and child abuse potential. | The SafeCare intervention did not result in significantly improved outcomes in terms of preventing recidivism or reduction in risk factors associated with child abuse and neglect as compared to child welfare services as usual. Further, no significant differences in program engagement and satisfaction between SafeCare and services as usual were detected. |
| In-iw (2017) | Descriptive | Quants- descriptive, observational. | Child maltreatment and parenting skills. | The YFC showed good outcomes for teenage mothers and their children. Educational sessions, particularly types of contraceptives, parenting skills, and risk prevention had an impact on young family’s outcomes. |
| Kachingwe (2021) | Mixed | Mixed - quasi-experimental with intervention and control groups with pre/post assessment design, participant interviews. | Parenting skills, nutritional practice, parenting stress, mother-child interaction, child physical development and cognitive functions. | The Young Womens' Christian Association of Malawi intervention group showed statistically significant increase in knowledge on parenting skills, nutritional practice, motor skills and cognitive functions in children, as well as expressive language and socio-emotional capacities in children, while the change in confidence and psychosocial well-being was not statistically significant. |
| Long (2018) | Mixed | Mixed - case study and pre-post pilot with no control group. | Parenting stress and parenting interactions | There were observable differences in the interactions of mothers particularly if they attended 10-15 sessions of Theraplay. Increased parenting stress co-occurred with increased negative parenting behaviours. |
| Mackinnon (2014) | Qualitative | Quals - photovoice and interviews. | Maternal sensitivity & social connection. | Participants in the Pskov Positive Parenting Program shifted behaviours to include more sensitive, responsive parenting behavior; competence and confidence in the mothering role increased; social connections between the participants strengthened and helped reduce their isolation; the Program provided information about maternal rights and facilitated access to social and medical services; the Program provided a forum and resources for participants experiencing domestic violence; and finally, the Program had a non-hierarchical, participatory structure. |
| McHugh (2017) | Quantitative | Quants - observational study for intervention completers verses non-completers. | Child abuse reports and health outcomes for infants including emergency room visits, immunisation status and weight. and their parents | Those who completed a full year of the Bellevue Hospital Adolescent Program had some significantly improved measures compared to those who did not, with fewer child abuse reports and more well-baby visits, more immunisations and earlier referral for developmental delays. There was additional health benefits for the adolescent mothers noted as well. |
| McKelvey (2012) | Quantitative | Quants - quasi-experimental, longitudinal (measures at baseline then every 6 months over 24 months), intervention and CAU. | Parenting and child rearing attitudes. | The Thrive Program participants had less inappropriate expectations of children, less strong beliefs in the use of corporal punishment and less reversing of parent-child family roles. However, there was no effect for empathy towards children's needs or oppressing children's power and independence. |
| Nicolson (2013) | Quantitative | Quants - pilot quasi-experimental design with intervention and CAU, blind coded assessors | Mother-infant interaction at age 4 months. | AMPLE intervention effect was evident for emotional availability and separation-reunion as well as maternal non-intrusiveness and maternal non-hostility. |
| Paine (2020) | RCT | Quants - observational sub study of RCT comparing intervention to CAU. | Internal state language (referencing cognitions, desires, emotions, intentions, preferences, physiology and perception) reflecting quality of maternal communication and emotional attunement. | No significant differences were found between Family Nurse Partnership (FNP) and CAU groups in the frequency of maternal internal state language during mother–child interactions. Factors associated with fewer internal state references included higher deprivation scores and mothers not being in education, employment, or training, while positive predictors included being friends with the child’s father and higher maternal mean length of utterance (MLU). Multivariate analysis confirmed that mothers' relationship with the father and MLU were significantly associated with increased use of internal state language. |
| Riva Crugnola (2016) | Mixed | Mixed - quasi-experimental pilot with intervention and control; case study | Maternal sensitivity, parenting style and emotional regulation in both adolescents and mothers at 3, 6, and 9 months. | PRERAYMI participants showed significantly improved maternal sensitivity and decreased controlling styles, with positive effects on infant cooperation, reduced passivity, and increased time spent in coordinated play and affective matches, especially within the first six months. Dyads in the intervention group demonstrated greater capacity for repairing mismatches and maintaining positive interactions compared to the control group, which showed declines in sensitivity, increases in controlling styles, and more mismatched states over time. |
| Riva Crugnola (2021) | Quantitative | Quants - quasi-experimental with intervention and control and pre/post design. | Maternal mind-mindedness and styles of interaction evaluated at infant aged 3 months and 9 months. | The PRERAYMI intervention significantly improved outcomes with increases in attuned mind-related comments, overall verbalizations, maternal sensitivity, and infant cooperative style, while reducing non-attuned and controlling behavour. No changes were observed in the control group. Neither maternal attachment nor childhood experiences of maltreatment significantly moderated the intervention's effects on mind-mindeness or mother-infant interaction styles. |
| Rispoli (2017) | Mixed | Mixed - case study and quantitative pre-post observational data. | Parental positive affect, responsiveness, verbalisations to help child self-regulate and social initiations towards child. | The PIWI-T intervention is acceptable to teachers, can be implemented with fidelity, and has the potential to increase positive caregiving practices for adolescent parents with the largest effects for responsiveness and quality of verbalisations. |
| Robling (2016) | RCT | RCT - Pragmative, non-blinded, random assignment, parallel-group to intervention or care as usual. | Emergency attendance and hospital admission for child in first 24 months | No evidence of benefit from Family Nurse Partnership intervention on smoking and other addictions or on child emergency admissions. |
| : Rokhanawati (2023) | Quantitative | Quants - quasi-experimental with intervention and control and pre/post design. | Parenting self-efficacy and behaviour, growth and development of children. | Compared with the control group, the PPE intervention group reported significantly better parenting self-efficacy, parenting behaviour, children’s growth, and children’s cognitive and language development with very small effects on motor development. |
| Schaffer (2012) | Descriptive | Quants - descriptive, intervention compared to all teens in the metro area. | Maternal-infant bonding and attachment and infant growth and development | MVNA participants were supported with parenting skills and child development, with 95% of children up-to-date on immunizations, 92% with normal ASQ:SE scores, and significant improvements in maintaining a safe home environment and responsiveness to babies, alongside high participant satisfaction (92% recommending the program). |
| Stiles (2010) | Mixed | Mixed methods - Descriptive case study & pre/post design. | Maternal sensitivity, depression, anxiety, self-concept, parenting stress at post-test. | Participant gained confidence in parenting abilities and increased maternal sensitivity to her infant. There was no change in her depression and her anxiety increased. Self-concept, parenting stress and social support all improved. |
| Suess (2016) | Quantitative | Quants - quasi-experimental design with allocation to intervention or CAU and data collection at 12 & 24 months. | Mother- infant attachment style, parenting attitudes, maternal depression. | Significant attachment results (increased security, decreased disorganization) were evident at 12 months and at 24 months in the STEEPb intervention group, even though they had higher risk factors. At the end of intervention, STEEPb group mothers showed significant less risky child rearing attitudes, particularly in empathy and valuing children's autonomy. Depression was not affected. |
| Tua (2018) | Quantitative | Quants - quasi-experimental with pre-post design and comparison to control group. | Responsible parenting skills (no child negligence or abuse records), co-parenting practices. | There was a significant change in nurturing family environments between pre and post for the Family Incubator Model intervention participants. |
| Valades (2021) | RCT | RCT - pilot study with random assignment to intervention or CAU, blind assessment, pre-post design. | Parental sensitivity, infant emotional regulation. | Thula Sana had a positive impact on maternal sensitivity and infants showed more regulated behaviour, more attempts to restore communication and more social and goal-directed behaviour. |
| Williams (2013) | Quantitative | Quants - pre-post design pilot, no control group | Dysfunctional parenting style - laxness, overactivity, verbosity. | There was no statistically significant difference between pre and post for parenting style for Incredible Years participants. |
Table 4.
Quality Ratings.
| Citation | Methodology | Program Name | Score/5 | S12 | S23 | S34 | S45 |
|---|---|---|---|---|---|---|---|
| Alarcão (2021) | RCT | Primeiros Laços | 4 | X | X | X | X |
| Barlow (2013) | RCT | Family Spirit Program | 3 | X | X | X | X |
| Barr (2011) | Mixed | The Baby Elmo Program | 4 | X | X | X | X |
| Barr (2014) | Quantitative | The Baby Elmo Program | 3 | X | X | X | X |
| Berry (2022) | Quantitative | N/A | 3 | X | X | X | |
| Bohr (2014) | Quantitative | Right From the Start | 1 | X | X | X | X |
| Cavallaro (2023) | Quantitative | Family Nurse Partnership | 4 | X | X | X | X |
| Cox (2019) | RCT | Office of Adolescent Pregnancy Programs | 3 | X | X | X | |
| Demeusy (2021) | Quantitative | Building Healthy Children | 4 | X | X | X | X |
| Elliott (2020) | Mixed | Video Interaction Guidance (VIG) | 3 | X | X | X | |
| Fatori (2020) | RCT | Primeiros Laços | 4 | X | X | X | X |
| Fatori (2021) | RCT | Primeiros Laços | 5 | X | X | X | X |
| Firk (2021) | RCT | STEEP-b | 2 | X | X | X | |
| Florsheim (2012) | Quantitative | Young Parenthood Program | 3 | X | X | X | X |
| Hans (2013) | RCT | Chicago Doula Project | 4 | X | X | X | |
| Hasani (2024) | Quantitative | SATIR Approach | 2 | X | X | ||
| P19: Hubel (2018) | Quantitative | SafeCare | 3 | X | X | X | |
| In-iw (2017) | Descriptive | Young Family Clinic | 1 | X | X | ||
| Kachingwe (2021) | Mixed | The Young Women's Christian Association of Malawi | 2 | X | X | X | |
| Long (2018) | Mixed | Theraplay | 2 | X | |||
| Mackinnon (2014) | Qualitative | Pskov Positive Parenting Program | 3 | Can't tell | X | ||
| McHugh (2017) | Quantitative | Bellevue Hospital Adolescent Parenting Program | 2 | X | X | ||
| McKelvey (2012) | Quantitative | Thrive Program (derived from the Healthy Families America model) | 1 | X | X | X | X |
| Nicolson (2013) | Quantitative | AMPLE Intervention | 4 | X | X | X | |
| Paine (2020) | RCT | Family Nurse Partnership | 2 | X | X | X | X |
| Rispoli (2017) | Mixed | Parents Interacting with Infants - Teen version (PIWI-T) | 3 | X | X | X | X |
| Riva Crugnola (2016) | Mixed | PRERAYMI | 4 | X | X | X | X |
| Riva Crugnola (2021) | Quantitative | PRERAYMI | 4 | X | X | X | X |
| Robling (2016) | RCT | Family Nurse Partnership | 5 | X | X | X | X |
| Rokhanawati (2023) | Quantitative | Parenting Peer Education Model | 4 | X | X | X | |
| Schaffer (2012) | Descriptive | MNVA Pregnant and Parenting Teen Program | 5 | X | X | ||
| Stiles (2010) | Mixed | Promoting First Relationships | 1 | X | X | ||
| Suess (2016) | Quantitative | STEEP-b (Steps Toward Effective and Enjoyable Parenting) | 3 | X | X | X | X |
| Tua (2018) | Quantitative | Family Incubator Model | 2 | X | |||
| Valades (2021) | RCT | Thula Sana | 5 | X | X | X | X |
| Williams (2013) | Quantitative | Incredible Years | 2 | X | X |
- 2
- Are there clear research questions?
- 3
- Do the collected data address the research questions?
- 4
- Is the description of the method sufficient for replication?
- 5
- Does the intervention have sufficient standardisation to enable replication (is it manualised)?
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



