
Submitted:
23 July 2025
Posted:
24 July 2025
You are already at the latest version
Abstract
Background: Copy number variations (CNVs), also referred to as large genomic rearrangements (LGRs), represent a crucial component of BRCA1/2 (BRCA) testing. Next-generation sequencing (NGS) has become an established approach for detecting LGRs by combining sequencing data with dedicated bioinformatics pipelines. However, CNV detection in formalin-fixed paraffin-embedded (FFPE) samples remains technically challenging, and it cannot always be guaranteed that such in-formation will be reliably obtained. Therefore, optimization is needed, and implementing a robust analysis strategy for routine clinical practice could provide significant advantages.
Methods: This study evaluated 40 FFPE ovarian cancer (OC) samples from patients undergoing BRCA testing. The performance of the amplicon-based NGS Diatech Myriapod® NGS BRCA1/2 panel (Diatech Pharmacogenetics, Jesi, Italy) was assessed for its ability to detect BRCA CNVs, and results were compared to two hybrid capture-based reference assays.
Results: Among the 40 analyzed samples (17 CNV-positive and 23 CNV-negative for BRCA genes), the Diatech pipeline showed high concordance with the reference methods. In a clinical di-agnostic setting, the evaluated method achieved an overall accuracy of about 96%, with a sensitivity of 94% and specificity of 96%. Despite one inconclusive result due to low sequencing quality and one sample with a somatic CNV in BRCA1 that was not detected, the Diatech Myriapod® NGS BRCA1/2 panel kit demonstrated strong potential for routine clinical application in CNV detection from FFPE tissue.
Conclusions: These findings support the clinical utility of NGS-based CNV analysis in FFPE sam-ples when combined with appropriate bioinformatics tools. Integrating visual inspection of CNV plots with automated CNV calling improves the reliability of CNV detection and enhances the in-terpretation of results from tumor tissue. Accurate CNV detection directly from tumor tissue may reduce the need for reflex germline testing and improve turnaround times. Nevertheless, blood-based testing remains essential to determine whether detected BRCA CNVs are of germline or so-matic origin, particularly in cases with a strong clinical suspicion of a germline CNV.
Keywords:
BRCA genes
; NGS
; large genomic rearrangements
; ovarian cancer
; copy number variations
; FPG500
; Diatech Myriapod® NGS BRCA1/2 panel kit
; SOPHiA DDM™ homologous recombination solution
1. Introduction
Hereditary breast and/or ovarian cancer syndrome has traditionally been the primary criterion for genetic counseling, followed by germline BRCA1/2 (BRCA) testing [1]. However, over the past decade, numerous clinical studies have demonstrated that ovarian cancer (OC) patients harboring germline or somatic pathogenic BRCA variants (PVs) show sensitivity to poly (ADP-ribose) polymerase inhibitors (PARPi) and platinum-based chemotherapy [2,3]. In addition, functional defects in homologous recombination repair genes, collectively referred to as homologous recombination deficiency (HRD), have been clinically validated as predictive biomarkers for PARPi treatment in OC [4]. As a result, BRCA and/or HRD testing on formalin-fixed paraffin-embedded (FFPE) tumor samples, which allow simultaneous detection of both somatic and germline PVs, has become increasingly important in the molecular management of OC patients [5,6,7].
Copy number variations (CNVs), also referred to as large genomic rearrangements (LGRs), such as deletions or duplications larger than 1,000 base pairs, have been identified in BRCA genes. Their prevalence varies widely among populations, ranging from less than 1% to more than 24% [8]. Consequently, LGRs account for a substantial proportion of BRCA PVs and are now an integral component of BRCA and HRD testing [6].
Next-generation sequencing (NGS) is a now well-established method for comprehensive BRCA screening from blood, enabling the simultaneous detection of single nucleotide variants (SNVs), insertions/deletions (indels), and CNVs [9,10,11]. However, CNV detection in tumor tissue presents specific challenges, including tumor heterogeneity, low tumor cellularity, the absence of a matched normal baseline, poor DNA quality, and the presence of PCR contaminants or artifacts. These factors can lead to uneven sequencing coverage across genomic regions, impairing the accurate identification of CNVs. As a result, NGS-based CNV detection may generate false positives or, more critically, false negatives, particularly when using workflows that lack validated and dedicated bioinformatics pipelines for CNV calling [10,11].
Among various NGS protocols, hybrid capture-based approaches have demonstrated greater reliability for CNV detection compared to amplicon-based PCR protocols. Nonetheless, several BRCA CNV assays are currently available, and not all are fully validated for clinical use or supported by robust bioinformatics pipelines [12].
The aim of this study was to evaluate the ability of different NGS bioinformatics pipelines to accurately identify and call BRCA CNVs from FFPE tumor samples. To this end, 40 OC samples were selected, including 17 samples harboring clinically significant LGRs. CNV calls from two hybrid capture-based NGS protocols were compared with the amplicon PCR-based Diatech Myriapod® NGS BRCA1/2 panel kit.
Finally, an analysis strategy was proposed to improve the interpretation of NGS data for reliable identification of CNVs in FFPE samples, in a clinical setting (Figure 1).
2. Materials and Methods
2.1. Patient Cohort and Study Design
This retrospective cohort study was conducted at the Genomics Core Facility, G-STeP, Fondazione Policlinico Universitario Agostino Gemelli IRCCS. Formalin-fixed paraffin-embedded (FFPE) tumor blocks from patients with advanced or relapsed platinum-sensitive OC were collected as part of routine clinical care for BRCA status assessment through the FPG500 program [13] and HRD testing performed in our institution. The same FFPE samples were evaluated for CNV calling using the Diatech Myriapod® NGS BRCA1/2 panel kit (Diatech Pharmacogenetics, Jesi, Ancona, Italy).
A total of 40 patients were included in the study: 17 with BRCA CNV-positive results and 23 with BRCA CNV-negative results. All CNVs corresponded to clinically significant LRGs (Table 1).
All participants provided informed consent to participate in the study (Study ID: FPG500; Ethics Committee Approval No. 3837), which was conducted in accordance with the Declaration of Helsinki. Patient characteristics are summarized in Table 1.
2.2. Patient Selection
Patient selection for the study was performed using the TruSight Oncology 500 High Throughput (TSO500HT) (Illumina Inc., San Diego, CA) and the SOPHiA DDM™ Homologous Recombination Solution (SOPHiA DDM™ HRD) (SOPHIA Genetics). Both tests were performed on 19 samples, while 21 samples were analyzed with only one of the two assays (Table 1).
Multiplex Ligation-dependent Probe Amplification (MLPA) analysis on blood samples was carried out to confirm whether the CNVs were of germline origin, using the SALSA P002 BRCA1 and SALSA P045 BRCA2 MLPA kits (MRC Holland), as previously described [12].
The reference sequences used for CNV reporting were NG_005905.2/NM_007294.3 and NG_012772.3/NM_000059.3 for BRCA1 and BRCA2 respectively (Table 1).
2.3. DNA Extraction
For DNA extraction, FFPE tissue samples containing >20% tumor cells and <10% necrosis, as determined by the local pathologist, were selected. DNA was extracted using the Qiagen AllPrep DNA/RNA FFPE Kit on the EZ2 Connect workstation (Qiagen), following the manufacturer's protocol. DNA quantity and quality were assessed using the Qubit 3.0 Fluorometer (Thermo Fisher Scientific, Waltham, MA, USA).
2.4. BRCA Testing with Myriapod® NGS BRCA1/2 Panel Kit and Primary Sequencing Strategy
The Myriapod® NGS BRCA1/2 panel kit is an in vitro diagnostic assay that enables the detection of SNVs, indels and splice variants in the BRCA genes. CNV analysis and calling were conducted using a proprietary algorithm part of toghe Myriapod® NGS data analysis software.
With the aim to evaluate the performance of CNV detection algorithm of Myriapod® NGS BRCA1/2 panel kit considering “stressed” testing conditions, a “primary CNV calling strategy” was defined. In this strategy, four NGS runs, each including 10 FFPE samples, were performed on the MiSeq System, using MiSeq Micro Flow Cell (Illumina Inc., San Diego, CA). Specifically, two runs included 5 BRCA CNV-positive and 5 BRCA CNV-negative cases, while the other two runs consisted of 4 BRCA CNV-positive and 6 BRCA CNV-negative samples, respectively.
Data analysis was performed using Myriapod® NGS Data analysis software (Diatech Pharmacogenetics, Jesi, Ancona, Italy).
2.5. Re-Evaluation of CNV Calling Using Diatech Software by Simulating a Diagnostic Setting
To further evaluate the CNV calling performance of the Myriapod® NGS BRCA 1-2 kit in association with the Myriapod® NGS data analysis software , all 40 samples were re-analyzed to simulate a routine clinical setting. Specifically, the analysis was designed to reflect a scenario in which CNVs occur with an estimated prevalence of less than 10% in the general population, corresponding to the likelihood of detecting at most one positive case per sequencing run of 10 samples.
2.6. Read Coverage and Comparative Analyses
Sequencing performance was evaluated across the 4 NGS runs, with the aim of optimizing CNV calling. Key quality metrics assessed included mean coverage, percentage of uniformity and on-target reads. Results were analyzed separately for each sequencing run and summarized as mean ± standard deviation (SD) across all samples within each run.
In parallel with the assessment of sequencing quality, statistical analyses were conducted to evaluate CNV calling performance using the Myriapod® NGS BRCA1/2 panel kit in association with Myriapod® NGS data analysis software. Overall accuracy, sensitivity, and specificity of the Myriapod® NGS BRCA 1-2 solution were calculated and compared to those of the TSO500HT and SOPHiA DDM™ HRD Solution kits.
2.7. Data Analysis
Sequencing data were processed and interpreted using Myriapod® NGS Data Analysis Software, a CE-marked in vitro diagnostic application for targeted NGS assays within the Diatech NGS Applications portfolio. The software automatically generates an initial variant report, incorporating both SNVs, indels and CNVs analysis. For CNV detection, it plots each gene on an independent chart, assigning a copy-number score for each exon or amplicon.
3. Results
A total of 40 OC patients, selected from tests previously performed in-house as part of routine clinical care, were enrolled in the study. As shown in Table 1, 17 samples were BRCA-CNV positive and 23 were BRCA-CNV negative. The performance of CNV detection using the Myriapod® NGS BRCA1/2 panel in combination with the Myriapod® NGS data analysis software was assessed at three distinct levels:
- (a)
- Graphical visualization and interpretation of CNV plots;
- (b)
- CNV calling by the Myriapod® NGS data analysis software;
- (c)
- Final interpretation and reporting of CNV status, as a decision-making result integrating the two previous analysis levels.
3.1. Concordance Analysis Between TSO500HT/SOPHiA DDM HRD and Myriapod® NGS BRCA 1-2 Pipeline in Primary CNV Calling Strategy (5/4 BRCA CNV-Positive vs 5/6 BRCA CNV-Negative Samples in the Same NGS Run)
3.1.1. BRCA-CNV-Negative Samples
Based on the graphical visualization and interpretation of CNV status, out of the 23 CNV-negative samples, 16 could be considered negative for both genes. Four samples were CNV-negative for BRCA2 but showed a potential CNV in BRCA1. One sample was CNV-negative for BRCA1 with an inconclusive CNV result in BRCA2, while another was CNV-negative for BRCA2 with an inconclusive CNV result in BRCA1. Finally, one sample was negative for BRCA1 and showed an "other CNV" in BRCA2.
According to the CNV calling performed by the Diatech software, 7 samples were classified as CNV Not Positive for both genes. Nine samples were CNV Not Positive for BRCA2 but showed a Potential CNV in BRCA1. Three samples were identified as Potential CNV for both genes, and 4 samples showed a Potential CNV in BRCA2 and were CNV Not Positive for BRCA1.
The final interpretation and reporting of CNV status, based on both graphical visualization and software based CNV calling, led to the classification of 18 samples as negative, 3 samples as showing a Potential CNV in BRCA1 and Negative in BRCA2, 1 sample as Inconclusive in BRCA2 and Negative in BRCA1, and 1 sample with a potential CNV in BRCA2 and CNV negative in BRCA1 (Table 2)
Considering the final interpretation and reporting of CNV results, out of the 23 negative samples, 18 would be considered completely negative, and 5 would be referred for confirmatory testing.
3.1.2. BRCA-CNV-Positive Samples
Based on graphical visualization and interpretation of CNV status, among the 17 CNV-positive samples, 10 were confirmed as Positive in both genes. In 2 samples, a CNV was confirmed in BRCA2, while a Potential CNV was suspected in BRCA1. In 1 sample, the CNV was confirmed in BRCA1 and considered Inconclusive in BRCA2. In 2 samples, the CNV was not confirmed in BRCA1 and was Inconclusive in BRCA2. In another sample, a CNV was confirmed in BRCA1, and an additional CNV was suspected in BRCA2. Finally, one sample was considered a complete CNV calling failure in both genes. According to CNV calling by the Diatech software, one sample was classified as failed.
In 9 samples, the expected CNV was correctly identified. Of these, 5 also showed a Potential CNV in the other gene, where a negative result was expected. In the remaining 4, only the expected CNV was detected. In 7 samples, the expected CNV was not detected, but a Potential CNV was identified in the other gene.
The final interpretation and reporting of CNV status, integrating graphical visualization with software-based calling, resulted in 13 samples being classified as definitively CNV-positive. Two samples were negative for the expected CNV but showed inconclusive findings in other genes. One sample was interpreted as Inconclusive for CNVs in both target genes, and one sample was classified as failed (Table 2).
Considering the final interpretation and reporting of CNV results, out of the 17 positive samples, 13 would be considered Positive, and 3 samples as Negative and 1 Inconclusive.
Overall, under these analytical conditions, the Myriapod® NGS BRCA1/2 pipeline shows a sensitivity, specificity, and accuracy of about 80% compared to the reference assays (Table 4).
3.2. CNV Calling in a Simulated Diagnostic Scenario (1 BRCA CNV-Positive vs 9 BRCA CNV-Negative Samples in the Same NGS Run)
3.2.1. BRCA-CNV-Negative Samples
Based on the graphical visualization and interpretation of CNV status, out of the 23 CNV-negative samples, 22 could be considered negative for both genes. One sample was Negative for BRCA2 but showed a Potential CNV in BRCA1.
According to the CNV calling performed by the Diatech software, 13 samples were classified as CNV Not Positive for both genes. Four samples were CNV Not Positive for BRCA1 but showed a Potential CNV in BRCA2. Four samples showed a Potential CNV in BRCA2 and were CNV Not Positive for BRCA1. Two samples were identified as CNV-Positive for both genes.
The final interpretation and reporting of CNV status, integrating both graphical visualization and software-based CNV calling, led to the classification of 22 samples as Negative, and 1 sample as showing a Potential CNV in BRCA1 with CNV Negative in BRCA2. Based on the final interpretation and reporting, among the 23 samples initially classified as CNV-negative, 22 were considered definitively negative, while 1 sample was recommended for confirmatory testing.
3.2.2. BRCA-CNV Positive Samples
Based on the graphical visualization and interpretation of CNV status, among the 17 CNV-positive samples, 14 were confirmed as Positive for both genes. One sample showed a confirmed CNV in BRCA1 and an Inconclusive result in BRCA2. One sample did not show a CNV in BRCA1 as expected and was also Inconclusive in BRCA2.
According to the CNV calling performed by the Diatech software, one sample was classified as failed. In 12 samples, the expected CNV was correctly identified. Of these, four also showed a Potential CNV in the other gene, where a negative result was expected. In the remaining eight samples, only the expected CNV was detected. Four samples did not show the expected CNV in BRCA1 but instead showed a CNV in BRCA2.
The final interpretation and reporting of CNV status, integrating graphical visualization with software-based calling, resulted in 15 samples being classified as definitively CNV-positive. One sample was interpreted as Negative in BRCA1 (compared to the expected result) and Inconclusive in BRCA2. One sample was classified as failed (Table 3).
Overall, under these analytical conditions, the Diatech pipeline showed a sensitivity, specificity, and accuracy of about 95% when compared to the reference assays (Table 4).
3.3. Sequencing Metrics and Performance
The distribution of sequencing quality metrics across individual samples in different runs is shown in Figure 2. Mean coverage was uniformly high, reflecting adequate sequencing depth consistent with expected performance in somatic sequencing. Coverage uniformity confirmed efficient and balanced target representation. The percentage of on-target reads showed minimal variation between samples reflecting the specificity and overall performance of the protocol.
Table 5 compared the summary statistics (mean ± standard deviation) of mean coverage, and on-target read percentage across the different sequencing runs, as well as the overall averages. Mean coverage was maintained at elevated levels across all four runs, with a total average of 6680 ± 1346×. The mean uniformity across all samples was 94.9% ± 0.88, suggesting efficient and balanced coverage of the targeted regions. The percentage of on-target reads was remarkably high across all runs, with minimal variability with a total mean of 99.8% ± 0.05. Taken together, these results demonstrate a high level of technical reliability across runs, with all quality metrics falling within expected and acceptable thresholds.
4. Discussion
This study evaluated the analytical performance of different NGS strategies for the detection of BRCA CNVs in FFPE samples from OC patients. Specifically, we focused on the concordance of CNV calls between two hybrid capture-based protocols and the amplicon-based Diatech Myriapod® NGS BRCA1/2 panel. Particular attention was given to the clarity and reliability of result interpretation, as well as the practical feasibility of integrating these methods into routine clinical diagnostics. A key emphasis was placed on the crucial role of bioinformatics pipelines in enabling accurate and robust CNV detection, especially when dealing with the technical challenges posed by FFPE-derived DNA, which is often degraded and affected by tumor heterogeneity [15]. Amplicon-based sequencing protocols are widely used in clinical diagnostics due to their high efficiency in detecting SNVs and indels. However, several studies have highlighted the limitations of these methods in accurately detecting CNVs, particularly in FFPE samples [12].
An interesting aspect was the strategy used to evaluate the Diatech Myriapod® NGS BRCA1/2 solution. Specifically, the bioinformatics pipeline was first intentionally stressed by assessing CNV calling under diagnostic conditions with up to 5 BRCA CNVs in a run of 10 samples. Subsequently, a more clinically realistic setting was simulated, in which only one CNV might be present in an NGS run of 10 OC samples. In both analytical conditions, the pipeline demonstrated high performance. Notably, in the second analysis mode, CNV calling using the Diatech Myriapod® NGS BRCA1/2 panel achieved a maximum accuracy of approximately 96% compared to hybrid capture-based reference methods in successfully identifying CNVs. Excluding one sample that failed sequencing, all germline CNV-positive cases were correctly identified. Among the somatic CNVs, only one case was missed. We recognize that this limitation may arise particularly in the context of somatic CNVs, where different NGS strategies can exhibit variable detection performance. However, missing a somatic CNV is generally considered less critical than failing to identify a germline CNV, which can have significant implications for patient management and familial risk assessment [16].
From a diagnostic perspective, our findings suggest that graphical visualization and software-based interpretation should be considered complementary tools. Therefore, a multi-step approach combining algorithmic CNV calling, graphical visualization, and expert review is confirmed as the most reliable strategy, particularly for CNV detection in amplicon-based protocols using FFPE samples (Figure 1). It is, however, essential to note that the manufacturer's instructions require that samples automatically classified by the software as CNV-potential positive must always be confirmed by an orthogonal method.
The reliability of CNV detection is also intrinsically linked to the quality of sequencing data. Accurate variant calling requires that key quality metrics, such as mean coverage, coverage uniformity, and on-target read percentage, meet established thresholds. When these metrics fall below recommended levels, the risk of inconclusive or incorrect calls increases, primarily due to insufficient read depth or uneven read distribution. In our study, sequencing metrics remained consistently high across runs, with mean coverage exceeding 6,600× and on-target rates approaching 100%, supporting the technical robustness of the workflow and likely contributing to the successful CNV detection.
Among the strengths of this study are the use of real-world clinical FFPE samples, comparison across different NGS platforms, and simulation of practical diagnostic scenarios. However, certain limitations must be acknowledged. First, the sample size was relatively small and may not fully capture the heterogeneity of BRCA CNVs observed in routine clinical practice. Second, orthogonal validation methods (e.g., MLPA, qPCR) were not employed for all discordant or borderline cases, which may have introduced uncertainty in result interpretation.
Looking ahead, integrating automated quality control checkpoints and confidence scoring for CNV calls could reduce the burden of manual review while enhancing overall reliability. Furthermore, continued development and validation of dedicated CNV detection algorithms specifically optimized for amplicon-based sequencing will be essential for broader clinical implementation.
5. Conclusions
Our study highlights the importance of having validated NGS workflows and bioinformatics pipelines for the accurate detection of BRCA CNVs in FFPE tumor samples. The amplicon-based Myriapod® NGS BRCA1/2 panel in combination with Myriapod® NGS data analysis software proved effective in identifying CNVs, demonstrating strong concordance with hybrid capture-based approaches when combined with optimized bioinformatics analysis and expert interpretation and reporting.
These elements are essential for the reliable molecular identification of BRCA CNVs, which carry critical implications for the management of OC patients, including therapeutic decisions involving PARP inhibitors and cascade testing in hereditary cancer syndromes. For these reasons, it is possible to hypothesize a decision-making workflow, as described in Figure 1, where suspected CNV detections can guide either a therapeutic approach or germline screening as for other PVs in BRCA genes. Therefore, the accurate and reliable detection of these alterations remains a fundamental requirement in the genomic evaluation of OC patients.
Acknowledgements
We gratefully acknowledge the Diatech team for their technical support, in contributing to the results presented. We also thank the Genomics Core Facility Group at the Gemelli Science and Technology Park (G-STeP) for their valuable contribution. This work is dedicated to the memory of Professor Giovanni Scambia, whose untimely passing represents a profound loss to the scientific community. His exceptional dedication, visionary leadership, and significant contributions to the field continue to inspire and guide both this project and future research efforts.
Conflicts of Interest
The authors declare that they have no competing interests.
Abbreviations
CNVs: Copy number variations; LGRs: large genomic rearrangements; BRCA: BRCA1/2;NGS: Next generation sequencing; FFPE: Formalin-fixed paraffin-embedded; OC: Ovarian cancer; PVs: Pathogenic variants; PARP-1: Poly-(ADP-ribose) polymerase; HRD: Homologous recombination repair; SNVs: single nucleotide variants (SNVs); INDELS: Insertions/deletions; MLPA: Multiplex ligation-dependent probe amplification; SD: Standard deviation
References
- Marmolejo, D.H.; Wong, M.Y.Z. Overview of Hereditary Breast and Ovarian Cancer (HBOC) Guidelines across Europe. Eur. J. Med. Genet. 2021, 64, 104350.
- Lee, J.M.; Ledermann, J.A.; Kohn, E.C. PARP Inhibitors for BRCA1/2 Mutation-Associated and BRCA-Like Malignancies. Ann. Oncol. 2014, 25, 32–40.
- Dewani, D.; Jaiswal, A.; Karwade, P.C. Poly(Adenosine Diphosphate Ribose) Polymerase (PARP) Inhibitors in the Treatment of Advanced Ovarian Cancer: A Narrative Review. Cureus 2024, 16, e68463.
- Guffanti, F.; Mengoli, I.; Damia, G. Current HRD Assays in Ovarian Cancer: Differences, Pitfalls, Limitations, and Novel Approaches. Front. Oncol. 2024, 14, 1405361.
- Ratnaparkhi, R.; Javellana, M.; Jewell, A.; Spoozak, L. Evaluation of Homologous Recombination Deficiency in Ovarian Cancer. Curr. Treat. Options Oncol. 2024, 25, 237–260.
- Arcieri, M.; Tius, V.; Andreetta, C.; Restaino, S.; Biasioli, A.; Poletto, E.; Damante, G.; Ercoli, A.; Driul, L.; Fagotti, A.; Lorusso, D.; Scambia, G.; Vizzielli, G. How BRCA and Homologous Recombination Deficiency Change Therapeutic Strategies in Ovarian Cancer: A Review of Literature. Front. Oncol. 2024, 14, 1335196.
- Mafficini, A.; Simbolo, M.; Parisi, A.; Rusev, B.; Luchini, C.; Cataldo, I.; Piazzola, E.; Sperandio, N.; Turri, G.; Franchi, M.; Tortora, G.; Bovo, C.; Lawlor, R.T.; Scarpa, A. BRCA Somatic and Germline Mutation Detection in Paraffin-Embedded Ovarian Cancers by Next-Generation Sequencing. Oncotarget 2016, 7, 1076–1083.
- Ewald, I.P.; Ribeiro, P.L.; Palmero, E.I.; Cossio, S.L.; Giugliani, R.; Ashton-Prolla, P. Genomic Rearrangements in BRCA1 and BRCA2: A Literature Review. Genet. Mol. Biol. 2009, 32, 437–446.
- Concolino, P.; Mello, E.; Minucci, A.; Santonocito, C.; Scambia, G.; Giardina, B.; Capoluongo, E. Advanced Tools for BRCA1/2 Mutational Screening: Comparison between Two Methods for Large Genomic Rearrangements (LGRs) Detection. Clin. Chem. Lab. Med. 2014, 52, 1119–1127.
- Enyedi, J.; Pintér, L.; Sükösd, F.; Gyuris, Z.; Hajdu, A.; Határvölgyi, E.; Priskin, K.; Haracska, L. Simultaneous Detection of BRCA Mutations and Large Genomic Rearrangements in Germline DNA and FFPE Tumor Samples. Oncotarget 2016, 20, 61845–61859.
- Schmidt, A.Y.; Hansen, T.V.O.; Ahlborn, L.B.; Jønson, L.; Yde, C.W.; Nielsen, F.C. Next-Generation Sequencing-Based Detection of Germline Copy Number Variations in BRCA1/BRCA2: Validation of a One-Step Diagnostic Workflow. J. Mol. Diagn. 2017, 19, 809–816.
- Minucci, A.; Mazzuccato, G.; Marchetti, C.; Pietragalla, A.; Scambia, G.; Fagotti, A.; Urbani, A. Detecting Large Germline Rearrangements of BRCA1 by Next-Generation Tumor Sequencing. Mol. Biol. (Mosk.) 2020, 54, 688–698.
- Nero C.; Duranti S.; Giacomini F.; Minucci A.; Giacò L.; Piermattei A.; Genuardi M.;Pasciuto T.; Urbani A.; Daniele G.; Lorusso D.; Pignataro R.; Tortora G.; Normanno N.; Scambia G. Integrating a Comprehensive Cancer Genome Profiling into Clinical Practice: A Blueprint in an Italian Referral Center. J. Pers. Med. 2022,12,1746.
- Minucci, A.; Scambia, G.; Santonocito, C.; Concolino, P.; Canu, G.; Mignone, F.; Saggese, I.; Guarino, D.; Costella, A.; Molinario, R.; De Bonis, M.; Ferrandina, G.; Petrillo, M.; Scaglione, G.L.; Capoluongo, E. Clinical Impact on Ovarian Cancer Patients of Massive Parallel Sequencing for BRCA Mutation Detection: The Experience at Gemelli Hospital and a Literature Review. Expert Rev. Mol. Diagn. 2015, 15, 1383–1403.
- Szczerba, E.; Kamińska, K.; Mierzwa, T.; Misiek, M.; Kowalewski, J.; Lewandowska, M.A. BRCA1/2 Mutation Detection in the Tumor Tissue from Selected Polish Patients with Breast Cancer Using Next Generation Sequencing. Genes 2021, 12, 519.
- Barili, V.; Ambrosini, E.; Bortesi, B.; Minari, R.; De Sensi, E.; Cannizzaro, I.R.; Taiani, A.; Michiara, M.; Sikokis, A.; Boggiani, D.; et al. Genetic Basis of Breast and Ovarian Cancer: Approaches and Lessons Learnt from Three Decades of Inherited Predisposition Testing. Genes 2024, 15, 219.
Figure 1.
Strategy for interpreting CNV calls from NGS data in FFPE samples, optimized for real-world clinical implementation.
Figure 1.
Strategy for interpreting CNV calls from NGS data in FFPE samples, optimized for real-world clinical implementation.
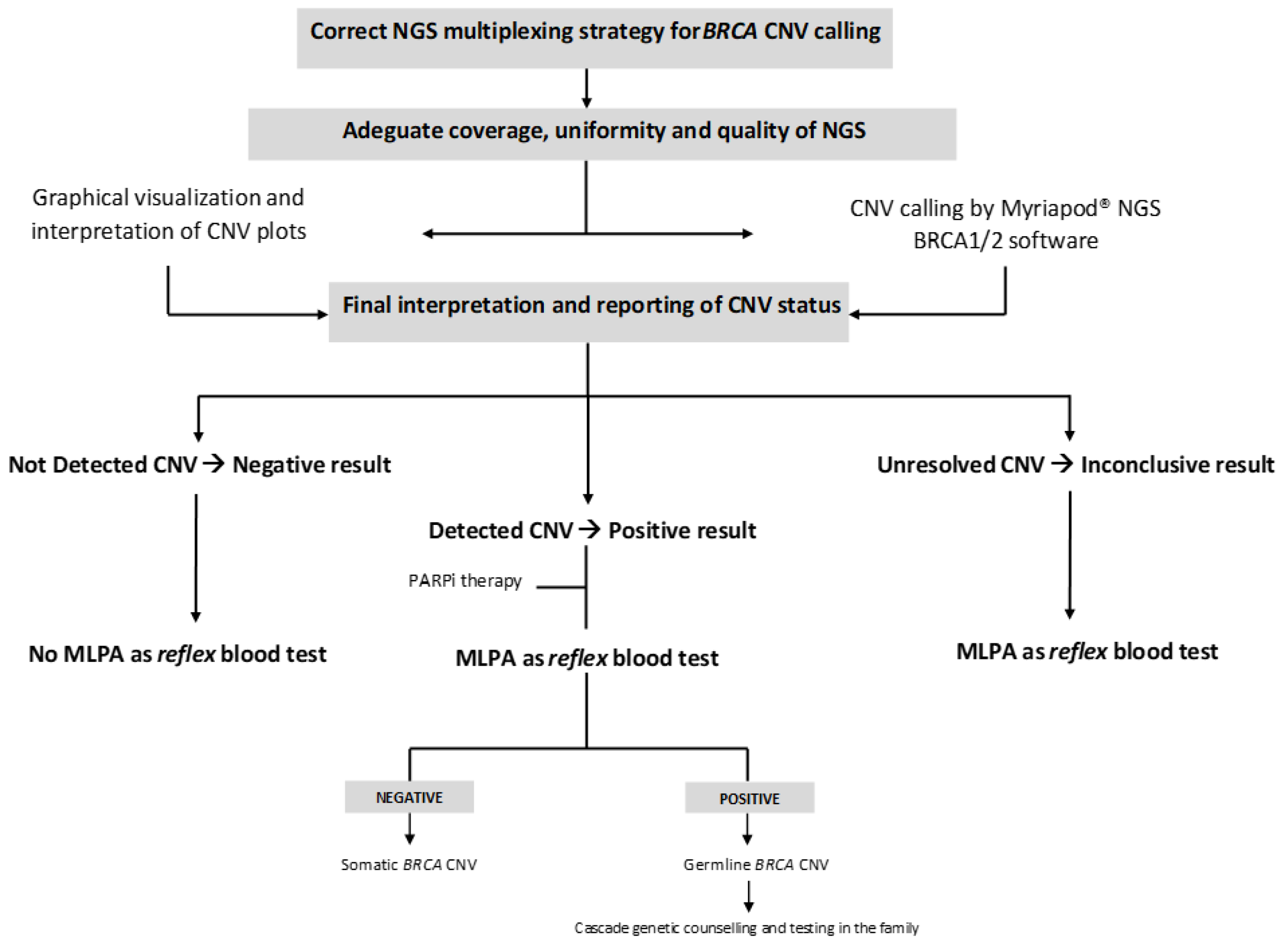
Figure 2.
Comparison of sequencing metrics between NGS runs: Mean Coverage (X); On target reads (%); Uniformity (%).
Figure 2.
Comparison of sequencing metrics between NGS runs: Mean Coverage (X); On target reads (%); Uniformity (%).


Table 1.
Clinical and molecular characteristics of patients enrolled in the study.
| ID | Disease | Timing | Age of the sample | Tumor content (%) | CNV Status | Reference assay | Gene | Exons | Type of CNV | Status of CNV* |
| 1 | HGSC | PRIMARY | 2024 | 90 | Positive | TSO500HT | BRCA2 | 2-3 | Intragenic deletion | Somatic |
| 2 | HGSC | PRIMARY | 2024 | 90 | Positive | TSO500HT SOPHiA DDM HRD HRD |
BRCA1 | 19 | Intragenic deletion | Somatic |
| 3 | HGSC | PRIMARY | 2024 | 60 | Positive | TSO500HT SOPHiA DDM HRD |
BRCA1 | 8-11 | Intragenic deletion | Germline |
| 4 | HGSC | PRIMARY | 2024 | 70 | Positive | TSO500HT SOPHiA DDM HRD |
BRCA1 | 20 | Intragenic deletion | Germline |
| 5 | HGSC | RELAPSE | 2023 | 90 | Positive | TSO500HT SOPHiA DDM HRD |
BRCA1 | 2 | Intragenic deletion | Germline |
| 6 | HGSC | RELAPSE | 2024 | 90 | Positive | SOPHiA DDM HRD | BRCA1 | 16-17 | Intragenic deletion | Germline |
| 7 | HGSC | RELAPSE | 2024 | 70 | Positive | TSO500HT SOPHiA DDM HRD |
BRCA1 | 4-7 | Intragenic deletion | Germline |
| 8 | HGSC | PRIMARY | 2023 | 90 | Positive | TSO500HT SOPHiA DDM HRD |
BRCA2 | 19-21 | Intragenic deletion | Somatic |
| 9 | ENOC | PRIMARY | 2024 | 90 | Positive | TSO500HT | BRCA1 | 11 | Intragenic deletion | Somatic |
| 10 | HGSC | PRIMARY | 2024 | 95 | Positive | TSO500HT SOPHiA DDM HRD |
BRCA1 | 2-3 | Intragenic deletion | Somatic |
| 11 | HGSC | PRIMARY | 2024 | 60 | Positive | TSO500HT SOPHiA DDM HRD |
BRCA1 | 19 | Intragenic deletion | Germline |
| 12 | HGSC | RELAPSE | 2024 | 80 | Positive | SOPHiA DDM HRD | BRCA1 | 2 | Intragenic deletion | Germline |
| 13 | HGSC | RELAPSE | 2024 | 80 | Positive | SOPHiA DDM HRD | BRCA1 | 2- 19 | Intragenic deletion | Somatic |
| 14 | HGSC | PRIMARY | 2024 | 80 | Positive | TSO500HT | BRCA1 | 15 | Intragenic deletion | Somatic |
| 15 | HGSC | PRIMARY | 2024 | 55 | Positive | TSO500HT SOPHiA DDM HRD |
BRCA1 | 1-24 | Whole gene deletion | Germline |
| 16 | HGSC | PRIMARY | 2025 | 30 | Positive | TSO500HT SOPHiA DDM HRD |
BRCA2 | 11-27 | Intragenic deletion | Somatic |
| 17 | HGSC | PRIMARY | 2024 | 80 | Positive | TSO500HT | BRCA1 | 3-23 | Intragenic deletion | Somatic |
| 18 | OCS | RELAPSE | 2024 | 60 | Positive | TSO500HT SOPHiA DDM HRD |
- | - | - | - |
| 19 | HGSC | PRIMARY | 2024 | 80 | Negative | TSO500HT SOPHiA DDM HRD |
- | - | - | - |
| 20 | HGSC | PRIMARY | 2025 | 20 | Negative | TSO500HT | - | - | ||
| 21 | HGSC | PRIMARY | 2024 | 80 | Negative | TSO500HT SOPHiA DDM HRD |
- | - | - | - |
| 22 | HGSC | PRIMARY | 2024 | 80 | Negative | TSO500HT | - | - | - | - |
| 23 | CCOC | PRIMARY | 2024 | 80 | Negative | TSO500HT | - | - | - | - |
| 24 | ENOC | PRIMARY | 2024 | 90 | Negative | TSO500HT | - | - | - | - |
| 25 | HGSC | PRIMARY | 2024 | 25 | Negative | TSO500HT | - | - | - | - |
| 26 | HGSC | PRIMARY | 2024 | 80 | Negative | TSO500HT SOPHiA DDM HRD |
- | - | - | - |
| 27 | HSGC | RELAPSE | 2024 | 95 | Negative | SOPHiA DDM HRD | - | - | - | - |
| 28 | ENOC | RELAPSE | 2024 | 30 | Negative | SOPHiA DDM HRD | - | - | - | - |
| 29 | HSGC | RELAPSE | 2024 | 30 | Negative | SOPHiA DDM HRD | - | - | - | - |
| 30 | HSGC | RELAPSE | 2024 | 35 | Negative | SOPHiA DDM HRD | - | - | - | - |
| 31 | HGSC | PRIMARY | 2023 | 70 | Negative | TSO500HT SOPHiA DDM HRD |
- | - | - | - |
| 32 | CCOC | PRIMARY | 2023 | 80 | Negative | TSO500HT | - | - | - | - |
| 33 | HGSC | PRIMARY | 2024 | 40 | Negative | TSO500HT SOPHiA DDM HRD |
- | - | - | - |
| 34 | HGSC | PRIMARY | 2024 | 36 | Negative | SOPHiA DDM HRD | - | - | - | - |
| 35 | HGSC | PRIMARY | 2023 | 80 | Negative | SOPHiA DDM HRD | - | - | - | - |
| 36 | HGSC | PRIMARY | 2025 | 70 | Negative | TSO500HT SOPHiA DDM HRD |
- | - | - | - |
| 37 | CCOC | PRIMARY | 2025 | 20 | Negative | TSO500HT | - | - | - | - |
| 38 | HGSC | PRIMARY | 2025 | 30 | Negative | TSO500HT SOPHiA DDM HRD |
- | - | - | - |
| 39 | CCOC | PRIMARY | 2025 | 70 | Negative | TSO500HT | - | - | - | - |
| 40 | HGSC | PRIMARY | 2025 | 25 | Negative | TSO500HT | - | - | - | - |
* CNV status was determined using MLPA as a reflex test on peripheral blood samples; Abbreviations: HGSC: High grade serous carcinoma; ENOC: endometrioid ovarian cancer, OCS: Ovarian carcinosarcoma; CCOC: Clear Cell Ovarian Carcinoma.
Table 2.
Concordance analysis between TSO500HT/SOPHiA DDM HRD and Myriapod® NGS BRCA1/2 software results in primary CNV calling strategy (5/4 BRCA-CNV positive vs 5/6 BRCA CNV-negative samples).
Table 2.
Concordance analysis between TSO500HT/SOPHiA DDM HRD and Myriapod® NGS BRCA1/2 software results in primary CNV calling strategy (5/4 BRCA-CNV positive vs 5/6 BRCA CNV-negative samples).
|
ID samples |
Graphical visualization and intepretation of CNV plots |
CNV calling by Diatech software |
Final interpretation and reporting CNV |
||||||||||
| BRCA1 | BRCA2 | BRCA1 | BRCA2 | BRCA1 | BRCA1 | ||||||||
| BRCA CNV-negative samples | |||||||||||||
| 18 | cCNV | oCNV | Potential CNV | Potential CNV | Negative | oCNV | |||||||
| 19 | oCNV | cCNV | Potential CNV | CNV Not Positive | Negative | Negative | |||||||
| 20 | cCNV | cCNV | CNV Not Positive | Potential CNV | Negative | Negative | |||||||
| 21 | cCNV | cCNV | Potential CNV | Potential CNV | Negative | Negative | |||||||
| 22 | cCNV | cCNV | Potential CNV | CNV Not Positive | Negative | Negative | |||||||
| 23 | cCNV | cCNV | Potential CNV | CNV Not Positive | Negative | Negative | |||||||
| 24 | cCNV | cCNV | Potential CNV | CNV Not Positive | Negative | Negative | |||||||
| 25 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | |||||||
| 26 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | |||||||
| 27 | oCNV | cCNV | Potential CNV | CNV Not Positive | oCNV | Negative | |||||||
| 28 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | |||||||
| 29 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | |||||||
| 30 | oCNV | cCNV | Potential CNV | CNV Not Positive | oCNV | Negative | |||||||
| 31 | cCNV | cCNV | Potential CNV | CNV Not Positive | Negative | Negative | |||||||
| 32 | cCNV | cCNV | Potential CNV | CNV Not Positive | Negative | Negative | |||||||
| 33 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | |||||||
| 34 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | |||||||
| 35 | cCNV | cCNV | CNV Not Positive | Potential CNV | Negative | Negative | |||||||
| 36 | cCNV | cCNV | CNV Not Positive | Potential CNV | Negative | Negative | |||||||
| 37 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | |||||||
| 38 | iCNV | cCNV | Potential CNV | CNV Not Positive | Negative | Negative | |||||||
| 39 | cCNV | iCNV | CNV Not Positive | Potential CNV | Negative | iCNV | |||||||
| 40 | oCNV | cCNV | Potential CNV | Potential CNV | oCNV | Negative | |||||||
| BRCA CNV-positive samples | |||||||||||||
| 1 | oCNV | cCNV | Potential CNV | Potential CNV | Positive | Positive | |||||||
| 2 | cCNV | cCNV | Potential CNV | Potential CNV | Positive | Negative | |||||||
| 3 | cCNV | cCNV | Potential CNV | Potential CNV | Positive | Negative | |||||||
| 4 | cCNV | cCNV | Potential CNV | CNV Not Positive | Positive | Negative | |||||||
| 5 | cCNV | cCNV | Potential CNV | CNV Not Positive | Positive | Negative | |||||||
| 6 | cCNV | cCNV | CNV Not Positive | Potential CNV | Positive | Negative | |||||||
| 7 | cCNV | oCNV | CNV Not Positive | Potential CNV | Negative | iCNV | |||||||
| 8 | oCNV | cCNV | Potential CNV | Potential CNV | oCNV | Positive | |||||||
| 9 | fCNV | fCNV | CNV Failed | CNV Failed | fCNV | fCNV | |||||||
| 10 | cCNV | cCNV | CNV Not Positive | Potential CNV | Positive | Negative | |||||||
| 11 | cCNV | cCNV | Potential CNV | CNV Not Positive | Positive | Negative | |||||||
| 12 | cCNV | iCNV | CNV Not Positive | Potential CNV | Positive | iCNV | |||||||
| 13 | cCNV | cCNV | CNV Not Positive | Potential CNV | Positive | Negative | |||||||
| 14 | cCNV | cCNV | Potential CNV | Potential CNV | Positive | Positive | |||||||
| 15 | ntCNV | iCNV | CNV Not Positive | Potential CNV | Negative | iCNV | |||||||
| 16 | cCNV | cCNV | CNV Not Positive | Potential CNV | Negative | Positive | |||||||
| 17 | ntCNV | iCNV | CNV Not Positive | Potential CNV | iCNV | iCNV | |||||||
Abbreviations: oCNV: other CNV; cCNV: confirmed CNV; fCNV: failed CNV; iCNV: inconclusive CNV; ntCNV: not detected CNV.
Table 4.
Concordance analysis of CNV calling between the Myriapod® NGS BRCA1/2 Panel and TSO500HT and the SOPHiA DDM™ HRD assays.
Table 4.
Concordance analysis of CNV calling between the Myriapod® NGS BRCA1/2 Panel and TSO500HT and the SOPHiA DDM™ HRD assays.
| A) Primary CNV Calling Strategy and concordance analysis (5/4 BRCA CNV-positive vs 5/6 BRCA CNV-negative samples). | ||
| Diatech Myriapod® NGS BRCA1/2panel kit | TSO500HT/SOPHiA DDM™ HRD | |
| CNV Positive | CNV Negative | |
| CNV Positive | 13 | 5 |
| CNV Negative | 3 | 18 |
| Inconclusive | 1 | |
| Analytical Performance | Value (%) | |
| Sensitivity | 81.25 | |
| Specificity | 78.26 | |
| Positive predictive value | 72.22 | |
| Negative predictive value | 85.71 | |
| Accuracy | 79.49 | |
| B) CNV Calling in a simulated BRCA diagnostic setting (1 BRCA CNV-positive vs 9 BRCA CNV-negative samples) | ||
| Diatech Myriapod® NGS BRCA1/2panel kit | TSO500HT/SOPHiA DDM™ HRD | |
| CNV Positive | CNV Negative | |
| CNV Positive | 15 | 1 |
| CNV Negative | 1 | 22 |
| Inconclusive | 1 | |
| Analytical Performance | Value (%) | |
| Sensitivity | 93.75 | |
| Specificity | 95.65 | |
| Positive predictive value | 94.87 | |
| Negative predictive value | 93.75 | |
| Accuracy | 95.65 | |
Table 3.
Concordance analysis between TSO500HT/SOPHiA HRD DDM and Diatech software results in CNV calling in a simulated BRCA diagnostic setting (1 BRCA CNV-positive vs 9 BRCA CNV-negative samples.
Table 3.
Concordance analysis between TSO500HT/SOPHiA HRD DDM and Diatech software results in CNV calling in a simulated BRCA diagnostic setting (1 BRCA CNV-positive vs 9 BRCA CNV-negative samples.
|
ID samples |
Graphical visualization and intepretation of CNV plots |
CNV calling by Diatech software |
Final interpretation and reporting CNV |
|||||||
| BRCA1 | BRCA2 | BRCA1 | BRCA2 | BRCA1 | BRCA1 | |||||
| BRCA CNV-negative samples | ||||||||||
| 18 | cCNV | cCNV | CNV Not Positive | Potential CNV | Negative | Negative | ||||
| 19 | cCNV | cCNV | CNV Not Positive | Potential CNV | Negative | Negative | ||||
| 20 | cCNV | cCNV | Potential CNV | CNV Not Positive | Negative | Negative | ||||
| 21 | cCNV | cCNV | CNV Not Positive | Potential CNV | Negative | Negative | ||||
| 22 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | ||||
| 23 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | ||||
| 24 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | ||||
| 25 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | ||||
| 26 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | ||||
| 27 | cCNV | cCNV | Potential CNV | CNV Not Positive | Negative | Negative | ||||
| 28 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | ||||
| 29 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | ||||
| 30 | cCNV | cCNV | Potential CNV | CNV Not Positive | Negative | Negative | ||||
| 31 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | ||||
| 32 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | ||||
| 33 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | ||||
| 34 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | ||||
| 35 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | ||||
| 36 | cCNV | cCNV | CNV Not Positive | Potential CNV | Negative | Negative | ||||
| 37 | cCNV | cCNV | CNV Not Positive | CNV Not Positive | Negative | Negative | ||||
| 38 | cCNV | cCNV | Potential CNV | CNV Not Positive | Negative | Negative | ||||
| 39 | oCNV | cCNV | Potential CNV | Potential CNV | oCNV | Negative | ||||
| 40 | cCNV | cCNV | Potential CNV | Potential CNV | Negative | Negative | ||||
| BRCA CNV-positive samples | ||||||||||
| 1 | cCNV | cCNV | CNV Not Positive | Potential CNV | Negative | Positive | ||||
| 2 | cCNV | cCNV | Potential CNV | CNV Not Positive | Positive | Negative | ||||
| 3 | cCNV | cCNV | Potential CNV | Potential CNV | Positive | Negative | ||||
| 4 | cCNV | cCNV | Potential CNV | CNV Not Positive | Positive | Negative | ||||
| 5 | cCNV | cCNV | Potential CNV | CNV Not Positive | Positive | Negative | ||||
| 6 | cCNV | cCNV | Potential CNV | CNV Not Positive | Positive | Negative | ||||
| 7 | cCNV | iCNV | CNV Not Positive | Potential CNV | Positive | iCNV | ||||
| 8 | cCNV | cCNV | Potential CNV | Potential CNV | Negative | Positive | ||||
| 9 | fCNV | fCNV | CNV failed | CNV failed | fCNV | fCNV | ||||
| 10 | cCNV | cCNV | Potential CNV | CNV Not Positive | Positive | Negative | ||||
| 11 | cCNV | cCNV | Potential CNV | CNV Not Positive | Positive | Negative | ||||
| 12 | cCNV | cCNV | Potential CNV | Potential CNV | Positive | Negative | ||||
| 13 | cCNV | cCNV | CNV Not Positive | Potential CNV | Positive | Negative | ||||
| 14 | cCNV | cCNV | Potential CNV | Potential CNV | Positive | Negative | ||||
| 15 | cCNV | cCNV | CNV Not Positive | Potential CNV | Positive | Negative | ||||
| 16 | cCNV | cCNV | CNV Not Positive | Potential CNV | Negative | Positive | ||||
| 17 | ntCNV | iCNV | CNV Not Positive | Potential CNV | Negative | iCNV | ||||
Abbreviations: oCNV: other CNV; cCNV: confirmed CNV; fCNV: failed CNV; iCNV: inconclusive CNV; ntCNV: not detected CNV .
Table 5.
Summary statistics (mean ± standard deviation) across the different NGS runs: Mean coverage (X); On -target read (%).
Table 5.
Summary statistics (mean ± standard deviation) across the different NGS runs: Mean coverage (X); On -target read (%).
| Mean ± Standard Deviation | |||
| ID Run | Mean Coverage | Uniformity (%) | On target reads (%) |
| 1 | 5231±876 | 96.1±1.9 | 99.9±0.03 |
| 2 | 6514±1083 | 94.6±2.3 | 99.9±0.03 |
| 3 | 8490±2167 | 94±6.12 | 99.8±0.2 |
| 4 | 6488±2732 | 94.9±2.6 | 99.8±0.07 |
| Total | 6680±1346 | 94.9±0.88 | 99.8±0.05 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



