
Submitted:
08 December 2025
Posted:
11 December 2025
You are already at the latest version
Abstract
Despite progress in controlling microbial infections, the global burden of pathogenic bacteria remains high. Moreover, the spread of antibiotic-resistant bacteria has increased and is likely to continue. Consequently, recent research has focused on antibiotic alternatives to slow the proliferation of resistance and improve patient outcomes. One promising approach is phage therapy, which uses lytic viruses of bacteria to treat bacterial infections. However, an underexplored potential benefit is its capacity to enhance health outcomes across the socioeconomic spectrum and improve healthcare equity. Drawing on the history of phage therapy, recent clinical successes, and advancements in research, we argue that phage therapy is well-suited to advance health and healthcare equity. This is because it offers a comparatively greater potential to increase access and reduce disadvantages faced by lower socioeconomic groups relative to conventional antibiotics. Based on these points, we propose research objectives that aim to achieve these scientific and ethical goals.
Keywords:
antimicrobial resistance
; bacteriophage
; bioethics
; health equity
; health services accessibility
; phage therapy
Introduction
Despite the significant biomedical advances of the 21st century, the global incidence and impact of microbial infections remain high. Every year, microbial infections cause millions of human deaths globally [1]. Simultaneously, pathogenic microbes have a significant economic impact on various industries, including agriculture, farming, and food processing [2,3,4,5]. Amongst microbes, pathogenic bacteria present unique challenges, and their burden is predicted to increase in the next few decades for various reasons. For one, the human population is growing, and a significant portion of this growth will occur in low and middle-income countries (LMICs) with limited medical and public health infrastructure relative to high-income countries (HICs), leaving sizable portions of these populations facing elevated risk [6,7]. Secondly, climate change and other human-induced environmental changes, like encroachment on wildlife habitats, are expected to contribute to an increasing prevalence of bacterial infections [8,9,10]. Lastly, the prevalence of antibiotic resistance is spreading among various pathogenic bacterial species, while simultaneously, the speed of traditional antibiotic discovery has slowed [11,12]. An estimated 1.1 million deaths were attributable to antibiotic resistant bacteria in 2021, and recent studies estimate that by 2050, this could increase to as many as 1.9 million, while costing over $100 trillion in global economic output [13,14]. In turn, calls for antibiotic stewardship across medicine and agriculture have begun [15], even though millions die yearly in LMICs from lack of access to antibiotics [16]. These factors contribute to a growing concern about the potential burden of bacterial diseases in the future and how we should prepare for and deal with them. One treatment option that has received increasing attention in the past decade is phage therapy.
Bacteriophages are naturally occurring viruses that specifically infect bacteria and are the most abundant biological entities on Earth [17]. Phage therapy is the therapeutic use of bacteriophages to combat bacterial infections in patients, with the goal of improving their medical outcomes [18]. The use of bacteriophages in medicine dates to the early 1900s, when researchers, soon after discovering bacteriophages, hypothesized that they could be used to combat infections in humans. Despite the early interest and promise, research into the therapeutic use of phages slowed following the discovery of penicillin and broader advances in antibiotic production [19]. Nonetheless, the use of phages continued primarily in the former Soviet Union and other Eastern Bloc nations, which remained effectively isolated from the antibiotic advances of the Western world [20]. Indeed, routine medical treatment with phages continues today in countries like Russia, Georgia, and Poland [21,22]. However, while the emerging antimicrobial resistance (AMR) crisis has reinvigorated scientific interest in phage therapy, it is only one of the motivating factors for continued investment. Another possible motivation for advancing research into phage therapy, in addition to or instead of traditional antibiotics, may be the bioethical advantages associated with the method. As we will argue, these advantages make phage therapy particularly well-suited to address healthcare inequities related to the burden of pathogenic bacteria.
Equity is the absence of unfair differences amongst groups of people that are avoidable or remediable, whether those groups are defined socially, economically, demographically, or geographically [23]. To use a historical example, before women’s suffrage, voting rights were inequitable, in that men but not women were eligible to vote. That political difference was both unfair and avoidable. Healthcare equity is the absence of unfair differences in access to healthcare among different groups of people that are avoidable or remediable. This is impeded by preventable disparities linked to social determinants, including income inequality, healthcare accessibility, differences in the physical built environment, workplace conditions, group-based discrimination, and access to education [24,25,26]. We contend that phage therapy can play a unique and vital role in promoting healthcare equity by directly addressing issues related to antimicrobial control that are primarily driven by income and healthcare access inequalities. Importantly, it is also equipped to address how these may be exacerbated by rising antibiotic resistance. This is because, compared to traditional antibiotics, phage therapy products are more likely to have lenient storage requirements, lower manufacturing costs, a lower barrier to entry for producers due to publicly available phage manufacturing protocols, and the relative ease of isolating phage candidates from the environment [27,28,29]. These contribute to more efficient patient accessibility and distribution, as well as a reduced reliance on the existing commercial pharmaceutical industry for LMICs. These characteristics can work cohesively to alleviate issues related to bacterial infections disproportionately faced by lower socio-economic populations.
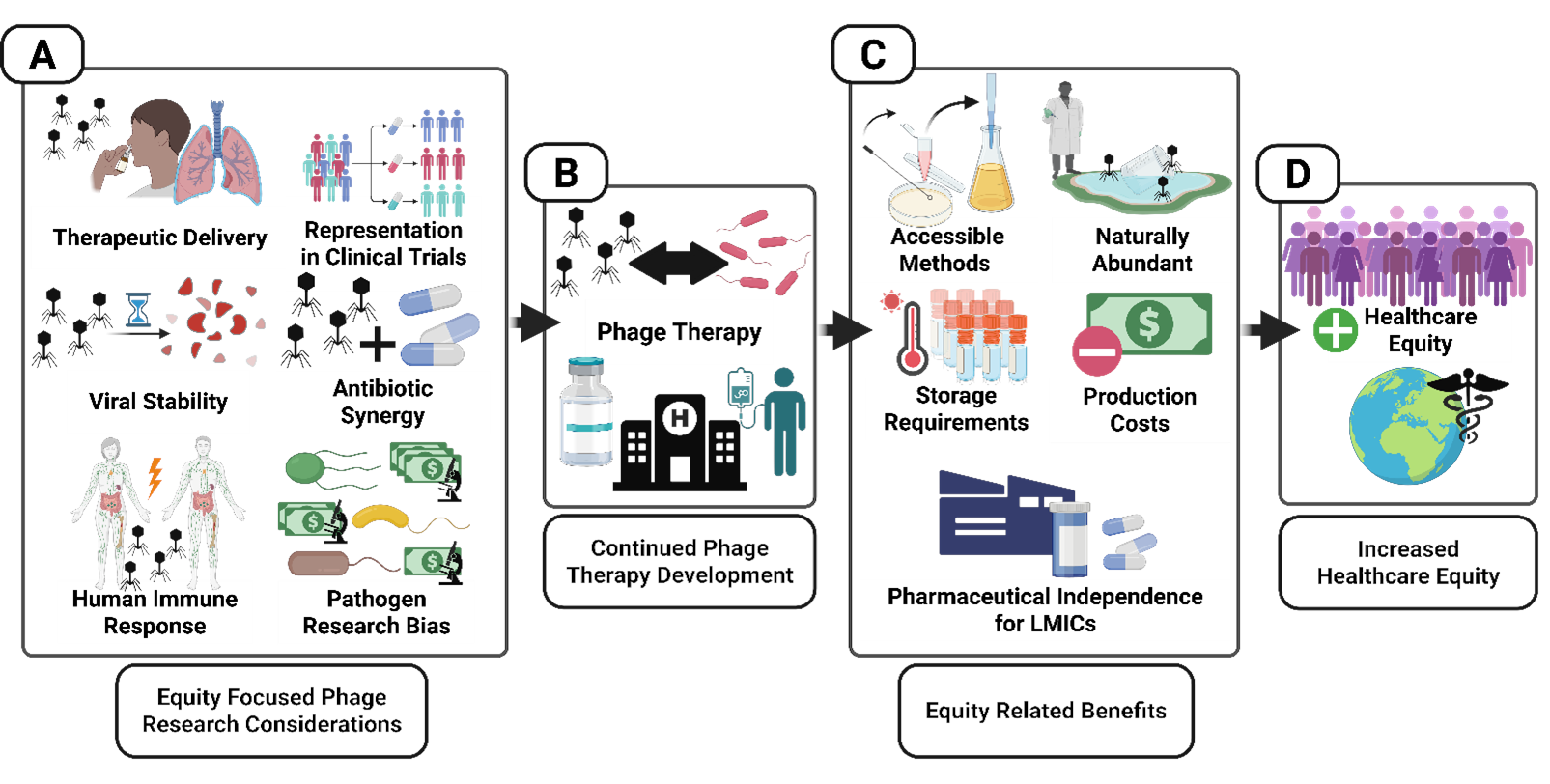
Here, we employ an interdisciplinary approach to examine how investment in bacteriophage therapy can enhance healthcare equity in countries worldwide, ultimately enabling individuals to reach a fuller potential for health and well-being (global health equity; Figure 1). We begin by briefly discussing the history of phage therapy and its recent medical successes, before identifying characteristics that may make it particularly well-suited to addressing some healthcare inequalities. We then review the ethical and regulatory challenges associated with the broader use of phage therapy in medicine and make suggestions to address them. Lastly, we identify the biological obstacles associated with wider use and outline the lines of research inquiry that could resolve or mitigate these issues. Importantly, these research recommendations are pertinent to both basic and applied scientists in research fields related to phage therapy. They represent ways in which scientific researchers can contribute not just to scientific progress but also progress towards greater healthcare equity. Holistically, we aim to draw attention to the immense potential of phage therapy in improving healthcare equity, while also identifying the research gaps that need to be addressed to realize a more comprehensive application of the method. We also emphasize that, while this review focuses on the development of phage therapy for human bacterial infections, much of the ethical analysis and many of the research suggestions apply to the use of bacteriophages in food production, agriculture, and veterinary medicine [30,31,32,33,34,35].
The History and Promise of Phage Therapy
Phage therapy has a rich history, documented extensively in prior reviews and scholarly books [19,20,36,37,38]. Bacteriophage research began in the early 1900s, starting with the independent discovery of phages through the work of microbiologists Frederik Twort and Félix d’Hérelle. Whereas Twort was the first to describe a ‘transparent material’ that inhibited bacterial growth [39], d’Hérelle conceived the idea of an obligate parasite of bacteria termed bacteriophage or “bacteria-eater” [40]. Immediately, d’Hérelle established the field of phage therapy by recognizing these microbes had therapeutic potential for treatment of bacterial diseases; in 1919, he successfully used phage to treat chickens infected with Salmonella gallinarum [41,42]. Soon after, d’Hérelle attempted to treat human infections, demonstrating in 1921 that five patients with bacillary dysentery were successfully treated with a phage that infects Shigella dysenteriae [41,43]. By 1927, clinical trials were underway in India, which showed that mortality of cholera disease (caused by Vibrio cholerae) decreased from 62.8% in control groups to 8.1% in phage-treated groups [44]. Relatedly, d’Hérelle noted that anti-cholera phage could be introduced into drinking wells of rural villages during an outbreak, to address epidemic spread and prevent additional infections from occurring [44].
Despite d’Hérelle’s early breakthroughs, other scientists pursued the therapeutic and prophylactic potential of phage with varying success, for several reasons. First, phages tend to be highly specific in killing only a subset of genotypes of a target bacterial pathogen, indicating that prior characterization of phage susceptibility is warranted before attempting therapy. In 1923, Beckerish and Hauduroy used phage successfully to reduce bacterial load in the blood of patients with typhoid fever [45], whereas the following year, Smith [46] was unsuccessful in using phage on a similar patient population; a failure likely stemming from unknowingly using phage with a narrow host range [45]. d’Hérelle himself acknowledged this weakness, attributing the success of his early trials to careful choice of phage capable of infecting the causative bacterial agent [41]. Second, early methods for bulk-manufacturing therapeutic phage were likely contaminated with debris from lysed bacteria. Due to insufficient purification, the potential benefits of phage therapy were difficult to separate from the confounding effects of bacterial-antigen contaminants [47]. Third, early pharmacokinetic experiments showed that phages were rapidly removed from the body via the spleen, raising concerns about the sustained efficacy of phage treatment within the body [48]. Fourth, pioneering molecular biology studies used lytic phage selection to estimate spontaneous mutation rates of bacteria and demonstrated that bacteria were readily capable of evolving resistance to lytic phage attack [49]. Lastly, early studies demonstrated that in vitro laboratory experiments involving phage and bacteria did not always align with experimental outcomes observed in vivo [50,51,52]. Comprehensive evaluations of phage therapy by the American Medical Association in the 1930s and 1940s yielded mixed reviews but recognized its potential [53].
With these many perceived problems, Western medicine showed waning interest in phage therapy relative to newly discovered antibiotics, trending away from phage technology by the 1970s. In stark contrast, physicians and scientists in the then USSR, Poland, and elsewhere continued to develop phage therapy in earnest; the legacy remains evident in locales such as the George Eliava Institute of Bacteriophages in Tbilisi, Georgia, which has been operating since 1923. Fast forward to the current day, when the World Health Organization has alerted that the rise of antibiotic-resistant bacteria poses an increasing public health problem, threatening lives and economies throughout the world [54]. Thus, as bacterial pathogens continue to evolve resistance against past and recently approved antibiotics across all classes and compounds of these chemical agents, phage therapy is experiencing a resurgence of interest and reconsideration by the West. Increasing numbers of emergency and compassionate phage treatments are reported in countries where phage therapy is not currently approved [55,56]. These are cases where patients are given otherwise unauthorized therapies due to intractable illnesses that have failed to respond to authorized treatments [57]. Recent reviews highlight the general safety and efficacy of personalized phage treatments [58,59]. In countries like Belgium, legislation has been adopted that allows phage therapy to be routinely used under magistral preparation. This enables physicians and pharmacists to prepare a combination of pre-approved phages on a case-by-case basis for patients [60]. In other countries, such as the USA, numerous clinical trials are underway that aim to demonstrate the safety and efficacy of phages for specific infections [61], a necessary step in the approval of phage treatments as labeled drugs, which would make these therapies widely available. Thus, as evidence mounts that phages can be safely and effectively used as adjuvants alongside chemical antibiotics or as replacements for these failing drugs, a growing concern is that personalized phage treatments offer possible life-saving technologies, which, unfortunately, are not accessible to all who could benefit [62]. This demonstrates that even medical interventions that clearly have utility to patient populations can raise ethical issues.
How Phage Therapy Can Advance Healthcare Equity
The formal principle of justice that is traditionally attributed to Aristotle is fundamental to our understanding of equity. In ethics, a principle is a general guideline that assists us in deciding which behaviors are right or wrong by specifying particular considerations as ethically relevant. The formal principle of justice requires that equals should be treated equally and those who are unequal should be treated unequally [63]. Equity can be understood as a narrower instantiation of the formal principle of justice, in that when two parties are equal (in the respect relevant to the particular opportunities under consideration), they should not have preventable or avoidable disparities between them in their access to opportunities [64]. Importantly, healthcare equity does not dictate that relevantly equal individuals ought to have precisely the same health outcomes, but rather that they should have relevantly equal opportunity to access healthcare. Returning to the example of women’s suffrage, adult men and adult women are not relevantly different (i.e., unequal) in respect to their capacity for political participation. Both groups engage with and are represented by the government, and both possess the capacity for human logic and reason. It is also functionally and logistically possible to permit both groups to vote. Thus, only permitting adult men (and not adult women) to vote is a politically inequitable outcome. Furthermore, note that neither men nor women need to actually vote in order for this to be equitable in this way; equity requires that there is no unfair difference in their opportunity to vote that is avoidable or remediable. This same rationale applies when evaluating whether access to healthcare is equitable for different groups.
Healthcare disparities arise from a combination of social, economic, political, and systemic factors that both structural conditions and individual-level barriers can shape [65,66,67]. Healthcare inequity manifests when these disparities appear amongst equals, and these inequalities are both unfair and avoidable or remediable. For instance, people who reside in rural areas are not relevantly different in an ethical sense from those who live in urban areas. However, urban areas tend to have a higher relative abundance of healthcare services. This means that rural populations can often face an inequitable shortage of healthcare resources when compared to urban populations [68]. On an individual level, persons in rural communities often also have less access to health information, which can lead to an increase in detrimental health behaviors and outcomes [69]. While some disparities in healthcare access between these patient groups are not feasibly avoidable or remediable (e.g., the distance to the nearest level 1 trauma center for an isolated rural community), we nonetheless have ethical reasons to address disparities when feasible. Health outcomes are influenced by both genetic factors and environmental exposure throughout our lifespans. While we have no control over the genetics we receive at birth, a person’s environment is often influenced, at least in part, by non-biological factors such as class status, geography, and the built environment [70,71]. These factors are avoidable in the sense that they are not inherent to the group and are societally constructed and dictated. Thus, preventing or remedying these barriers enables individuals in the group to pursue healthcare without facing additional hardship due to their status as group members. Here, we highlight that while phage therapy development can promote healthcare equity and facilitate the formal principle of justice, it can also promote other widely accepted core bioethical principles (See Sidebar 1).
Sidebar 1. Phage Therapy and the Core Principles of Bioethics
This targeted review focuses on the ways phage therapy can facilitate increased equity in healthcare. As such, our ethical analysis primarily focuses on the principle of justice and how phage therapy could promote it. However, phage therapy can also be ethically supported through its promotion of other core bioethical principles: autonomy, beneficence, and non-maleficence. In many instances, one action or policy can be supported by multiple principles.
Autonomy
Autonomy refers to a person’s rational capacity for self-determination and self-governance. In medicine, the principle of respect for autonomy affirms a person with decision-making capacity’s right to make informed and voluntary decisions about their healthcare and health information [63]. Providers should act in ways that support, protect, and promote this right. Generally, autonomous individuals should be allowed to hold views, make choices, and take actions based on their preferences and desires, unless there are morally relevant reasons to restrict them (such as the need to isolate someone with a highly infectious and potentially fatal disease from others that are vulnerable to infection). The principle of autonomy is impeded in healthcare and research by several factors, including, but not limited to, socioeconomic disparities that limit freedom of choice, as well as paternalistic medical care practices, cultural differences, and a lack of informed consent [72,73,74]. Broadening access to phage therapy can help facilitate autonomy by promoting healthcare access and increasing patients’ ability to make free decisions by mitigating the constraints of low resources or access. Development of phage therapy infrastructure could also increase independence for LMICs, as moving away from the established pharmaceutical industry of the HICs would allow for a greater degree of self-governance without foreign influence [75].
Beneficence
The principle of beneficence states that we ought to do good to others by advancing their well-being and preventing or removing harm from them. In medicine, the principle of beneficence affirms that providers should act in others’ (typically patients) best interests, to promote the “good” (typically measured by health outcome) they receive, and to prevent or remove harm from them [63]. Beneficence is also one of the primary motivators of biomedical research and plays a significant role in determining which projects are funded [76]. It is impeded by resource limitations, incentives that are not connected to patient well-being, biased research practices, and biases in healthcare workers [77,78]. Improvements in health equity typically improves access for underserved populations and are likely to have a net neutral impact on higher socioeconomic classes. However, if equity requires redistribution, it can lead to a reduction in beneficence for (or harm to) some individuals or groups [79]. Increased accessibility to phage therapy can improve beneficence across all groups by creating more favorable health outcomes and serving as an accessible and effective alternative to antibiotics.
Non-maleficence
The principle of non-maleficence states that we ought not inflict harm (intentionally or unintentionally) [63]. In medicine, the principle of non-maleficence affirms that providers should not cause pain, suffering, incapacitation, or death unless necessary for some important medical goal. For example, inflicting temporary pain through an injection may be justified for a blood test or vaccination. This principle is foundational to medicine and is arguably derived from the Hippocratic Oath [80]. In research, clinical trials test for the absence of harm before the presence of benefit, and institutional review boards (IRBs) work to balance benefits and harms in research [81,82]. Future use of phage therapy can promote non-maleficence by providing an accessible alternative to antibiotics that, in turn, reduces the harms associated with antimicrobial resistance caused by excessive antibiotic use [83,84].
Lower socioeconomic groups face a disproportionate burden of infectious diseases [26,85]. This is seen both in differences in disease risk for lower-income individuals compared to higher-income residents of the same country and in differences in disease incidence between HICs and LMICs around the world [86,87]. The spread of antibiotic resistance threatens to increase both the general burden of pathogenic bacteria and the degree to which that burden is inequitably distributed across the socioeconomic spectrum [83,88]. The burden of infectious disease is greater amongst lower socioeconomic groups due to several interacting factors. These include, but are not limited to, overcrowding, unsafe housing, poor sanitation, low water and food quality, proximity to pests and disease vectors, less access to adequate medical care, food insecurity, high-risk employment, and lower rates of health literacy [24,25,26]. The proliferation of antibiotic resistance may worsen the burden of infectious disease (regardless of socioeconomic status) by creating greater scarcity of therapeutically effective drugs and stressing already strained medical systems. For populations that already struggle to access conventional antibiotics, which have been available for decades and are more readily accessible to those from higher socioeconomic backgrounds, this may present a particularly salient issue. Furthermore, as we attempt to blunt the evolution and spread of antibiotic resistance by limiting societal use of antibiotics, those who already face an increased chance of pathogen exposure will also be asked to limit their use of antibiotics [84]. This presents an equity issue akin to that faced by LMICs seeking to further develop fossil fuel infrastructure in the era of climate change [89,90]. While individuals in LMICs have not been the primary users or beneficiaries of antibiotics, and even though they are in arguably the greatest need of antibiotics, they will be asked to sacrifice their use to achieve a broader societal goal (continued antibiotic efficacy).
Phage therapy can directly promote greater healthcare equity by improving access to antimicrobials through the removal or alleviation of logistical and financial barriers that contribute to these disparities. This is due to both the biological properties of bacteriophages and the current state of the methods that exist for their isolation, purification, and therapeutic deployment. For one, bacteriophages can be cheaper to isolate and produce compared to traditional antibiotics, with estimated manufacturing costs often lower than those of antibiotics [28,29,91]. Phage therapy can also use low dosages, because phages self-amplify on target bacteria [28,29]. These reduced production costs and low dosage requirements could result in reduced consumer costs and directly respond to calls from academia and the public for more research on less costly therapies that benefit vulnerable populations [92]. Secondly, bacteriophages can have less stringent storage requirements compared to antibiotics, and can be feasibly stored at room temperature [93,94,95]. This avoids the refrigeration requirement of some antibiotics, and, in conjunction with the lowered production costs and dosage requirements, can facilitate wider distribution compared to traditional methods.
Another benefit is that phages are naturally occurring and abundant, and methods for their isolation and replication in the laboratory are widely available and reasonably accessible [28,91,96]. For example, there are numerous undergraduate and secondary school modules and courses focused on phage discovery, characterization, and genomics [97,98,99,100]. This means that phages can be continuously isolated from the environment and then trained to use against pathogen strains of interest using laboratory evolution and engineering techniques [101,102,103]. This is particularly advantageous for developing alternative therapies against pathogens of rising global concern due to the spread of antibiotic resistance, like ESKAPE pathogens (Enterococcus faecium, Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Enterobacter spp.)[104]. Lastly, because these techniques are in the public domain and have a lower barrier to entry, further development of phage therapy could also enable greater self-determination in LMICs through a decreased reliance on the international pharmaceutical industry [75,105]. For example, collections of locally isolated and pre-characterized phages could be used on a national or regional level to treat infections. These “phage banks” are already present in multiple regions and could be particularly beneficial for LMICs [106,107].
Challenges and Recommendations for Equity-Oriented Phage Therapy Research and Development
For phage therapy to realize its full potential in addressing the burden of bacterial infections and improving healthcare equity, efforts must be dedicated to addressing several outstanding biological and ethical challenges. These generally relate to the development of therapeutic bacteriophages, the optimal protocols for prescribing those bacteriophages, biases in the pathogens investigated for bacteriophage therapy potential, difficulties in establishing regulations, issues with informed consent, and representation in clinical trials and amongst those receiving benefits during development. In addition to identifying challenges associated with phage therapy, we also recommend lines of biological and ethical inquiry that will help address these challenges and facilitate the desired outcomes.
Ethical and Regulatory Challenges and Recommendations
Because phage therapy and its research have been limited in recent decades, especially outside of the Former Soviet Union and other Eastern Bloc nations, there is limited knowledge about phage therapy amongst clinical researchers, healthcare providers, and potential research participants. These shortcomings pose an ethical challenge regarding informed consent for patient treatment and research, particularly in clinical trials. In this context, it is challenging to obtain informed consent from research participants as they often have a limited understanding of phages, and clinical researchers are currently not well equipped to provide them with sufficient information. For example, one issue found in research on public opinion on phage therapy is hesitancy inherently related to being given active viral particles, stressing the importance of how therapies are framed to patients [108]. Given this limitation, we recommend that clinical researchers develop informed consent guidelines specifically designed to address this limitation by providing both general information about phage therapy and how it is different from relevant alternatives (e.g., antibiotics) as well as information specific to the trial itself. To further address this challenge, clinical researchers should adopt evidence-based improvements to the informed consent process, such as interactive one-on-one consent processes with feedback or teach-back components [109,110].
Most phage therapy use in the Western world has been limited to compassionate (expanded) use clinical trials [55,56,61]. To widen the use of phage therapy beyond compassionate care access, several regulatory and intellectual property issues must be sufficiently addressed [111,112,113]. Some of these have already appeared during the process of approving phage therapy for compassionate use. For instance, in the European Union (EU), there was substantial debate about whether phage therapy should be considered as an advanced therapy medicinal product or a biological medicinal product [114]. Relatively small categorical differences like this can cause significant differences in the development and regulation process. Currently, phage therapy regulations vary considerably between countries, even among those that have regularly used phage therapy [21]. This can introduce barriers for researchers collaborating across countries, as well as for patients. Ethicists, legal experts, health professionals, and phage researchers should be consulted to help regulatory bodies develop equitable and safe guidelines. Similarly, establishing a standardized good manufacturing practice (GMP) is of utmost importance before wider expansion [115]. Lastly, for increased investment from private industry, intellectual property protections (IPP) and patenting laws must be clarified on a country-by-country basis. For instance, judicial systems around the world have generally ruled that naturally occurring forms of life, including their specific genetic code, cannot be patented [116]. However, laws remain undefined regarding the patenting of novel methods using naturally occurring biological materials (e.g., phage cocktails, engineered phages, etc.). Ultimately, private entities may be most likely to profit from phage therapy by patenting cocktail treatments or bioengineered phage genomes, as has been successfully, and sometimes controversially, done with domesticated crops in the agricultural industry [117]. To limit the marginalization of LMICs, HIC patent laws should consider the social value of the technologies being considered or pursue incentive programs for companies that develop socially valuable but unprofitable treatments [116].
While phage therapy presents unique opportunities to assist underserved populations, like most new biomedical interventions, it is likely to be more available to the wealthy, urban, and well-connected when first available. Despite this, the development and allocation of such interventions is ethically defensible [118]. This disproportionate availability occurs because the wealthy and well-connected are able to afford new and expensive medical interventions and are more likely to live near (or be able to easily travel to) advanced medical facilities. Even initiatives designed explicitly to make new interventions available to the most needy are subject to this effect. For example, setting up a COVID-19 vaccination site in the initial rollout in a neighborhood that had the highest case rates in Manhattan was undermined by the fact that the first recipients of that vaccine were those who were able to travel from elsewhere in New York City and New York state [119]. While this was inequitable insofar as there was an unfair and avoidable or remediable difference between population groups, it did not make the development of the COVID-19 vaccine (nor the setup of the vaccination site) ethically indefensible. After all, the COVID-19 vaccine prevented significant death and disease, and later became more widely available amongst different populations [120,121]. Analogously, even if phage therapy is initially more available to the wealthy, urban, and well-connected during and after its initial development, it does not make such development or its initial availability ethically wrong. Instead, phage therapy researchers should pursue initiatives that minimize unfair and avoidable differences between potential beneficiaries of phage therapy, both during development and after initial availability. Furthermore, given the aforementioned lower production costs, low dosage requirements given phage ability to self-amplify on target bacteria, less stringent storage requirements, and natural availability of phages, it is likely that phage therapy can be produced and distributed more equitably than many other novel biomedical interventions.
Lastly, as with all research, biases exist in the allocation of funding and the selection of pathogens for investigation. Inequalities in research funding can lead to inequities when they contribute to a disproportionate burden of disease amongst a particular group that is no less deserving of healthcare than another group. Inequity in research funding can worsen existing health disparities and lead to populations facing dual marginalization of inadequate access to treatment and insufficient research funding to create new therapies. To promote a more equitable distribution of research efforts targeting bacteria for phage therapy, pathogens of disproportionate concern in LMICs must receive attention commensurate with their burden. Several of the most problematic bacteria in terms of antibiotic resistance are widely distributed globally, so advances in phage therapy for these pathogens are likely to be beneficial across countries. However, there are several bacterial illnesses associated with poverty that are unlikely to receive significant investment due to their low burden in wealthy nations and thus would require direct attention. This includes less studied diseases like Yaws (a chronic skin infection caused by Treponema pallidum), which receives relatively little funding, as well as diseases like Tuberculosis (TB; caused by Mycobacterium tuberculosis), which receives significant research funding but remains prevalent in many LMICs [122]. Investment in regional phage banks and centers could address these concerns by focusing on bacteria of local importance. Primary investigators in HICs can also support these efforts by prioritizing research into bacterial pathogens that are important in LMICs and establishing international collaboration with researchers based in LMICs. However, these relationships can present ethical challenges due to the power imbalance between researchers and should be prepared for in advance [123,124]. Additionally, funding agencies based in HICs can continue to provide capital to investigators from LMICs, supporting basic and applied research [125].
Biological Challenges and Recommendations
Numerous challenges must be addressed for phage therapy to become generally useful and available to patients worldwide. The longstanding practice of phage therapy, beginning roughly 100 years ago, shows overwhelming evidence that safety is not a major concern; for countries such as Russia and Poland with a history of phages as approved therapies, as well as those like Canada and the UK, where phage therapy is still experimental, very few significant adverse events are reported [59,126,127]. Phages are natural members of human microbiomes and have been “generally recognized as safe” for use in food production, receiving the designation by the US Food and Drug Administration in 2006 [57]. However, characterization of phage therapy candidates is essential, especially subjecting these viruses to whole-genome sequencing to confirm clinical findings and ensure they do not harbor toxin or other genes that could threaten patient health. Examples of phage production pipelines and their standardization are described in the literature [128,129]. It is nevertheless advisable to continue conducting research on best practices for efficiently manufacturing phages, to ensure that doses are prepared with minimal toxicity. This includes essential steps like removing harmful bacterial debris that could prompt adverse physiological responses in patients. Whereas these research efforts should benefit all patient communities, here we focus on recommended research that addresses biological challenges pertinent to LMICs, where phage therapy development has been slower or nonexistent to date.
Perhaps the foremost consideration is that hospital and clinical settings are highly variable across different countries and communities. For example, interruptions in electricity may occur in some locales, either spontaneously or because of planned power outages that help maintain stressed electrical grids. Whether planned or not, intermittent supply of electricity makes equipment such as refrigerators and freezers unreliable for storing phages and phage doses at low temperatures, and some settings (e.g., rural communities) may lack electricity altogether. This challenge suggests that further research efforts should focus on developing methods for preserving phages at ambient temperatures, as this may be beneficial or even necessary. Phage lyophilization could be a worthwhile alternative. Lyophilization (or ‘freeze drying’) is a low temperature dehydration process that involves freezing a product and lowering pressure, so that ice is removed by sublimation. Beyond its historical use in food storage, the process is a relatively inexpensive and classic method for obtaining a ‘phage powder’ that can be stored at ambient temperatures, and later reanimated via rehydration [130]. Other recently described methods are also useful for achieving phage powders, such as spray-drying (concentrated liquid atomized and exposed to hot air to evaporate water) and hot-air-drying (pre-treating sample with ethyl oleate and potassium carbonate solutions, then exposing to high temperature for evaporation) [95]. The benefit is that these methods can preserve phages without refrigeration, whereas the obvious cost is that production still relies on specialized electrical equipment. Nevertheless, if phage powders can be produced at scale within a centralized location with reliable electricity/equipment, these formulations can be distributed to various locations where electrical service is weak or absent. The above considerations suggest many areas for basic research: improved ways to bulk manufacture phage powders and efficiently distribute them; determining which phages (strains, families) can be reanimated from powder form while preserving high titers; identifying mutations responsible for increased phage stability under desiccation, or at elevated temperatures, and the underlying mechanisms responsible [131,132].
Strategies for phage delivery to the site of infection vary. This is another benefit of phage therapy compared to antibiotics, which can be limited to a single method of distribution, such as injection via a needle [133]. For example, topical application of phages has shown promise for treating skin wounds and burn injuries [134]. Intra-articular delivery appears to be effective for managing prosthetic joint infections (independently or as part of debridement, antibiotics, and implant retention (DAIR)) [135,136]. Alternatively, nebulizer delivery (inhalation of droplets using solutions containing phages) may be advisable when addressing pulmonary infections of the lower respiratory tract [56,137,138,139,140]. Intravenous (IV) delivery may be ideal following proper source control and if the exact infection site is known. In principle, blood circulation may allow administered phages to travel to areas where antibiotic concentration is unable to eradicate bacteria or penetrance is insufficient, and introduction of a replicating phage may reduce burden [141]. An issue is that some of these strategies rely on specialized equipment such as nebulizers, although evidence suggests that the exact make/model may be irrelevant for ensuring efficient phage delivery to organs like the lung [142]. Conditions in resource-limited settings may necessitate the least expensive and most generalized delivery strategy, such as IV, despite valid concerns that this approach may increase the likelihood of stimulating immunity against phages, thereby reducing the future ability to re-administer them to the same patient [141,143]. Here, we advocate for additional research on the interactions between phages and human immunobiology to determine which phages, alone or in combination (cocktails), are least stimulatory and elucidate the reasons why. Further, we call for more research into the optimal phage delivery strategy for a range of bacterial illnesses and their pathologies.
These research efforts would ultimately benefit an improved understanding of phage therapy in all clinical settings with a significant impact on LMICs. However, targeted research efforts could specifically address infections relevant to patient communities in LMICs and help deal with these issues more directly. For some bacterial threats that are endemic to these regions, a subset of the population – such as young children, the elderly, individuals in displacement camps, those experiencing severe poverty and malnutrition –experiences the highest disease burden. Here, it is possible that phage interactions with human immunobiology can differ according to age and physical condition. For example, in some LMICs, diarrheagenic bacterial pathogens pose greater mortality threats for children under the age of five because of malnutrition and its effects on the immune system [144]. If potable water is scarce and rehydration therapy is unavailable, phage therapy may provide a temporary alternative until sufficient clean water is made available. While more studies investigating phage therapy for diarrheagenic diseases are needed [145], Western scientists have largely ignored phage therapy research targeting such bacteria in LMICs due to reduced prevalence in HICs. This highlights a vital need to forge collaborations with physicians and scientists to develop these research efforts [27]. By the same logic, endemic bacterial diseases in LMICs and unequal infection burdens across sexes suggest that we may benefit from increased research into phage therapy for these illnesses and should examine how phages can interact with human immunobiology in concerns pertaining to urology and women’s health. For example, sexually transmitted infections (STIs) can impact women more severely due to their relatively exposed reproductive and urological systems, their increased risk of asymptomatic infection, and social stigmas related to women’s sexuality, which leads to decreased testing [146]. Several bacterial STIs have seen a rise in the prevalence of antibiotic resistance [147]. As it can with other bacteria, phage therapy could be used to treat these diseases in patients [148]. This is also true of bacterial urinary tract infections (UTI), which impact women in LMICs at a significantly higher rate than in HICs, with pregnant women facing an even higher risk [149]. Relatedly, a historical problem with clinical trials is the under enrollment (or exclusion) of female participants, causing sex-associated toxicity to be missed along the paths of drug development and approval [150]. It is crucial to avoid these potential problems in clinical trials for phage therapy development in countries like the USA, where personalized medicine is currently the only option, to ensure that phage-based drugs are safe and effective for the general public.
Conclusions
Phages have been used for medical treatment since shortly after their discovery, and have been used routinely in some parts of the world for almost 100 years [19,20]. As antibiotic resistance spreads around the globe, phage therapy has gained attention as a possible alternative to, or synergistic therapy with, antibiotics. In this paper, we have employed an interdisciplinary approach to explore how phage therapy might work to increase healthcare equity. This can be accomplished because of the ability of phage therapy to increase access to antimicrobials by removing or alleviating many of the logistical and financial barriers faced by disadvantaged populations. This can work to close disparities experienced by citizens of different socioeconomic statuses within the same nation, as well as the disparities that exist between HICs and LMICs. Biologically, we recommend research into the human immunological response to phage, including differences in that response between the sexes and during pregnancy, phage temperature stability, long-term storage stability, the development and study of methods for deployment, pharmacological strategies for synergistic or combination therapy, and increased investment in pathogens that specifically affect LMICs. Ethically, we recommend implementation (and continued evaluation) of improved methods for ensuring informed consent during clinical trials that address known deficiencies in knowledge about phage therapy, strategies for equitable participation during development and access in the initial deployment, development of a more robust intellectual property and regulatory framework, and greater investment in researching bacteria that disproportionately impact LMICs. Investment in the equity-related areas of research outlined in this manuscript (Figure 2) will elucidate pressing questions in phage biology, while simultaneously addressing key questions necessary for phage therapy to reach its full potential.
Summary Points
1. The global burden of bacterial infections is high and is expected to increase due to the proliferation of antibiotic resistance.
2. Phage therapy, the use of lytic viruses of bacteria to treat bacterial infections, is one therapeutic alternative that has been used to combat antibiotic resistant infections.
3. A potential benefit of the method is its capacity to enhance human health outcomes amongst lower socioeconomic populations.
4. Phage therapy can accomplish this due to lower manufacturing costs, less stringent storage requirements, and well-established and cost-effective methods for isolation and characterization.
5. Through these traits, phage therapy has the capability to increase healthcare equity (the absence of unfair, and avoidable or remediable differences in access to healthcare among different groups of people).
6. To facilitate these outcomes, researchers can focus on realms of research that are likely to directly benefit patients in low and middle-income countries (LMICs) and low socioeconomic populations in high-income countries (HICs).
7. These areas of research include topics in the natural and physical sciences, the medical sciences, regulatory science, intellectual property, and bioethics.
Funding
This research was financially supported by Yale University’s Center for Phage Biology and Therapy (BKC & PET), start-up funds provided by the Biology Department and the Provost Office at the University of South Carolina (JAL), and the National Science Foundation Postdoctoral Research Fellowship in Biology (Award Number: 2209109; JAL). Any opinions, findings, and conclusions or recommendations expressed in this material are those of the authors and do not necessarily reflect the views of the National Science Foundation or any of the authors’ home institutions.
Acknowledgments
We would like to thank the members of the Turner lab and the Center for Phage Biology and Therapy at Yale University for their assistance during the conception of this paper. We would also like to thank the members of the Tad Dallas Lab and the Lewis Lab at the University of South Carolina for their feedback during the manuscript editing process.
Conflicts of Interest
Yale University has an institutional conflict of interest related to this manuscript due to patented phage technologies developed at the University.
References
- GBD 2019 Antimicrobial Resistance Collaborators. Global mortality associated with 33 bacterial pathogens in 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 2022, 400(10369), 2221–48. [Google Scholar] [CrossRef]
- Lynch, M.F.; Tauxe, R.V.; Hedberg, C.W. The growing burden of foodborne outbreaks due to contaminated fresh produce: risks and opportunities. Epidemiology Infect. 2009, 137, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Savary, S.; Willocquet, L.; Pethybridge, S.J.; Esker, P.; McRoberts, N.; Nelson, A. The global burden of pathogens and pests on major food crops. Nat. Ecol. Evol. 2019, 3, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Maldonado-Miranda, JJ; Castillo-Pérez, LJ; Ponce-Hernández, A; Carranza-Álvarez, C. Chapter 19 - Summary of economic losses due to bacterial pathogens in aquaculture industry. In Bacterial Fish Diseases; Dar, GH, Bhat, RA, Qadri, H, Al-Ghamdy, KM, Hakeem, KR, Eds.; Academic Press, 2022; pp. 399–417. [Google Scholar]
- Niemi, JK; Foster, ed N; Kyriazakis, I; Barrow, P. 1 - The economic cost of bacterial infections. In Advancements and Technologies in Pig and Poultry Bacterial Disease Control; Academic Press, 2021; pp. 1–23. [Google Scholar]
- Gu, D.; Andreev, K.; Dupre, M.E. Major Trends in Population Growth Around the World. China CDC Wkly. 2021, 3, 604–613. [Google Scholar] [CrossRef] [PubMed]
- Raleigh, V.S. World population and health in transition. BMJ 1999, 319, 981–984. [Google Scholar] [CrossRef]
- Liao, H.; Lyon, C.J.; Ying, B.; Hu, T. Climate change, its impact on emerging infectious diseases and new technologies to combat the challenge. Emerg. Microbes Infect. 2024, 13, 2356143. [Google Scholar] [CrossRef]
- Baker, R.E.; Mahmud, A.S.; Miller, I.F.; Rajeev, M.; Rasambainarivo, F.; Rice, B.L.; Takahashi, S.; Tatem, A.J.; Wagner, C.E.; Wang, L.-F.; et al. Infectious disease in an era of global change. Nat. Rev. Microbiol. 2022, 20, 193–205. [Google Scholar] [CrossRef]
- Mahon, M.B.; Sack, A.; Aleuy, O.A.; Barbera, C.; Brown, E.; Buelow, H.; Civitello, D.J.; Cohen, J.M.; de Wit, L.A.; Forstchen, M.; et al. A meta-analysis on global change drivers and the risk of infectious disease. Nature 2024, 629, 830–836. [Google Scholar] [CrossRef]
- Luepke, K.H.; Suda, K.J.; Boucher, H.; Russo, R.L.; Bonney, M.W.; Hunt, T.D.; Mohr, J.F. Past, Present, and Future of Antibacterial Economics: Increasing Bacterial Resistance, Limited Antibiotic Pipeline, and Societal Implications. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2017, 37, 71–84. [Google Scholar] [CrossRef]
- Frieri, M; Kumar, K; Boutin, A. Antibiotic resistance. Journal of Infection and Public Health 2017, 10(4), 369–78. [Google Scholar] [CrossRef]
- Dadgostar, P. Antimicrobial Resistance: Implications and Costs. Infect. Drug Resist. 2019, 12, 3903–3910. [Google Scholar] [CrossRef] [PubMed]
- Naghavi, M; Vollset, SE; Ikuta, KS; Swetschinski, LR; Gray, AP; et al. Global burden of bacterial antimicrobial resistance 1990–2021: a systematic analysis with forecasts to 2050. The Lancet 2024, 404(10459), 1199–1226. [Google Scholar] [CrossRef] [PubMed]
- Giubilini, A; Savulescu, J. Moral Responsibility and the Justification of Policies to Preserve Antimicrobial Effectiveness. In Ethics and Drug Resistance: Collective Responsibility for Global Public Health; Jamrozik, Selgelid, M, Eds.; Springer International Publishing: Cham, 2020; Volume 5, pp. 141–54. [Google Scholar]
- Laxminarayan, R.; Matsoso, P.; Pant, S.; Brower, C.; Røttingen, J.-A.; Klugman, K.; Davies, S. Access to effective antimicrobials: a worldwide challenge. Lancet 2016, 387, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Bacteriophages: Biology and Applications; Kutter, E, Sulakvelidze, A, Eds.; CRC Press: Boca Raton, 2004; p. 528 pp. [Google Scholar]
- Kortright, K.E.; Chan, B.K.; Koff, J.L.; Turner, P.E. Phage Therapy: A Renewed Approach to Combat Antibiotic-Resistant Bacteria. Cell Host Microbe 2019, 25, 219–232. [Google Scholar] [CrossRef]
- Summers, W.C. The strange history of phage therapy. Bacteriophage 2012, 2, 130–133. [Google Scholar] [CrossRef]
- Chanishvili, N. Phage Therapy—History from Twort and d’Herelle through soviet experience to current approaches. Adv. Virus Res. 2012, 82, 3–40. [Google Scholar]
- Yang, Q.; Le, S.; Zhu, T.; Wu, N. Regulations of phage therapy across the world. Front. Microbiol. 2023, 14, 1250848. [Google Scholar] [CrossRef]
- Steele, A.; Stacey, H.J.; de Soir, S.; Jones, J.D. The Safety and Efficacy of Phage Therapy for Superficial Bacterial Infections: A Systematic Review. Antibiotics 2020, 9, 754. [Google Scholar] [CrossRef]
- Organization WH. Health equity WPRO; World Health Organization International, 2025; Available online: www.who.int.
- A Bhutta, Z.; Sommerfeld, J.; Lassi, Z.S.; A Salam, R.; Das, J.K. Global burden, distribution, and interventions for infectious diseases of poverty. Infect. Dis. Poverty 2014, 3, 1–7. [Google Scholar] [CrossRef]
- Braveman, P.; Egerter, S.; Williams, D.R. The Social Determinants of Health: Coming of Age. Annu. Rev. Public Heal. 2011, 32, 381–398. [Google Scholar] [CrossRef]
- Ayorinde, A.; Ghosh, I.; Ali, I.; Zahair, I.; Olarewaju, O.; Singh, M.; Meehan, E.; Anjorin, S.S.; Rotheram, S.; Barr, B.; et al. Health inequalities in infectious diseases: a systematic overview of reviews. BMJ Open 2023, 13, e067429. [Google Scholar] [CrossRef]
- Nagel, T.E.; Chan, B.K.; De Vos, D.; El-Shibiny, A.; Kang'EThe, E.K.; Makumi, A.; Pirnay, J.-P. The Developing World Urgently Needs Phages to Combat Pathogenic Bacteria. Front. Microbiol. 2016, 7, 882. [Google Scholar] [CrossRef]
- Loc-Carrillo, C.; Abedon, S.T. Pros and cons of phage therapy. Bacteriophage 2011, 1, 111–114. [Google Scholar] [CrossRef] [PubMed]
- Kutter, E.; De Vos, D.; Gvasalia, G.; Alavidze, Z.; Gogokhia, L.; Kuhl, S.; Abedon, S.T. Phage Therapy in Clinical Practice: Treatment of Human Infections. Curr. Pharm. Biotechnol. 2010, 11, 69–86. [Google Scholar] [CrossRef]
- Chaudhary, V.; Kajla, P.; Lather, D.; Chaudhary, N.; Dangi, P.; Singh, P.; Pandiselvam, R. Bacteriophages: a potential game changer in food processing industry. Crit. Rev. Biotechnol. 2024, 44, 1325–1349. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Han, G.; Li, Z.; Cun, S.; Hao, B.; Zhang, J.; Liu, X. Bacteriophage therapy in aquaculture: current status and future challenges. Folia Microbiol. 2022, 67, 573–590. [Google Scholar] [CrossRef] [PubMed]
- García-Anaya, M.C.; Sepulveda, D.R.; Sáenz-Mendoza, A.I.; Rios-Velasco, C.; Zamudio-Flores, P.B.; Acosta-Muñiz, C.H. Phages as biocontrol agents in dairy products. Trends Food Sci. Technol. 2020, 95, 10–20. [Google Scholar] [CrossRef]
- Balogh, B.; Jones, J.B.; Iriarte, F.B.; Momol, M.T. Phage Therapy for Plant Disease Control. Curr. Pharm. Biotechnol. 2010, 11, 48–57. [Google Scholar] [CrossRef]
- Loponte, R.; Pagnini, U.; Iovane, G.; Pisanelli, G. Phage Therapy in Veterinary Medicine. Antibiotics 2021, 10, 421. [Google Scholar] [CrossRef]
- Villalpando-Aguilar, J.L.; Matos-Pech, G.; López-Rosas, I.; Castelán-Sánchez, H.G.; Alatorre-Cobos, F. Phage Therapy for Crops: Concepts, Experimental and Bioinformatics Approaches to Direct Its Application. Int. J. Mol. Sci. 2022, 24, 325. [Google Scholar] [CrossRef]
- Fruciano, D.E.; Bourne, S. Phage as an Antimicrobial Agent: D’herelle’s Heretical Theories and Their Role in the Decline of Phage Prophylaxis in the West. Can. J. Infect. Dis. Med Microbiol. 2006, 18, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Kutateladze, M.; Adamia, R. Bacteriophages as potential new therapeutics to replace or supplement antibiotics. Trends Biotechnol. 2010, 28, 591–595. [Google Scholar] [CrossRef] [PubMed]
- Salmond, G.P.C.; Fineran, P.C. A century of the phage: past, present and future. Nat. Rev. Microbiol. 2015, 13, 777–786. [Google Scholar] [CrossRef] [PubMed]
- Twort, F. AN INVESTIGATION ON THE NATURE OF ULTRA-MICROSCOPIC VIRUSES. Lancet 1915, 186, 1241–1243. [Google Scholar] [CrossRef]
- d’Herelle, MF. Sur un microbe invisible antagoniste des bacilles dysentériques. In Comptes rendus de l’Academie des Sciences; 1917; pp. 373–75. [Google Scholar]
- Ho, K. Bacteriophage Therapy for Bacterial Infections: Rekindling a Memory from the Pre-Antibiotics Era. Perspect. Biol. Med. 2001, 44, 1–16. [Google Scholar] [CrossRef]
- d’Herelle, F; Smith, GH. The bacteriophage and its behavior; Williams & Wilkins: Baltimore, MD, 1926. [Google Scholar]
- Summers, W.C. Cholera and plague in India: The bacteriophage inquiry of 1927–1936. J. Hist. Med. Allied Sci. 1993, 48, 275–301. [Google Scholar] [CrossRef]
- d’Herelle, F; Malone, RH; Lahiri, MN. Studies on Asiatic cholera. 1930. [Google Scholar]
- Hadley, P. The Twort-D'Herelle Phenomenon: A Critical Review and Presentation of a New Conception (Homogamic Theory) Of Bacteriophage Action. J. Infect. Dis. 1928, 42, 263–434. [Google Scholar] [CrossRef]
- Smith, J. THE BACTERIOPHAGE IN THE TREATMENT OF TYPHOID FEVER. BMJ 1924, 2, 47–49. [Google Scholar] [CrossRef]
- Cowie, D; Hicks, W. Observations on the bacteriophage III. J. Lab. Clin. Med. 1932, 17, 685. [Google Scholar]
- Krestownikowa, W; Gubin, W. Die Verteilung and die Ausscheidung von Bak-teriophagen im Meerschweinchen-organismus bei subkutaner Applicationsart. J. Microbiol., Patolog. i. Infekzionnich bolesney 1925, 1(3). [Google Scholar]
- Luria, S.E.; Delbrück, M. Mutations of bacteria from virus sensitivity to virus resistance. Genetics 1943, 28, 491–511. [Google Scholar] [CrossRef] [PubMed]
- Riding, D. Acute Bacillary Dysentery in Khartoum Province, Sudan, with Special Reference to Bacteriophage Treatment: Bacteriological Investigation. Epidemiology Infect. 1930, 30, 387–401. [Google Scholar] [CrossRef] [PubMed]
- Eaton, MD; Bayne-Jones, S. Bacteriophage Therapy: Review of the Principles and Results of the use of Bacteriophage in the Treatment of Infections. JAMA 1934, 103(23), 1769–76. [Google Scholar] [CrossRef]
- Krueger, AP; Scribner, EJ. The Bacteriophage: Its Nature and its Theraputic Use. JAMA 1941, 116(20), 2269–77. [Google Scholar] [CrossRef]
- Summers, W.C. The Cold War and Phage Therapy: How Geopolitics Stalled Development of Viruses as Antibacterials. Annu. Rev. Virol. 2024, 11, 381–393. [Google Scholar] [CrossRef]
- Organization WH. WHO publishes list of bacteria for which new antibiotics are urgently needed; Geneva, Switzerland, Geneva, Switzerland, 2017. [Google Scholar]
- Pirnay, J.-P.; Djebara, S.; Steurs, G.; Griselain, J.; Cochez, C.; De Soir, S.; Glonti, T.; Spiessens, A.; Berghe, E.V.; Green, S.; et al. Personalized bacteriophage therapy outcomes for 100 consecutive cases: a multicentre, multinational, retrospective observational study. Nat. Microbiol. 2024, 9, 1434–1453. [Google Scholar] [CrossRef]
- Chan, B.K.; Stanley, G.L.; Kortright, K.E.; Vill, A.C.; Modak, M.; Ott, I.M.; Sun, Y.; Würstle, S.; Grun, C.N.; Kazmierczak, B.I.; et al. Personalized inhaled bacteriophage therapy for treatment of multidrug-resistant Pseudomonas aeruginosa in cystic fibrosis. Nat. Med. 2025, 31, 1494–1501. [Google Scholar] [CrossRef]
- Borysowski, J.; Górski. 2019. Ethics of Phage Therapy. In Phage Therapy: A Practical Approach, ed A Górski, R Międzybrodzki, J Borysowski, pp. 379–85. Cham: Springer International Publishing.
- Pires, D.P.; Meneses, L.; Brandão, A.C.; Azeredo, J. An overview of the current state of phage therapy for the treatment of biofilm-related infections. Curr. Opin. Virol. 2022, 53, 101209. [Google Scholar] [CrossRef]
- Uyttebroek, S.; Chen, B.; Onsea, J.; Ruythooren, F.; Debaveye, Y.; Devolder, D.; Spriet, I.; Depypere, M.; Wagemans, J.; Lavigne, R.; et al. Safety and efficacy of phage therapy in difficult-to-treat infections: a systematic review. Lancet Infect. Dis. 2022, 22, e208–e220. [Google Scholar] [CrossRef] [PubMed]
- Pirnay, J.-P.; Verbeken, G.; Ceyssens, P.-J.; Huys, I.; De Vos, D.; Ameloot, C.; Fauconnier, A. The Magistral Phage. Viruses 2018, 10, 64. [Google Scholar] [CrossRef] [PubMed]
- Hitchcock, N.M.; Nunes, D.D.G.; Shiach, J.; Hodel, K.V.S.; Barbosa, J.D.V.; Rodrigues, L.A.P.; Coler, B.S.; Soares, M.B.P.; Badaró, R. Current Clinical Landscape and Global Potential of Bacteriophage Therapy. Viruses 2023, 15, 1020. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.E.; Azeredo, J.; Buurman, E.T.; Green, S.; Haaber, J.K.; Haggstrom, D.; Carvalho, K.K.d.F.; Kirchhelle, C.; Moreno, M.G.; Pirnay, J.-P.; et al. Addressing the Research and Development Gaps in Modern Phage Therapy. PHAGE 2024, 5, 30–39. [Google Scholar] [CrossRef]
- Beauchamp, TL; Childress, JF. Principles of Biomedical Ethics, 8th ed.; Oxford University Press: New York, 2019; p. 512 pp. [Google Scholar]
- Rawls, J. A Theory of Justice, 2nd ed.; Oxford University Press: Cambridge, MA, 1999; p. 538 pp. [Google Scholar]
- Spencer, K.L.; Grace, M. Social Foundations of Health Care Inequality and Treatment Bias. Annu. Rev. Sociol. 2016, 42, 101–120. [Google Scholar] [CrossRef]
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.-J.R.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E. Socioeconomic Inequalities in Health in 22 European Countries. New Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef]
- Dickman, S.L.; Himmelstein, D.U.; Woolhandler, S. Inequality and the health-care system in the USA. Lancet 2017, 389, 1431–1441. [Google Scholar] [CrossRef]
- Reilly, M. Health Disparities and Access to Healthcare in Rural vs. Urban Areas. Theory Action 2021, 14, 6–27. [Google Scholar] [CrossRef]
- Chen, X; Orom, H; Hay, JL; Waters, EA; Schofield, E; et al. Differences in Rural and Urban Health Information Access and Use. The Journal of Rural Health 2019, 35(3), 405–17. [Google Scholar] [CrossRef]
- Evans, GW; Kantrowitz, E. Socioeconomic Status and Health: The Potential Role of Environmental Risk Exposure. Annual Review of Public Health 2002, 23((Volume 23), 303–31. [Google Scholar] [CrossRef]
- Iceland, J.; Wilkes, R. Does Socioeconomic Status Matter? Race, Class, and Residential Segregation. Soc. Probl. 2006, 53, 248–273. [Google Scholar] [CrossRef]
- Barnato, A.E. Challenges In Understanding And Respecting Patients’ Preferences. Heal. Aff. 2017, 36, 1252–1257. [Google Scholar] [CrossRef] [PubMed]
- Parascandola, M.; Hawkins, J.S.; Danis, M. Patient Autonomy and the Challenge of Clinical Uncertainty. Kennedy Inst. Ethic- J. 2002, 12, 245–264. [Google Scholar] [CrossRef] [PubMed]
- Ng, I.K. Informed consent in clinical practice: Old problems, new challenges. J. R. Coll. Physicians Edinb. 2024, 54, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Mulumba, M.; Oga, J.; Koomson, N.; Kara, T.-A.; Cynthia, A.N.; Forman, L. Decolonizing global health: Africa’s pursuit of pharmaceutical sovereignty. BMC Heal. Serv. Res. 2025, 25, 1–9. [Google Scholar] [CrossRef]
- National Comission for the Protection of Human Subjects of Biomedical and Behavioral Research. The Belmont report: Ethical principles and guidelines for the protection of human subjects of research. In U.S. Department of Health and Human Services; 1979. [Google Scholar]
- Huecker, MR; Shreffler, J. Ethical Issues in Academic Medicine. In StatPearls [Internet]; StatPearls Publishing, 2025. [Google Scholar]
- Fitzgerald, C.; Hurst, S. Implicit bias in healthcare professionals: a systematic review. BMC Med. Ethic 2017, 18, 1–18. [Google Scholar] [CrossRef]
- Norheim, O.F.; Asada, Y. The ideal of equal health revisited: definitions and measures of inequity in health should be better integrated with theories of distributive justice. Int. J. Equity Heal. 2009, 8, 40–40. [Google Scholar] [CrossRef]
- Askitopoulou, H.; Vgontzas, A.N. The relevance of the Hippocratic Oath to the ethical and moral values of contemporary medicine. Part II: interpretation of the Hippocratic Oath—today’s perspective. Eur. Spine J. 2018, 27, 1491–1500. [Google Scholar] [CrossRef]
- White, M.G. Why Human Subjects Research Protection Is Important. Ochsner J. 2020, 20, 16–33. [Google Scholar] [CrossRef]
- Varkey, B. Principles of Clinical Ethics and Their Application to Practice. Med Princ Pract. 2021, 30(1), 17–28. [Google Scholar] [CrossRef]
- Reid, L. Antimicrobial Resistance and Social Inequalities in Health: Considerations of Justice. In Ethics and Drug Resistance: Collective Responsibility for Global Public Health; Jamrozik, Selgelid, M, Eds.; Springer International Publishing: Cham, 2020; pp. 257–78. [Google Scholar]
- Adebisi, Y.A. Balancing the risks and benefits of antibiotic use in a globalized world: the ethics of antimicrobial resistance. Glob. Heal. 2023, 19, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Naghavi, M.; Mestrovic, T.; Gray, A.; Hayoon, A.G.; Swetschinski, L.R.; Aguilar, G.R.; Weaver, N.D.; Ikuta, K.S.; Chung, E.; E Wool, E.; et al. Global burden associated with 85 pathogens in 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Infect. Dis. 2024, 24, 868–895. [Google Scholar] [CrossRef] [PubMed]
- Emadi, M.; Delavari, S.; Bayati, M. Global socioeconomic inequality in the burden of communicable and non-communicable diseases and injuries: an analysis on global burden of disease study 2019. BMC Public Heal. 2021, 21, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Blackmon, S.; E Avendano, E.; Nirmala, N.; Chan, C.W.; A Morin, R.; Balaji, S.; McNulty, L.; Argaw, S.A.; Doron, S.; Nadimpalli, M.L. Socioeconomic status and the risk for colonisation or infection with priority bacterial pathogens: a global evidence map. Lancet Microbe 2024, 6, 100993–100993. [Google Scholar] [CrossRef]
- Keenan, K.; Corrêa, J.S.; Sringernyuang, L.; Nayiga, S.; Chandler, C.I.R. The social burden of antimicrobial resistance: what is it, how can we measure it, and why does it matter? JAC-Antimicrobial Resist. 2025, 7, dlae208. [Google Scholar] [CrossRef]
- Resnik, D.B. Environmental justice and climate change policies. Bioethics 2022, 36, 735–741. [Google Scholar] [CrossRef]
- Okereke, C. Climate justice and the international regime. WIREs Clim. Chang. 2010, 1, 462–474. [Google Scholar] [CrossRef]
- Skurnik, M.; Pajunen, M.; Kiljunen, S. Biotechnological challenges of phage therapy. Biotechnol. Lett. 2007, 29, 995–1003. [Google Scholar] [CrossRef]
- Reed, S.L.; McKerrow, J.H. Why Funding for Neglected Tropical Diseases Should Be a Global Priority. Clin. Infect. Dis. 2018, 67, 323–326. [Google Scholar] [CrossRef]
- Li, M.; Ke, W.-R.; Chang, R.Y.K.; Chan, H.-K. Long-term Storage Stability of Inhalable Phage Powder Formulations: A Four-Year Study. AAPS J. 2025, 27, 128. [Google Scholar] [CrossRef]
- Jończyk-Matysiak, E.; Łodej, N.; Kula, D.; Owczarek, B.; Orwat, F.; Międzybrodzki, R.; Neuberg, J.; Bagińska, N.; Weber-Dąbrowska, B.; Górski, A. Factors determining phage stability/activity: challenges in practical phage application. Expert Rev. Anti-infective Ther. 2019, 17, 583–606. [Google Scholar] [CrossRef] [PubMed]
- Wdowiak, M.; Paczesny, J.; Raza, S. Enhancing the Stability of Bacteriophages Using Physical, Chemical, and Nano-Based Approaches: A Review. Pharmaceutics 2022, 14, 1936. [Google Scholar] [CrossRef] [PubMed]
- Hyman, P. Phages for Phage Therapy: Isolation, Characterization, and Host Range Breadth. Pharmaceuticals 2019, 12, 35. [Google Scholar] [CrossRef] [PubMed]
- Williamson, R.P.; Barker, B.T.; Drammeh, H.; Scott, J.; Lin, J. Isolation and genetic analysis of an environmental bacteriophage: A 10-session laboratory series in molecular virology. Biochem. Mol. Biol. Educ. 2014, 42, 480–485. [Google Scholar] [CrossRef]
- Heller, D.M.; Sivanathan, V.; Asai, D.J.; Hatfull, G.F. SEA-PHAGES and SEA-GENES: Advancing Virology and Science Education. Annu. Rev. Virol. 2024, 11, 1–20. [Google Scholar] [CrossRef]
- Bittle, C; Brittain, K; Doore, SM; Dover, J; Bergland Drarvik, SM; et al. Phage Hunting in the High School Classroom: Phage Isolation and Characterization. The American Biology Teacher 2023, 85(8), 440–47. [Google Scholar] [CrossRef]
- Jordan, T.C.; Burnett, S.H.; Carson, S.; Caruso, S.M.; Clase, K.; DeJong, R.J.; Dennehy, J.J.; Denver, D.R.; Dunbar, D.; Elgin, S.C.R.; et al. A Broadly Implementable Research Course in Phage Discovery and Genomics for First-Year Undergraduate Students. mBio 2014, 5, e01051-13–13. [Google Scholar] [CrossRef]
- Lewis, J.A.; Morran, L.T. Advantages of laboratory natural selection in the applied sciences. J. Evol. Biol. 2022, 35, 5–22. [Google Scholar] [CrossRef]
- Peng, H.; A Chen, I. Phage engineering and the evolutionary arms race. Curr. Opin. Biotechnol. 2020, 68, 23–29. [Google Scholar] [CrossRef]
- Oromí-Bosch, A.; Antani, J.D.; Turner, P.E. Developing Phage Therapy That Overcomes the Evolution of Bacterial Resistance. Annu. Rev. Virol. 2023, 10, 503–524. [Google Scholar] [CrossRef]
- Miller, W.R.; Arias, C.A. ESKAPE pathogens: antimicrobial resistance, epidemiology, clinical impact and therapeutics. Nat. Rev. Microbiol. 2024, 22, 598–616. [Google Scholar] [CrossRef] [PubMed]
- Semin, S.; Güldal, D. Globalization of the Pharmaceutical Industry and the Growing Dependency of Developing Countries: The Case of Turkey. Int. J. Heal. Serv. 2008, 38, 379–398. [Google Scholar] [CrossRef] [PubMed]
- Nagel, T.; Musila, L.; Muthoni, M.; Nikolich, M.; Nakavuma, J.L.; Clokie, M.R. Phage banks as potential tools to rapidly and cost-effectively manage antimicrobial resistance in the developing world. Curr. Opin. Virol. 2022, 53, 101208–101208. [Google Scholar] [CrossRef] [PubMed]
- Resch, G.; Brives, C.; Debarbieux, L.; Hodges, F.E.; Kirchhelle, C.; Laurent, F.; Moineau, S.; Martins, A.F.M.; Rohde, C. Between Centralization and Fragmentation: The Past, Present, and Future of Phage Collections. PHAGE 2024, 5, 22–29. [Google Scholar] [CrossRef]
- McCammon, S.; Makarovs, K.; Banducci, S.; Gold, V. Phage therapy and the public: Increasing awareness essential to widespread use. PLOS ONE 2023, 18, e0285824. [Google Scholar] [CrossRef]
- Nishimura, A.; Carey, J.; Erwin, P.J.; Tilburt, J.C.; Murad, M.H.; McCormick, J.B. Improving understanding in the research informed consent process: a systematic review of 54 interventions tested in randomized control trials. BMC Med Ethic- 2013, 14, 28–28. [Google Scholar] [CrossRef]
- Glaser, J.; Nouri, S.; Fernandez, A.; Sudore, R.L.; Schillinger, D.; Klein-Fedyshin, M.; Schenker, Y. Interventions to Improve Patient Comprehension in Informed Consent for Medical and Surgical Procedures: An Updated Systematic Review. Med Decis. Mak. 2020, 40, 119–143. [Google Scholar] [CrossRef]
- Fauconnier, A. Phage Therapy Regulation: From Night to Dawn. Viruses 2019, 11, 352. [Google Scholar] [CrossRef]
- Verbeken, G.; De Vos, D.; Vaneechoutte, M.; Merabishvili, M.; Zizi, M.; Pirnay, J.-P. European Regulatory Conundrum of Phage Therapy. Futur. Microbiol. 2007, 2, 485–491. [Google Scholar] [CrossRef]
- De Vos, D; Verbeken, G; Quintens, J; Pirnay, J-P. Phage Therapy in Europe: Regulatory and Intellectual Property Protection Issues. In Phage Therapy: A Practical Approach; Górski, Międzybrodzki, R, Borysowski, J, Eds.; Springer International Publishing: Cham, 2019; pp. 363–77. [Google Scholar]
- Naureen, Z.; Malacarne, D.; Anpilogov, K.; Dautaj, A.; Camilleri, G.; Cecchin, S.; Bressan, S.; Casadei, A.; Albion, E.; Sorrentino, E.; et al. Comparison between American and European legislation in the therapeutical and alimentary bacteriophage usage. Acta Biomedica Atenei Parmensis 2020, 91, e2020023. [Google Scholar]
- Bretaudeau, L.; Tremblais, K.; Aubrit, F.; Meichenin, M.; Arnaud, I. Good Manufacturing Practice (GMP) Compliance for Phage Therapy Medicinal Products. Front. Microbiol. 2020, 11, 1161. [Google Scholar] [CrossRef] [PubMed]
- Anomaly, J. The Future of Phage: Ethical Challenges of Using Phage Therapy to Treat Bacterial Infections. Public Heal. Ethic- 2020, 13, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Barbu, E.M.; Cady, K.C.; Hubby, B. Phage Therapy in the Era of Synthetic Biology. Cold Spring Harb. Perspect. Biol. 2016, 8, a023879. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, G.O.; Emanuel, E.J.; Wertheimer, A. The Obligation to Participate in Biomedical Research. JAMA 2009, 302, 67–72. [Google Scholar] [CrossRef]
- Schwalbe, N.; Nunes, M.C.; Cutland, C.; Wahl, B.; Reidpath, D. Assessing New York City’s COVID-19 Vaccine Rollout Strategy: A Case for Risk-Informed Distribution. J. Urban Heal. 2024, 101, 923–933. [Google Scholar] [CrossRef]
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global impact of the first year of COVID-19 vaccination: a mathematical modelling study. Lancet Infect. Dis. 2022, 22, 1293–1302. [Google Scholar] [CrossRef]
- Ioannidis, J.P.A.; Pezzullo, A.M.; Cristiano, A.; Boccia, S. Global Estimates of Lives and Life-Years Saved by COVID-19 Vaccination During 2020-2024. JAMA Heal. Forum 2025, 6, e252223. [Google Scholar] [CrossRef]
- Impact Global Health. Smart Decisions: The G-FINDER 2024 Neglected Disease R&D Report; Sydney, Australia, 2025. [Google Scholar]
- Armenteras, D. Guidelines for healthy global scientific collaborations. Nat. Ecol. Evol. 2021, 5, 1193–1194. [Google Scholar] [CrossRef]
- McCoy, D.; Mwansambo, C.; Costello, A.; Khan, A. Academic partnerships between rich and poor countries. Lancet 2008, 371, 1055–1057. [Google Scholar] [CrossRef]
- Petersen, O.H. Inequality of Research Funding between Different Countries and Regions is a Serious Problem for Global Science. Function 2021, 2, zqab060. [Google Scholar] [CrossRef]
- Stacey, H.J.; De Soir, S.; Jones, J.D. The Safety and Efficacy of Phage Therapy: A Systematic Review of Clinical and Safety Trials. Antibiotics 2022, 11, 1340. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Van Belleghem, J.D.; de Vries, C.R.; Burgener, E.; Chen, Q.; Manasherob, R.; Aronson, J.R.; Amanatullah, D.F.; Tamma, P.D.; Suh, G.A. The Safety and Toxicity of Phage Therapy: A Review of Animal and Clinical Studies. Viruses 2021, 13, 1268. [Google Scholar] [CrossRef] [PubMed]
- Luong, T.; Salabarria, A.-C.; Edwards, R.A.; Roach, D.R. Standardized bacteriophage purification for personalized phage therapy. Nat. Protoc. 2020, 15, 2867–2890. [Google Scholar] [CrossRef] [PubMed]
- Würstle, S.; Lee, A.; Kortright, K.E.; Winzig, F.; An, W.; Stanley, G.L.; Rajagopalan, G.; Harris, Z.; Sun, Y.; Hu, B.; et al. Optimized preparation pipeline for emergency phage therapy against Pseudomonas aeruginosa at Yale University. Sci. Rep. 2024, 14, 1–13. [Google Scholar] [CrossRef]
- Engel, H.W.; Smith, L.; Berwald, L.G. The preservation of mycobacteriophages by means of freeze drying. 1974, 109, 561–6. [Google Scholar] [CrossRef]
- Dessau, M.; Goldhill, D.; McBride, R.L.; Turner, P.E.; Modis, Y. Selective Pressure Causes an RNA Virus to Trade Reproductive Fitness for Increased Structural and Thermal Stability of a Viral Enzyme. PLOS Genet. 2012, 8, e1003102. [Google Scholar] [CrossRef]
- Kering, K.K.; Zhang, X.; Nyaruaba, R.; Yu, J.; Wei, H. Application of Adaptive Evolution to Improve the Stability of Bacteriophages during Storage. Viruses 2020, 12, 423. [Google Scholar] [CrossRef]
- Mitragotri, S. Immunization without needles. Nat. Rev. Immunol. 2005, 5, 905–916. [Google Scholar] [CrossRef]
- Kyung Chang, RY; Morales, S; Okamoto, Y; Chan, H-K. Topical application of bacteriophages for treatment of wound infections. Transl Res. 2020, 220, 153–66. [Google Scholar] [CrossRef]
- Doub, J.B.; Johnson, A.J.; Nandi, S.; Ng, V.; Manson, T.; Lee, M.; Chan, B. Experience Using Adjuvant Bacteriophage Therapy for the Treatment of 10 Recalcitrant Periprosthetic Joint Infections: A Case Series. Clin. Infect. Dis. 2022, 76, e1463–e1466. [Google Scholar] [CrossRef]
- Abedi, AO; Abedi, AA; Ferry, T; Citak, M. Current Applications and the Future of Phage Therapy for Periprosthetic Joint Infections. Antibiotics (Basel) 2025, 14(6), 581. [Google Scholar] [CrossRef]
- Weiner, I.; Kahan-Hanum, M.; Buchstab, N.; Zelcbuch, L.; Navok, S.; Sherman, I.; Nicenboim, J.; Axelrod, T.; Berko-Ashur, D.; Olshina, M.; et al. Phage therapy with nebulized cocktail BX004-A for chronic Pseudomonas aeruginosa infections in cystic fibrosis: a randomized first-in-human trial. Nat. Commun. 2025, 16, 1–15. [Google Scholar] [CrossRef]
- Köhler, T.; Luscher, A.; Falconnet, L.; Resch, G.; McBride, R.; Mai, Q.-A.; Simonin, J.L.; Chanson, M.; Maco, B.; Galiotto, R.; et al. Personalized aerosolised bacteriophage treatment of a chronic lung infection due to multidrug-resistant Pseudomonas aeruginosa. Nat. Commun. 2023, 14, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Dedrick, R.M.; Guerrero-Bustamante, C.A.; Garlena, R.A.; Russell, D.A.; Ford, K.; Harris, K.; Gilmour, K.C.; Soothill, J.; Jacobs-Sera, D.; Schooley, R.T.; et al. Engineered bacteriophages for treatment of a patient with a disseminated drug-resistant Mycobacterium abscessus. Nat. Med. 2019, 25, 730–733. [Google Scholar] [CrossRef] [PubMed]
- Aslam, S.; Courtwright, A.M.; Koval, C.; Lehman, S.M.; Morales, S.; Furr, C.L.; Rosas, F.; Brownstein, M.J.; Fackler, J.R.; Sisson, B.M.; et al. Early clinical experience of bacteriophage therapy in 3 lung transplant recipients. Am. J. Transplant 2019, 19, 2631–2639. [Google Scholar] [CrossRef] [PubMed]
- Dąbrowska, K. Phage therapy: What factors shape phage pharmacokinetics and bioavailability? Systematic and critical review. Med. Res. Rev. 2019, 39, 2000–2025. [Google Scholar] [CrossRef]
- Thompson, D.L.; Semersky, Z.; Feinn, R.; Huang, P.; E Turner, P.; Chan, B.K.; Koff, J.L.; Murray, T.S. Particle size distribution of viable nebulized bacteriophage for the treatment of multi-drug resistant Pseudomonas aeruginosa. Respir. Med. Res. 2024, 86, 101133. [Google Scholar] [CrossRef]
- Speck, P.; Smithyman, A. Safety and efficacy of phage therapy via the intravenous route. FEMS Microbiol. Lett. 2015, 363. [Google Scholar] [CrossRef]
- Kotloff, K.L. The Burden and Etiology of Diarrheal Illness in Developing Countries. Pediatr. Clin. North Am. 2017, 64, 799–814. [Google Scholar] [CrossRef]
- Gutiérrez, B.; Domingo-Calap, P. Phage Therapy in Gastrointestinal Diseases. Microorganisms 2020, 8, 1420. [Google Scholar] [CrossRef]
- Van Gerwen, O.T.; Muzny, C.A.; Marrazzo, J.M. Sexually transmitted infections and female reproductive health. Nat. Microbiol. 2022, 7, 1116–1126. [Google Scholar] [CrossRef]
- Jensen, J.S.; Unemo, M. Antimicrobial treatment and resistance in sexually transmitted bacterial infections. Nat. Rev. Microbiol. 2024, 22, 435–450. [Google Scholar] [CrossRef]
- Cater, K.; Międzybrodzki, R.; Morozova, V.; Letkiewicz, S.; Łusiak-Szelachowska, M.; Rękas, J.; Weber-Dąbrowska, B.; Górski, A. Potential for Phages in the Treatment of Bacterial Sexually Transmitted Infections. Antibiotics 2021, 10, 1030. [Google Scholar] [CrossRef]
- Al Kadri, H.M.; El-Metwally, A.A.; Al Sudairy, A.A.; Al-Dahash, R.A.; Al Khateeb, B.F.; Al Johani, S.M. Antimicrobial resistance among pregnant women with urinary tract infections is on rise: Findings from meta-analysis of observational studies. J. Infect. Public Heal. 2024, 17, 102467. [Google Scholar] [CrossRef]
- Liu, K.A.; Mager, N.A.D. Women’s involvement in clinical trials: historical perspective and future implications. Pharm. Pr. (Internet) 2016, 14, 708–708. [Google Scholar] [CrossRef]
Figure 1.
Overview of the Main Manuscript Themes. The realms of research related to phage therapy development that would contribute to greater equity in how it is used or in who it would benefit, and the advantages of phage therapy in creating greater equity. From left to right, Panel A shows realms of research that could help optimize phage therapy for the most needy in collaboration with ongoing general development (Panel B) of phage therapy. Together, these help recognize the equity-related benefits of phage therapy (Panel C) and promote increased healthcare equity (Panel D).
Figure 1.
Overview of the Main Manuscript Themes. The realms of research related to phage therapy development that would contribute to greater equity in how it is used or in who it would benefit, and the advantages of phage therapy in creating greater equity. From left to right, Panel A shows realms of research that could help optimize phage therapy for the most needy in collaboration with ongoing general development (Panel B) of phage therapy. Together, these help recognize the equity-related benefits of phage therapy (Panel C) and promote increased healthcare equity (Panel D).
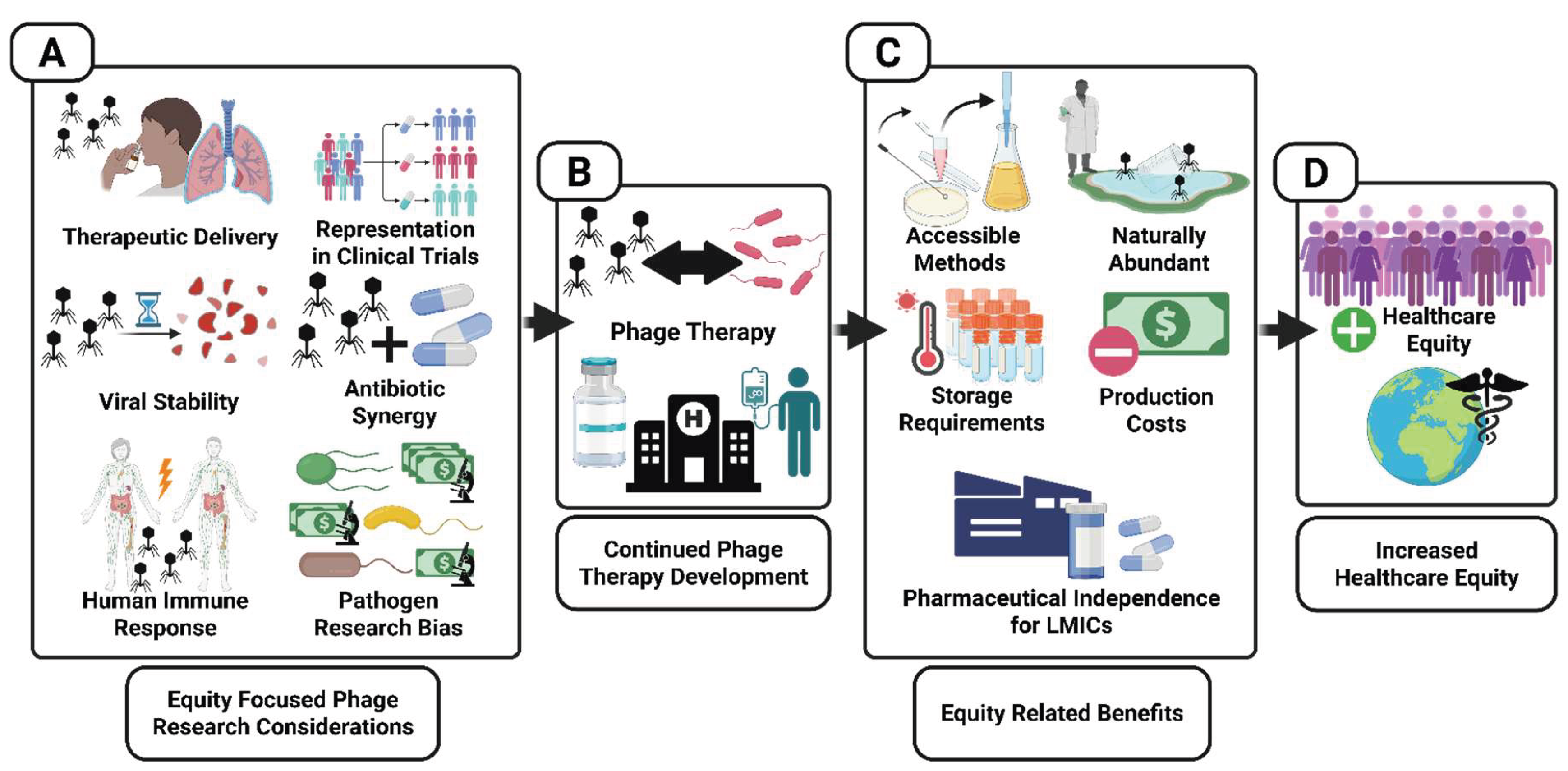
Figure 2.
Summary of Equity Oriented Phage Therapy Research. Overview of research recommendations that will work toward advancing phage therapy and its accessibility to low and middle-income families in High-Income countries (HICs), and for Low and Middle-Income countries in general (LMICs). Some of these recommendations relate to more than one field of research. $ represents “investment of capital”.
Figure 2.
Summary of Equity Oriented Phage Therapy Research. Overview of research recommendations that will work toward advancing phage therapy and its accessibility to low and middle-income families in High-Income countries (HICs), and for Low and Middle-Income countries in general (LMICs). Some of these recommendations relate to more than one field of research. $ represents “investment of capital”.
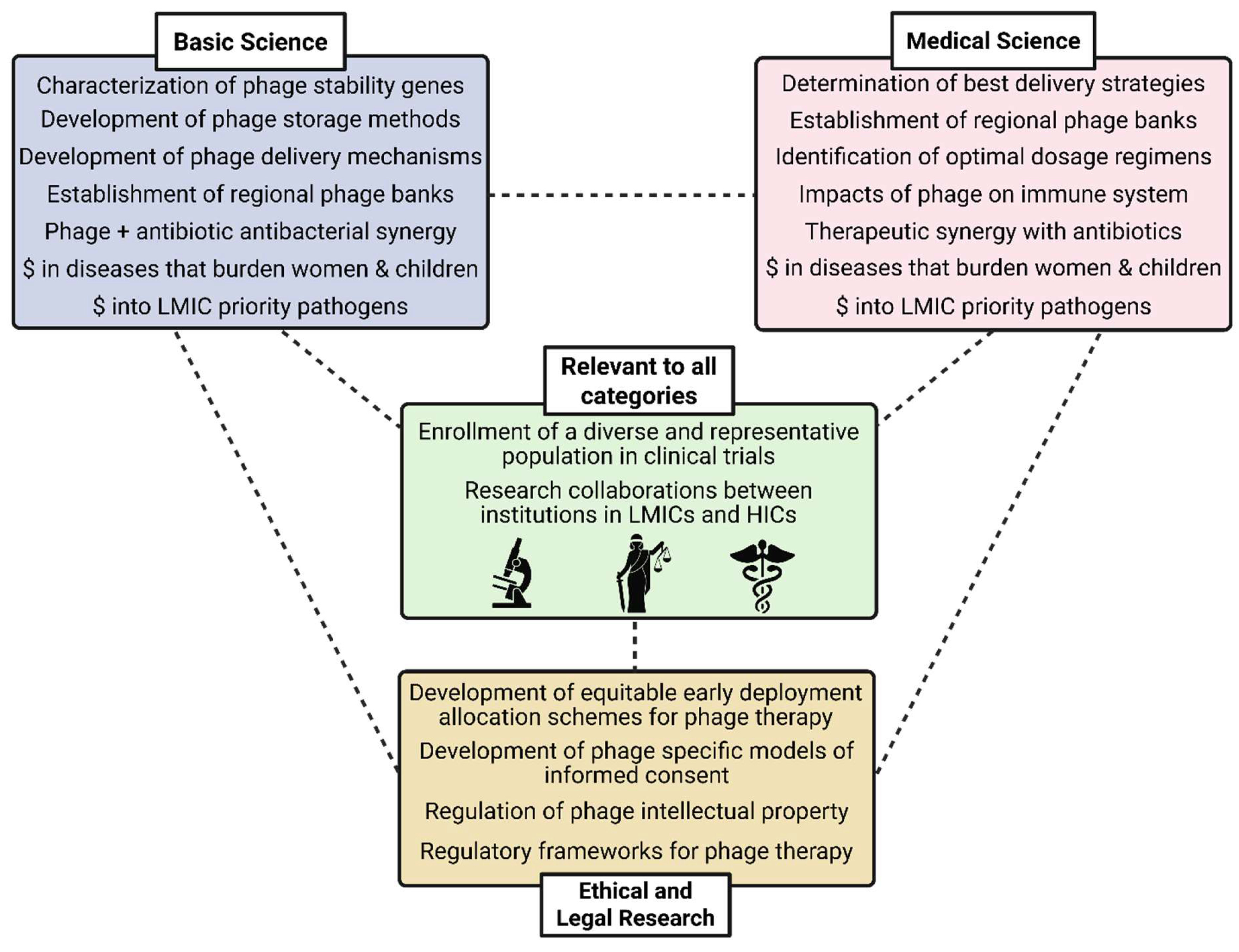
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



