Submitted:
03 October 2025
Posted:
07 October 2025
You are already at the latest version
Abstract
This prospective cohort study examines the association between hyperuricemia (HU) and cardiovascular diseases. We analyzed data from 4,082 participants, dividing them into two groups based on serum uric acid levels. Our findings reveal that participants with elevated serum uric acid or xanthine oxidase inhibitor (XOI) therapy had a significantly higher incidence of cardiovascular events such as coronary artery disease (8.4% vs 3.3%), stroke (2.6% vs. 1.2%), heart failure (3.4% vs. 0.9%), and chronic kidney insufficiency (4.5% vs. 1.9%) compared to those with normal uric acid levels. Moreover, group 2, which had higher serum uric acid levels, also exhibited a higher burden of established cardiovascular risk factors, including hypertension, obesity, and diabetes. These results support the hypothesis that HU is not only a marker for metabolic dysfunction but may also serve as an independent risk factor for cardiovascular morbidity and mortality. We propose that routine measurement of uric acid levels could be a valuable tool for early identification of high-risk cardiovascular patients, particularly in individuals with multiple metabolic risk factors. Further prospective studies are needed to explore the potential benefits of early XOI therapy in reducing cardiovascular events.
Keywords:
hyperuricemia
; coronary artery disease
; hypertension
; atrial fibrillation
; chronic kidney disease
; myocardial infarction
1. Introduction
Cardiovascular diseases are among the leading causes of morbidity and mortality worldwide, playing a central role in both preventive and curative medicine [1,2]. Established risk factors such as arterial hypertension, diabetes mellitus, smoking, and dyslipidemia have been extensively studied and play a key role in patient risk stratification [3,4]. Over the years, HU has gained increasing recognition as a potential risk factor for cardiovascular diseases and continues to receive scientific attention. First described by Garrod in the 19th Century in relation to gout [5]. Since the mid-20th century, evidence has accumulated linking elevated uric acid to hypertension, obesity, and atherosclerosis [6]. In recent decades, the prevalence of HU has steadily increased, presumably related to changes in dietary habits, as well as the rising numbers of overweight individuals and cases of metabolic syndrome [7,8]. Up until the 19th century, the treatment of HU and gout consisted mainly of weight reduction and a low-purine diet. Today, the central component of treatment involves pharmacotherapy with XOIs [9].
HU is classified as either primary or secondary. Secondary HU occurs as a result of underlying diseases associated with increased cell turnover or the use of certain medications. The etiology of primary HU is multifactorial and involves overproduction, increased intake, or reduced renal excretion [10,11].
HU promotes systemic inflammation, which is particularly associated with vascular dysfunctions [12]. It is described in the current literature in connection with metabolic syndrome, obesity, and type II diabetes mellitus and may act as an exacerbator of metabolic dysfunctions [13]. Elevated serum uric acid correlates with increased xanthine oxidase activity, which impairs vasodilation and thus contributes to the development of arterial hypertension [14,15]. Moreover, it promotes the formation of free oxygen radicals, which enhance inflammation in the vascular walls [8]. This results in a higher incidence of macroangiopathies such as coronary artery disease (CAD) and Peripheral artery disease (PAD) [16]. Additionally, it contributes to the development of heart failure and cardiac arrhythmias, such as atrial fibrillation [17,18,19,20].
Since the 1980s, HU > 10 mg/dl, regardless of the presence of gout, has been considered an absolute indication for treatment, based on the assumption that very high serum uric acid levels contribute to the development of cardiovascular events [21]. The effectiveness of treating asymptomatic HU to reduce cardiovascular events remains controversial. Different guidelines vary their recommendations regarding HU. The German Society of Rheumatology suggest treatment when organ manifestations such as arthropathy or nephropathy are present, or in cases of asymptomatic HU with a serum level > 10 mg/dl [9]. The American College of Rheumatology recommends the use of XOIs in close conjunction with cardiovascular comorbidities, being less conservative regarding treatment of asymptomatic HU [22,23]. Since 2011, the Japanese Society for Gout has recommended early treatment, considering HU as a cardiovascular risk factor, even in the asymptomatic stage. Both the KDIGO and the European Society of Cardiology acknowledge HU as a cardiovascular risk factor, but recommend treatment only after confirmed organ manifestation [24]. Recent reviews emphasize the complex and conflicting evidence regarding cardiovascular implications of HU and the safety of urate-lowering therapy [25]. Although HU is associated with the development of established risk factors such as arterial hypertension, the current evidence is insufficient to recommend early treatment [26]. This heterogeneity reflects the still unresolved controversy over whether HU should be treated before organ manifestation, highlighting the need for further prospective population-based studies.
To further investigate the debated question of whether HU can be considered an independent risk factor for cardiovascular diseases or whether it merely exacerbates existing risk factors such as diabetes mellitus, obesity, and hypertension, we conducted an analysis of patients from the prospective ELITE study [27,28]. The study aimed to assess the potential role of uric acid as a risk factor for cardiovascular events such as coronary artery disease, stroke, atrial fibrillation, peripheral arterial disease, and heart failure. Using a large cohort from the Oldenburg Muensterland region, we examined how HU correlates with established risk factors such as hypertension, diabetes, lipid disorders, obesity, and smoking. Additionally, the impact of factors such as gender, age, and comorbidities on these associations was investigated. Furthermore, through a detailed analysis of the dietary habits of the 4,000 participants in the study, the relationship between diet and HU was explored in greater detail. A study in Northwestern Germany examining these variables has not yet been published.
2. Materials and Methods
2.1. Study Design and Population
The data presented are from the ELITE study (DRKS-No.: 00 006 813), a prospective cohort study conducted over 4.4 years. All participants with available baseline serum uric acid measurements, complete baseline data, and follow-up information were included regardless of their underlying comorbidities even if gout was present at baseline. Individuals who did not attend follow-up were excluded. A total of 4082 patients with normal or elevated serum uric acid levels were divided into two groups. Clinical endpoints such as mortality, myocardial infarction, stroke, heart failure, and other cardiovascular events were recorded annually.
2.2. Recruitment
Participants were recruited through newspaper advertisements, invitations to employees of public institutions, and random sampling from population registry data.
2.3. Parameters Controlled
Data were collected on age, sex, health status, pre-existing conditions (e.g., hypertension, diabetes, CAD), medication use, and lifestyle (diet, physical activity). Cognitive functions were assessed using the DemTect test.
2.4. Cardiovascular Risk Factors
- BMI ≥ 30 kg/m2
- LDL > 130 mg/dl
- Smoking
- Diabetes Mellitus: HbA1c > 6.5% or pharmacological treatment
- Blood pressure ≥ 140/90 mmHg
2.5. Physical Activity
- Regular physical activity: ≥ 1x daily or 2–3x per week
- Moderate activity: 1x/week or every 2 weeks
- Rare activity/Inactivity: 1x/month or less
2.6. Cognitive Impairment (DemTect)
- Physiological: > 13 points
- Pathological: 0–12 points
2.7. Laboratory Parameters
Creatinine, eGFR, uric acid, glucose, HbA1c, LDL, HDL, lipoprotein (a), iron, and liver values were recorded. HU was considered diagnosed when the serum uric acid level exceeded the threshold of > 7 mg/dl for men and > 5.7 mg/dl for women. Although current guidelines recommend a single threshold irrespective of sex, large epidemiological studies report higher baseline levels in men, supporting the use of sex-specific cut-offs [29,30].
2.8. Follow Up
Annual follow-up visits and computer-generated individual reports on cardiovascular risk profiles.
2.9. Statistical Analysis
The data were analyzed using SPSS. Chi-square tests were used for categorical variables, and the T-test for metric variables. To account for multiple comparisons in the univariate analyses, Bonferroni correction was applied. Multivariate logistic regressions were employed to evaluate the influence of multiple factors on cardiovascular events. A P-Value <0.05 was considered statistically significant.
3. Results
Table 1 presents the baseline characteristics of the two groups. Of the 4,082 participants, 805 individuals (19.7%) had elevated uric acid levels or were undergoing pharmacological treatment for known HU (Group 2), while 3,277 (80.3%) had normal levels (Group 1; p< 0.001). In Group 2, approximately 15% received XOI therapy. Participants in Group 2 were more likely to be male (61% vs. 48.5%) and, on average, older (58 vs. 52 years; p< 0.001).
In Group 1, 1.64% of patients reported a stroke, 2.9% had CAD, 1.15% had a myocardial infarction, 1.7% had heart failure, 2.8% had atrial fibrillation, 4.9% had type 1 or type 2 diabetes, 56.4% had arterial hypertension, 4.7% had PAD and 1.92% had chronic kidney disease (CKD). In Group 2, the values for these pre-existing conditions were consistently higher: 3.4% for stroke, 9.3% for CAD, 4.9% for myocardial infarction, 4.4% for heart failure, 6.8% for atrial fibrillation, 12.8% for diabetes mellitus, 82.7% for arterial hypertension, 7.3% for PAD, and 14.1% for CKD, with differences being statistically significant in all cases.
The second section of Table 1 presents the risk profiles of Group 1 and Group 2. In summary, significant differences were observed between the two groups in several relevant clinical parameters, particularly in terms of BMI, arterial hypertension, HbA1c, diabetes status, and lipid profiles, with Group 2 showing a more burdened cardiovascular risk profile. Only smoking showed no significant difference between the groups.
A significant difference was observed in the number of cardiovascular risk factors per participant between Group 1 and Group 2. In Group 1, 20.7% of participants had no risk factors, while 34.9% had one, 27.6% had two, 10.8% had three, and 1.5% had four risk factors. In contrast, in Group 2, only 4.3% had no risk factors, 21.5% had one, 38% had two, 25% had three, and 5.2% had four risk factors (Figure 1).
In Group 1, 43.1% of participants reported engaging in regular vigorous physical activity. A moderate level of physical activity was reported by 28.6%, while 28.3% engaged in little to no physical activity (p<0.001). In Group 2, 33.5% reported engaging in regular vigorous physical activity, 29.8% participated in moderate physical activity, and 36.7% had little to no physical activity in their daily routine (p< 0.001) (Section 4 of Table 1).
A low level of fruit intake was noted in 15.3% of individuals in Group 1 and in 17.3% of those in Group 2. The proportion of participants with moderate fruit intake was nearly identical between groups (24.7% in Group 1 vs. 25% in Group 2). The majority in both groups reported a high consumption of fruit, accounting for 58.7% in Group 1 and 56.1% in Group 2. Low meat intake was reported by 20.9% of Group 1 and 16% of Group 2. Most participants consumed a moderate amount of meat, with 65% in Group 1 and 61.3% in Group 2. A higher intake of meat was slightly more prevalent in Group 2 (22.7%) than in Group 1 (13.3%) (Section 5 of Table 1).
At the beginning of the study, Group 1 scored an average of 16.3 points (SD 2.2) on the DemTect, which increased to 16.6 points (SD 2.2) by the end of the study. Group 2 started with 15.5 points (SD 2.8) and reached 16.4 points (SD 2.2) at the study’s conclusion (Section 6 of Table 1).
During the study period, the overall mortality rate was 2% in Group 1 and 8% in Group 2 (p<0.001). Cardiovascular events occurred in 11% of participants in Group 1 and 22% in Group 2 (p<0.001). Participants with HU had a significantly higher incidence for cardiovascular endpoints. The excess risk was most pronounced for CAD (8.4% vs. 3.3%), stroke (2.6% vs. 1.2%), CKD (5.5% vs. 1.9%) and myocardial infarction (3.1% vs. 1.3%). Please see Table 2.
In a multivariate analysis, the impact of age, diabetes mellitus, and HU on the clinical endpoints was evaluated. Age emerged as a significant predictor in all models (p < 0.001). Diabetes showed significant associations with CAD, stroke, CKD, myocardial infarction and heart failure. HU was significantly associated with the same endpoints except heart failure (Table 3).
4. Discussion
The results of this prospective cohort study correlate with a significantly higher prevalence and incidence of cardiovascular diseases and associated risk factors in individuals with elevated serum uric acid levels or those already undergoing XOI therapy. To date, no observational study in Northwestern Germany has been conducted with these results.
Participants with HU experienced significantly higher rates of CAD (8,4% vs. 3,3%), stroke (2,6% vs. 1,2%), heart failure (3,4% vs. 0,9%), atrial fibrillation (4,9% vs. 2%) and CKD (5.5% vs. 1.9%). HU showed a significant predictive value for CKD, stroke, CAD and myocardial Infarction. The overall mortality was also significantly higher in this group (8% vs. 2%). These findings support the hypothesis that HU may be a marker and predictor for cardiovascular morbidity and mortality.
Our findings are consistent with previous epidemiological studies, such as the Framingham Heart Study, which described the associations between elevated uric acid levels and the occurrence of cardiovascular events as early as the 19th century [6]. Current meta-analyses, such as those by Zheng et al. and Zao et al., confirm these findings based on large cohorts [31,32]. In our cohort, Group 2 showed, in addition to elevated uric acid levels, a significantly higher prevalence of established risk factors, such as arterial hypertension (82.7% vs. 56.4%), obesity (mean BMI 29.8 vs. 26.1 kg/m2), diabetes mellitus (12.8% vs. 4.9%), dyslipidemia (48,1% vs. 54,2%), and impaired kidney function (eGFR 82 vs. 102 ml/min). These comorbidities are well-established components of the metabolic syndrome and are associated with the presence of HU [33,34]. Our observations reflect the pathophysiological vicious circle in which HU plays a significant role in the development and potentiation of metabolic syndrome [33,35,36]. HU exacerbates the progression of impaired kidney function, leading to the retention of uric acid and the accumulation of systemic inflammation and vascular damage, thereby closing the vicious cycle [37,38,39]. Evidence for this is the already reduced eGFR in Group 2 (82 ml/min vs. 102 ml/min) with a significantly higher incidence of CKD in Group 2 (5.6% vs. 1.6%). Although a direct causal relationship cannot be established in this observational cohort, our multivariable regression analysis indicates that HU remained independently associated to CKD after adjustment for major risk factors. This suggests that HU may contribute to renal impairment beyond traditional metabolic comorbidities.
Lifestyle factors such as meat or dietary habits and physical activity presented significant differences in our cohort. Group 2 showed a lower level of physical activity, which is a well-known risk factor for cardiovascular diseases [40]. Regular moderate to intensive physical activity improves insulin resistance and renal uric acid excretion [41,42,43]. Participants in Group 2 demonstrated a significantly different pattern of meat consumption compared to Group 1. This observation aligns with current evidence indicating that high meat intake, due to its elevated purine content, contributes to increased uric acid production and sustained elevation of serum uric acid levels [44,45]. Participants in Group 1 reported a significantly higher fruit consumption compared to those in Group 2. Although fructose-rich diet can acutely increase uric acid levels, the observed inverse association in our cohort appears to be a marker for balanced nutrition and healthier lifestyle [46,47].
The relationship between HU and cognitive function remains controversial: while some studies suggest neuroprotective effects, other link HU to increased dementia risk due to vascular damage. In our cohort cognitive performance improved in both groups [48,49,50,51]. These changes are more likely attributable to an overall improvement of cardiovascular risk profile rather than a direct effect of serum uric acid [52].
The strengths of the study include the large sample size, detailed collection of laboratory and lifestyle data, and the prospective study design.
Potential limitations include the interventionist approach as it is possible that endpoint biases were introduced due to improvements in cardiovascular risk profiles of both groups, but especially Group 2. Second, as an observational study, causal relationships cannot be inferred Third dietary and physical activity data were self-reported and therefore subject to recall bias. Over- or underestimation of these behaviors cannot be ruled out. Additional baseline imbalances between the two groups may have biased follow-up risk estimates. For example, participants with HU had higher prevalence prior stroke, which increases risk for subsequent events.
In summary, our results show a significant association between HU and cardiovascular complications. The observed relationships cannot be interpreted independently of accompanying risk factors, meaning that a definitive causal relationship cannot be established. Given the observed clustering of metabolic dysfunctions, including glucose intolerance, obesity, hypertension, and dyslipidemia, in combination with existing HU, the routine measurement of elevated uric acid levels in clinical practice could represent a valuable tool for the early identification of high-risk cardiovascular patients. Particularly in patients with multiple metabolic risk factors, HU should be considered as a potential exacerbator of overall risk. Whether serum uric acid reduction through early use of XOIs leads to a reduction in cardiovascular events remains unclear and requires further studies. A renewed prospective interventional study over an extended period would be advisable. While current guidelines recommend therapy only for symptomatic HU or organ manifestation, our results support a more individualized approach to cardiovascular risk profiles, particularly in high-risk populations, with potential early use of XOIs even before organ manifestation.
Author Contributions
Conceptualization, F.A. and B.S.; methodology, J.S.; software, B.V.; validation, F.A., B.S., S.L., J.S. and A.E.; formal analysis, S.L.; investigation, F.A.; resources, F.A.; data curation, F.A. and B.V.; writing—original draft preparation, F.A.; writing—review and editing, F.A.; visualization, F.A.; supervision, S.L. and J.S.; project administration, J.S. All authors have read and agreed to the published version of the manuscript.”
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Ethics Committee of the University Goettingen (protocol code DRKS-No.: 00 006 813 approved 18.09.2014).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study
Data Availability Statement
Additional and raw data can be obtained from the corresponding author under fady.al-azem@uni-oldenburg.de
Conflicts of Interest
The authors declare no conflicts of interest
Abbreviations
The following abbreviations are used in this manuscript:
| AF | Atrial Fibrillation |
| BMI | Body mass index |
| CAD | Coronary artery disease |
| CKD | Chronic kidney disease |
| CVRF | Cardiovascular risk factors |
| eGFR | Estimated glomerular filtration rate |
| HbA1c | Glycated hemoglobin |
| HDL | High-density lipoprotein |
| HF | Heart failure |
| HU | Hyperuricemia |
| KDIGO | Kidney Disease: Improving Global Outcomes |
| LDL | Low-density lipoprotein |
| Lp(a) | Lipoprotein (a) |
| MI | Myocardial Infarction |
| PAD | Peripheral artery disease |
| SD | Standard deviation |
| SPSS | Statistical Package for the Social Sciences |
| XOI | Xanthine oxidase inhibitor |
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J Am Coll Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef]
- Tan, S.C.W.; Zheng, B.-B.; Tang, M.-L.; Chu, H.; Zhao, Y.-T.; Weng, C. Global Burden of Cardiovascular Diseases and its Risk Factors, 1990–2021: A Systematic Analysis for the Global Burden of Disease Study 2021. QJM. 2025, 118, 411–422. [Google Scholar] [CrossRef] [PubMed]
- Boehme, A.K.; Esenwa, C.; Elkind, M.S. Stroke Risk Factors, Genetics, and Prevention. Circ Res. 2017, 120, 472–495. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.J.; Xavier, D.; Liu, L.; Zhang, H.; Chin, S.L.; Rao-Melacini, P.; et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): A case-control study. Lancet 2010, 376, 112–123. [Google Scholar] [CrossRef] [PubMed]
- Garrod, A.B. A Treatise on gout and rheumatic gout (rheumatoid arthritis): Longmans, Green; 1876.
- Brand, F.N.; McGee, D.L.; Kannel, W.B.; Stokes, J.; 3rd Castelli, W.P. Hyperuricemia as a risk factor of coronary heart disease: The Framingham Study. Am J Epidemiol. 1985, 121, 11–18. [Google Scholar] [CrossRef]
- Shan, R.; Ning, Y.; Ma, Y.; Gao, X.; Zhou, Z.; Jin, C.; et al. Incidence and Risk Factors of Hyperuricemia among 2.5 Million Chinese Adults during the Years 2017-2018. Int J Environ Res Public Health. 2021, 18, 2579. [Google Scholar] [CrossRef]
- Zhang, S.; Wang, Y.; Cheng, J.; Huangfu, N.; Zhao, R.; Xu, Z.; et al. Hyperuricemia and Cardiovascular Disease. Curr Pharm Des. 2019, 25, 700–709. [Google Scholar] [CrossRef]
- Deutsche Gesellschaft für Rheumatologie. Leitlinie: Diagnostik und Therapie der Gicht. 2024. https://register.awmf.org/de/leitlinien/detail/060-005.
- Matsuo, H.; Nakayama, A.; Sakiyama, M.; Chiba, T.; Shimizu, S.; Kawamura, Y.; et al. ABCG2 dysfunction causes hyperuricemia due to both renal urate underexcretion and renal urate overload. Sci Rep. 2014, 4, 3755. [Google Scholar] [CrossRef]
- Waheed, Y.; Yang, F.; Sun, D. Role of asymptomatic hyperuricemia in the progression of chronic kidney disease and cardiovascular disease. Korean J Intern Med. 2021, 36, 1281–1293. [Google Scholar] [CrossRef]
- Yanai, H.; Adachi, H.; Hakoshima, M.; Katsuyama, H. Molecular Biological and Clinical Understanding of the Pathophysiology and Treatments of Hyperuricemia and Its Association with Metabolic Syndrome, Cardiovascular Diseases and Chronic Kidney Disease. Int J Mol Sci. 2021, 22, 9480. [Google Scholar] [CrossRef]
- He, Y.; Chen, D.; Xu, J.-P.; Jin, J.; Wang, J.; Geng, C.; et al. Association between Serum Uric Acid and Hypertension in a Large Cross-Section Study in a Chinese Population. Journal of Cardiovascular Development and Disease [Internet] 2022, 9, 287. [Google Scholar] [CrossRef] [PubMed]
- Landmesser, U.; Spiekermann, S.; Dikalov, S.; Tatge, H.; Wilke, R.; Kohler, C.; et al. Vascular oxidative stress and endothelial dysfunction in patients with chronic heart failure: Role of xanthine-oxidase and extracellular superoxide dismutase. Circulation 2002, 106, 3073–3078. [Google Scholar] [CrossRef] [PubMed]
- Packer, M. Uric Acid Is a Biomarker of Oxidative Stress in the Failing Heart: Lessons Learned from Trials With Allopurinol and SGLT2 Inhibitors. J Card Fail. 2020, 26, 977–984. [Google Scholar] [CrossRef]
- Kleber, M.E.; Delgado, G.; Grammer, T.B.; Silbernagel, G.; Huang, J.; Krämer, B.K.; et al. Uric Acid and Cardiovascular Events: A Mendelian Randomization Study. J Am Soc Nephrol. 2015, 26, 2831–2838. [Google Scholar] [CrossRef]
- Bos, M.J.; Koudstaal, P.J.; Hofman, A.; Witteman, J.C.; Breteler, M.M. Uric acid is a risk factor for myocardial infarction and stroke: The Rotterdam study. Stroke. 2006, 37, 1503–1507. [Google Scholar] [CrossRef]
- Ekundayo, O.J.; Dell’Italia, L.J.; Sanders, P.W.; Arnett, D.; Aban, I.; Love, T.E.; et al. Association between hyperuricemia and incident heart failure among older adults: A propensity-matched study. Int J Cardiol. 2010, 142, 279–287. [Google Scholar] [CrossRef]
- Kim, S.Y.; Guevara, J.P.; Kim, K.M.; Choi, H.K.; Heitjan, D.F.; Albert, D.A. Hyperuricemia and risk of stroke: A systematic review and meta-analysis. Arthritis Rheum. 2009, 61, 885–892. [Google Scholar] [CrossRef]
- Nyrnes, A.; Toft, I.; Njølstad, I.; Mathiesen, E.B.; Wilsgaard, T.; Hansen, J.B.; et al. Uric acid is associated with future atrial fibrillation: An 11-year follow-up of 6308 men and women--the Tromso Study. Europace. 2014, 16, 320–326. [Google Scholar] [CrossRef]
- Sato, Y.; Feig, D.I.; Stack, A.G.; Kang, D.H.; Lanaspa, M.A.; Ejaz, A.A.; et al. The case for uric acid-lowering treatment in patients with hyperuricaemia and CKD. Nat Rev Nephrol. 2019, 15, 767–775. [Google Scholar] [CrossRef]
- Gupta, M.K.; Singh, J.A. Cardiovascular Disease in Gout and the Protective Effect of Treatments Including Urate-Lowering Therapy. Drugs. 2019, 79, 531–541. [Google Scholar] [CrossRef]
- FitzGerald, J.D.; Dalbeth, N.; Mikuls, T.; Brignardello-Petersen, R.; Guyatt, G.; Abeles, A.M.; et al. 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Care Res (Hoboken). 2020, 72, 744–760. [Google Scholar] [CrossRef]
- Holubarsch, C. Deutsche Gesellschaft für Kardiologie: Harnsäuresenkung zur kardiovaskulären Risikoreduktion? 2016. https://dgk.org/pressemitteilungen/2016-ht-pm/2016-ht-statements/2016-ht-statements-tag2/harnsaeuresenkung-zur-kardiovaskulaeren-risikoreduktion/.
- Shubietah, A.; Awashra, A.; Milhem, F.; Ghannam, M.; Hattab, M.; Rajab, I.; et al. Hyperuricemia and Cardiovascular Risk: Insights and Implications. Crit Pathw Cardiol. 2025, 24, e0388. [Google Scholar] [CrossRef]
- Zhiwei, W.; Guiping, Y.; Bing, Y.; Chenghao, Z. The relationship between hyperuricemia and hypertension: A short review of current evidence. Metabolism and Target Organ Damage. 2024, 4, 3. [Google Scholar]
- Lüders, S.; Schrader, B.; Bäsecke, J.; Haller, H.; Elsässer, A.; Koziolek, M.; et al. ELITE study - Nutrition, lifestyle and individual information for the prevention of stroke, dementia and heart attack - Study design and cardiovascular status. Dtsch Med Wochenschr. 2019, 144, e42–e50. [Google Scholar]
- Schrader, B.; Schrader, J.; Koziolek, M.; Elsässer, A.; Bünker, A.M.; Hillmann, B.; et al. Influence of individualized prevention recommendations after one year on the control of hypertension in 3,868 follow-up participants of the ELITE study. Cent Eur J Public Health. 2021, 29, 305–310. [Google Scholar] [CrossRef]
- Zitt, E.; Fischer, A.; Lhotta, K.; Concin, H.; Nagel, G. Sex- and age-specific variations, temporal trends and metabolic determinants of serum uric acid concentrations in a large population-based Austrian cohort. Sci Rep. 2020, 10, 7578. [Google Scholar] [CrossRef]
- Liu, D.; Zheng, X.; Zhu, J.; Yang, J.; Lu, L.; Ji, X.; et al. Gender-specific association between serum uric acid levels and hypertension in East China: A cross-sectional study. BMC Public Health. 2025, 25, 944. [Google Scholar] [CrossRef] [PubMed]
- Zheng, L.; Zhu, Y.; Ma, Y.; Zhang, H.; Zhao, H.; Zhang, Y.; et al. Relationship between hyperuricemia and the risk of cardiovascular events and chronic kidney disease in both the general population and hypertensive patients: A systematic review and meta-analysis. Int J Cardiol. 2024, 399, 131779. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Cao, L.; Zhao, T.Y.; Yang, X.; Zhu, X.X.; Zou, H.J.; et al. Cardiovascular events in hyperuricemia population and a cardiovascular benefit-risk assessment of urate-lowering therapies: A systematic review and meta-analysis. Chin Med J (Engl). 2020, 133, 982–993. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.K.; Ford, E.S. Prevalence of the metabolic syndrome in individuals with hyperuricemia. Am J Med. 2007, 120, 442–447. [Google Scholar] [CrossRef]
- Yuan, H.; Yu, C.; Li, X.; Sun, L.; Zhu, X.; Zhao, C.; et al. Serum Uric Acid Levels and Risk of Metabolic Syndrome: A Dose-Response Meta-Analysis of Prospective Studies. J Clin Endocrinol Metab. 2015, 100, 4198–4207. [Google Scholar] [CrossRef]
- Jiang, J.; Zhang, T.; Liu, Y.; Chang, Q.; Zhao, Y.; Guo, C.; et al. Prevalence of Diabetes in Patients with Hyperuricemia and Gout: A Systematic Review and Meta-analysis. Curr Diab Rep. 2023, 23, 103–117. [Google Scholar] [CrossRef] [PubMed]
- Sowers, J.R.; Whaley-Connell, A.; Hayden, M.R. The Role of Overweight and Obesity in the Cardiorenal Syndrome. Cardiorenal Medicine. 2011, 1, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Jin, M.; Yang, F.; Yang, I.; Yin, Y.; Luo, J.J.; Wang, H.; et al. Uric acid, hyperuricemia and vascular diseases. FBL. 2012, 17, 656–669. [Google Scholar] [CrossRef] [PubMed]
- Loeffler, L.F.; Navas-Acien, A.; Brady, T.M.; Miller, E.R.; 3rd Fadrowski, J.J. Uric acid level and elevated blood pressure in US adolescents: National Health and Nutrition Examination Survey, 1999-2006. Hypertension. 2012, 59, 811–817. [Google Scholar] [CrossRef]
- Suliman, M.E.; Johnson, R.J.; García-López, E.; Qureshi, A.R.; Molinaei, H.; Carrero, J.J.; et al. J-shaped mortality relationship for uric acid in CKD. Am J Kidney Dis. 2006, 48, 761–771. [Google Scholar] [CrossRef]
- Regionalkomitee für Europa, T. Fünfundsechzigste Tagung des Regionalkomitees für Europa: Vilnius, 14.–17. September 2015: Strategie der Europäischen Region der WHO zur Bewegungsförderung (2016–2025). Vilnius: Weltgesundheitsorganisation. Regionalbüro für Europa; 2015.
- Zhang, W.Z.; Peng, Q.; Cai, X.S.; Jiang, G.L.; Huang, J.J.; Lu, L.L.; et al. A study on the correlation between hyperuricemia and lifestyle and dietary habits. Medicine 2025, 104, e41399. [Google Scholar] [CrossRef]
- Chen, J.H.; Wen, C.P.; Wu, S.B.; Lan, J.L.; Tsai, M.K.; Tai, Y.P.; et al. Attenuating the mortality risk of high serum uric acid: The role of physical activity underused. Ann Rheum Dis. 2015, 74, 2034–2042. [Google Scholar] [CrossRef]
- Lobelo, F.; Rohm Young, D.; Sallis, R.; Garber, M.D.; Billinger, S.A.; Duperly, J.; et al. Routine Assessment and Promotion of Physical Activity in Healthcare Settings: A Scientific Statement From the American Heart Association. Circulation 2018, 137, e495–e522. [Google Scholar] [CrossRef]
- Chi, X.; Cen, Y.; Yang, B.; Zhang, H.; Pu, Z.; Feng, J.; et al. Effects of dietary factors on hyperuricaemia and gout: A systematic review and meta-analysis of observational studies. Int J Food Sci Nutr. 2024, 75, 753–773. [Google Scholar] [CrossRef]
- Hong, F.; Zheng, A.; Xu, P.; Wang, J.; Xue, T.; Dai, S.; et al. High-Protein Diet Induces Hyperuricemia in a New Animal Model for Studying Human Gout. Int J Mol Sci. 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, Y.; Mazuka, M.; Yasuda, A.; Sato, M.; Hosaka, T.; Arai, H. Acute effect of fructose, sucrose, and isomaltulose on uric acid metabolism in healthy participants. J Clin Biochem Nutr. 2023, 72, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Olofsson, C.; Anderstam, B.; Bragfors-Helin, A.C.; Eriksson, M.; Qureshi, A.R.; Lindholm, B.; et al. Effects of acute fructose loading on levels of serum uric acid-a pilot study. Eur J Clin Invest. 2019, 49, e13040. [Google Scholar] [CrossRef] [PubMed]
- Tana, C.; Ticinesi, A.; Prati, B.; Nouvenne, A.; Meschi, T. Uric Acid and Cognitive Function in Older Individuals. 2018, 10.
- Yao, Y.; Zhu, S.; Ni, J.; Wei, M.; Li, T.; Long, S.; et al. Gout or Hyperuricemia and Dementia Risk: A Meta-Analysis of Observational Studies. J Alzheimers Dis. 2024, 101, 417–427. [Google Scholar] [CrossRef]
- Latourte, A.; Soumaré, A.; Bardin, T.; Perez-Ruiz, F.; Debette, S.; Richette, P. Uric acid and incident dementia over 12 years of follow-up: A population-based cohort study. Ann Rheum Dis. 2018, 77, 328–335. [Google Scholar] [CrossRef]
- Krittanawong, C.; Maitra, N.S.; Qadeer, Y.K.; Wang, Z.; Fogg, S.; Storch, E.A.; et al. Association of Depression and Cardiovascular Disease. Am J Med. 2023, 136, 881–895. [Google Scholar] [CrossRef]
- Latourte, A.; Bardin, T.; Richette, P. Uric acid and cognitive decline: A double-edge sword? Curr Opin Rheumatol. 2018, 30, 183–187. [Google Scholar] [CrossRef]
Figure 1.
Number of Cardiovascular Risk Factors (CVRF).
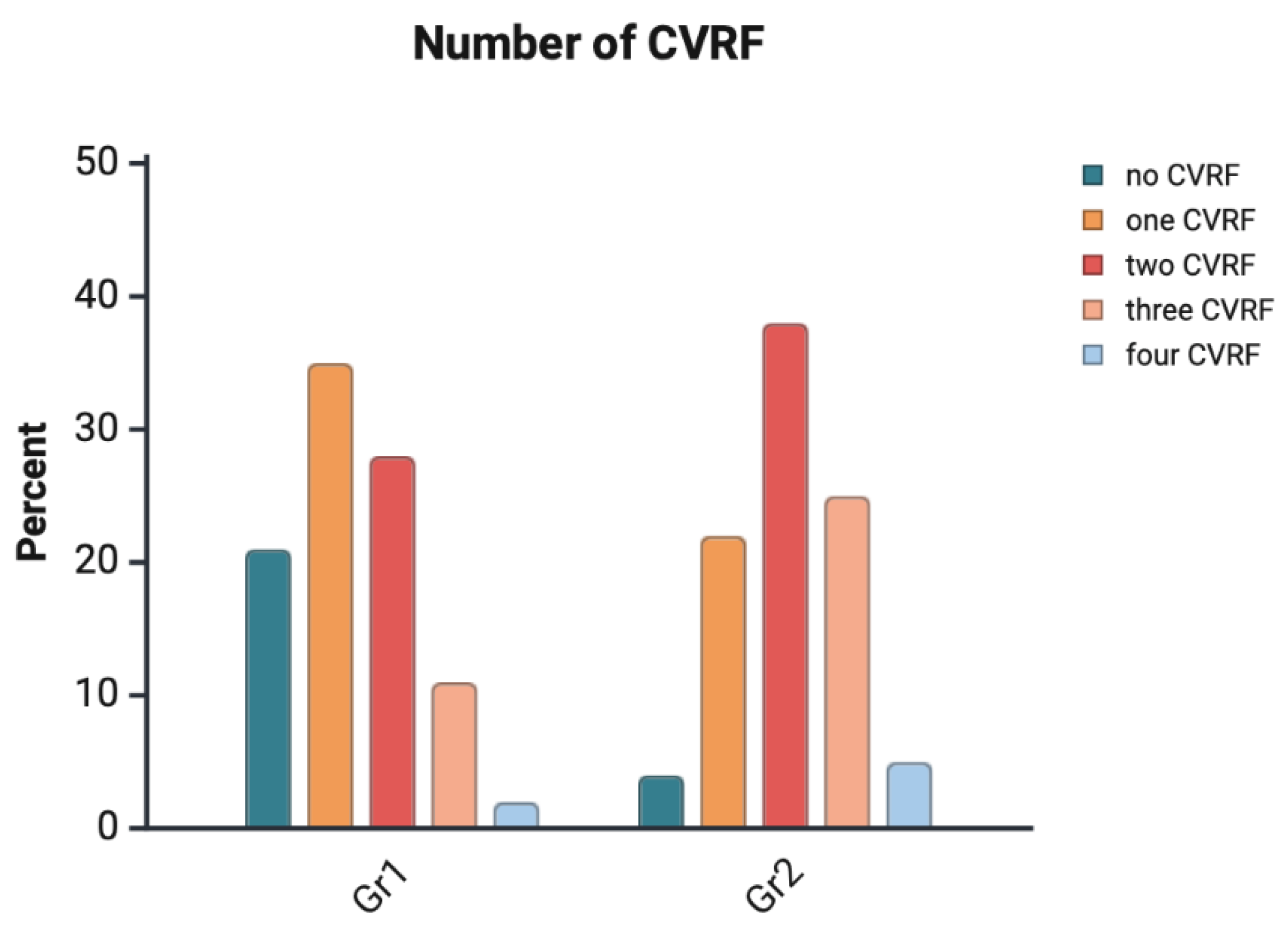

Table 1.
Baseline characteristics.
| Group 1 | Group 2 | P-Value | |
| Participants n (%) | 3288 (80.3) | 805 (19.7) | <0.001 |
| Age mean (SD) in years | 51.8 (13.6) | 58.0 (14.1) | <0.001 |
| Male, n (%) | 1589 (48.5) | 490 (60.9) | <0.001 |
| Female, n (%) | 1688 (51.5) | 315 (39.1) | <0.001 |
| Serum uric acid, mean (SD) in mg/dL | 4.8 (1.03) | 7.1 (1.13) | <0.001 |
| Serum uric acid level > 6,5 mg/dL, n (%) | 743 (92.2) | <0.001 | |
| Serum uric acid > 10 mg/dL, n (%) | 13 (1.6) | <0.001 | |
| Diabetes mellitus, n (%) | 146 (4.9) | 103 (12.8) | <0.001 |
| Arterial Hypertension, n (%) | 1847 (56.4) | 666 (82.7) | <0.001 |
| BMI > 30 kg/m2 n (%) | 553 (16.9) | 350 (42.5) | <0.001 |
| Tobacco use, n (%) | 467 (14.3) | 91 (11.3) | 0.116 |
| HbA1C %, mean (SD) in % | 5.2 (0.56) | 5.6 (0.65) | <0.001 |
| LDL, mean (SD) in mg/dL | 128.9 (35.4) | 136.9 (34.9) | <0.001 |
| HDL, mean (SD) in mg/dL | 63 (18.7) | 52.6 (15.6) | <0.001 |
| Lp(a), mean (SD) in nmol/L | 42.1 (20.3) | 43.4 (16.4) | <0.001 |
| eGFR, mean (SD) in ml/min | 102.7 (24.5) | 82.1 (26.4) | <0.001 |
| Stroke, n (%) | 54 (1.64) | 28 (3.4) | 0.002 |
| CAD, n (%) | 96 (2.9) | 75 (9.3) | <0.001 |
| MI, n (%) | 38 (1.15) | 40 (4.9) | <0.001 |
| HF, n (%) | 56 (1.7) | 36 (4.4) | <0.001 |
| AF, n (%) | 94 (2.8) | 55 (6.8) | <0.001 |
| PAD, n (%) | 154 (4.7) | 59 (7.3) | 0.003 |
| CKD, n (%) | 63 (1.92) | 114 (14.1) | <0.001 |
| Regular physical activity, n (%) | 1630 (43.1) | 275 (33.5) | <0.001 |
| Moderate physical activity, n (%) | 1081 (28.6) | 244 (29.6) | <0.001 |
| Sparse physical activity, n (%) | 1071 (28.3) | 301 (36.7) | <0.001 |
| High fruit intake, n (%) | 2221 (58.7) | 460 (56.1) | <0.001 |
| Moderate fruit intake, n (%) | 934 (24.7) | 205 (25.0) | 0.104 |
| Low fruit intake, n (%) | 579 (15.3) | 142 (17.3) | 0.27 |
| High meat intake, n (%) | 900 (13.3) | 186 (22.7) | 0.016 |
| Moderate meat intake, n (%) | 2159 (65.0) | 494 (61.3) | 0.024 |
| Low meat intake, n (%) | 686 (20.9) | 129 (16.0) | 0.002 |
| DemTect baseline, mean (SD) in points | 16.3 (2.2) | 15.5 (2.8) | |
| DemTect follow up, mean (SD) in points | 16.6 (2.2) | 16.4 (2.2) | |
* CAD; coronary artery disease, CKD; chronic kidney disease, PAD; peripheral artery disease, AF; atrial fibrillation, HF; heart failure, MI; myocardial infarction, BMI; body mass index, HbA1c; glycated hemoglobin, LDL; low-density lipoprotein cholesterol, HDL; high-density lipoprotein, Lp(a); lipoprotein(a), eGFR; estimated glomerular filtration rate.
Table 2.
Endpoints.
| Group 1 | Group 2 | P-Value | |
| CAD, n (%) | 108 (3.3) | 67 (8.4) | <0.001 |
| HF, n (%) | 31 (0.9) | 27 (3.4) | <0.001 |
| Stroke, n (%) | 40 (1.2) | 21 (2.6) | <0.001 |
| MI, n (%) | 44 (1.3) | 25 (3.1) | <0.001 |
| PAD, n (%) | 77 (2.4) | 36 (4.5) | <0.001 |
| AF, n (%) | 67 (2.0) | 39 (4.9) | <0.001 |
| CKD, n (%) | 62 (1.9) | 44 (5.5) | <0.001 |
* CAD; coronary artery disease, CKD; chronic kidney disease, PAD; peripheral artery disease, AF; atrial fibrillation, HF; heart failure, MI; myocardial infarction.
Table 3.
Multivariate logistic regression analysis: significance levels (p-values) of age, diabetes mellitus, and hyperuricemia as predictors.
Table 3.
Multivariate logistic regression analysis: significance levels (p-values) of age, diabetes mellitus, and hyperuricemia as predictors.
| Age | Diabetes Mellitus | Hyperuricemia | |
|---|---|---|---|
| CAD, P-Value | <0.001 | <0.001 | <0.001 |
| HF, P-Value | <0.001 | 0.018 | 0.092 |
| Stroke, P-Value | <0.001 | <0.001 | 0.049 |
| PAD, P-Value | <0.001 | 0.526 | 0.115 |
| AF, P-Value | <0.001 | 0.414 | 0.441 |
| CKD, P-Value | <0.001 | 0.015 | 0.022 |
| MI, P-Value | <0.001 | 0.011 | 0.003 |
* CAD; coronary artery disease, CKD; chronic kidney disease, PAD; peripheral artery disease, AF; atrial fibrillation, HF; heart failure, MI; myocardial infarction.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



