
Submitted:
18 September 2025
Posted:
19 September 2025
You are already at the latest version
Abstract
The incidence of acute myocardial infarction (AMI) in young adults has been steadily rising, emphasizing the need for new biomarkers to improve risk stratification. Lipo-protein(a) (Lp(a)), a genetically determined lipoprotein with pro-atherogenic and pro-thrombotic properties, has gained increasing attention in this context. Our findings show that elevated Lp(a) levels are significantly more common in young patients with AMI compared with healthy controls. Importantly, Lp(a) ≥30 mg/dL was strongly associated with multivessel coronary artery disease in NSTEMI, conferring more than a fourfold increased risk. In STEMI, its effect was weaker and largely influenced by concomitant factors such as diabetes and elevated LDL cholesterol. These results underline key pathophysiological differences between infarct phe-notypes and position Lp(a) as a particularly relevant biomarker in young NSTEMI pa-tients. Systematic assessment of Lp(a) may enhance coronary risk stratification and support more tailored secondary prevention strategies.
Keywords:
lipoprotein(a)
; myocardical infarction
; young people
1. Introduction
Over the past decade, the incidence of acute myocardial infarction in young patients has shown a steady increase, becoming a significant public health issue with major clinical and socio-economic implications. This trend underscores the urgent need for additional biomarkers capable of providing more accurate risk stratification and supporting individualized secondary prevention strategies. Among such biomarkers, lipoprotein(a) [Lp(a)] has attracted particular interest due to its pro-atherogenic and pro-thrombotic properties, as well as its consistent association with premature cardiovascular events.[1]
Although myocardial infarction is defined by a common ischemic mechanism, its clinical subtypes—ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation myocardial infarction (NSTEMI)—display distinct pathophysiological profiles. STEMI is most often triggered by acute plaque rupture and complete coronary occlusion, whereas NSTEMI is more frequently associated with diffuse, multivessel atherosclerotic disease, reflecting the chronic progression of coronary atherosclerosis.[2]
Lipoprotein(a) is considered a major genetically determined risk factor for cardiovascular disease, with circulating levels largely unaffected by environmental factors or lifestyle modifications. Recent studies have consistently demonstrated that elevated Lp(a) concentrations are linked to an increased risk of premature coronary events, independent of LDL cholesterol and other traditional risk factors. [3,4] However, the current body of literature focuses mainly on the role of Lp(a) in the occurrence of myocardial infarction, with far less attention to its differential implications in STEMI versus NSTEMI phenotypes and its association with the extent of coronary artery disease in young patients.
2. Materials and Methods
2.1. Study Design and Population
Our study was conducted on two patient cohorts enrolled over a 6-month period at the Craiova County Emergency Clinical Hospital. We enrolled young patients with acute ST-segment elevation myocardial infarction (STEMI, n = 88) and those with acute non-ST-segment elevation myocardial infarction (NSTEMI, n = 63) admitted to the Cardiology Clinic. The study was observational. Sample sizes and the composition of the two groups are documented in the manuscript’s results section.
Clinical and demographic variables available at admission/assessment were collected: sex, age, body mass index (BMI; analyzed both as a continuous and a categorical variable—normal weight/overweight/obesity), smoking status(Figure 1), and diagnoses of diabetes mellitus (Figure 2) and hypertension( Figure 3). The lipid profile included low density lipoprotein cholesterol (LDL-C) and high density lipoprotein cholesterol (HDL-C), measured in mg/dL, and lipoprotein(a) (Lp(a)) was quantified; we subsequently set a threshold of 30 mg/dL (Figure 4) for stratifying the risk of multivessel coronary involvement. (Table 1)
2.2. Definitions and Measurements
The diagnosis of STEMI/NSTEMI was established according to the center’s standard clinical and paraclinical assessment, in line with current guidelines of the European Society of Cardiology. The extent of coronary artery disease was assessed by coronary angiography and classified as single-vessel versus multivessel disease. Significant lesions were defined as stenoses greater than 70% of the vessel lumen.
2.3. Objectives
The primary objective was to compare clinical and biological characteristics between STEMI and NSTEMI. Secondary objectives included: (i) analyses stratified by Lp(a) level (≤30 vs >30 mg/dL) (Figure 5) to compare STEMI with NSTEMI within each stratum, and (ii) evaluation of the association between Lp(a) ≥30 mg/dL and the presence of multivessel coronary disease separately in STEMI and in NSTEMI. The subgroup structures (Lp(a) ≤30 mg/dL and >30 mg/dL) and the outcome variable (multivessel vs single-vessel) are detailed in the tables in the Results section.
2.4. Statistical Analysis
Continuous variables were summarized as medians and interquartile ranges (IQRs), and categorical variables as counts and percentages. Distributions between the two groups were compared using nonparametric tests for independent samples (Mann–Whitney/Kruskal–Wallis, as appropriate) and χ² or Fisher’s exact tests for categorical variables. To estimate effects on the probability of multivessel disease, separate binary regression models were built for the NSTEMI and STEMI cohorts, reporting relative risks (RRs) with 95% confidence intervals and p-values. In adjusted models, predictors included Lp(a) (≥30 vs <30 mg/dL) and available clinico-metabolic covariates (sex, age, BMI, diabetes mellitus, LDL-C). Statistical significance was set at p < 0.05.
2.5. Data Management
Analyses were performed on complete cases using the consolidated database (n = 151). Measurement units were kept consistent. The variable structures, BMI categories, and the predefined Lp(a) threshold also derive from the dataset and the tables attached to the manuscript.
3. Results
The analysis of clinical and demographic characteristics revealed significant differences between patients with acute myocardial infarction and the control group. In the STEMI cohort, the majority of patients were male (81.8%), a proportion comparable to that observed in NSTEMI patients (76.2%), but significantly higher than in the control group, where the sex distribution was balanced (50% men and 50% women, p<0.001). The median age of STEMI and NSTEMI patients was 48.0 and 50.0 years, respectively, significantly higher than that of the controls, who had a median age of 34.0 years (p<0.001).
Regarding body mass index, obesity was predominant among STEMI patients (51.1%), while NSTEMI patients were more frequently overweight (66.7%). In contrast, individuals with normal weight predominated in the control group (64.3%), with statistically significant differences between groups (p<0.001). Smoking status showed a high prevalence of smokers in the STEMI group (76.1%), compared with NSTEMI (52.4%) and controls (50.0%, p=0.002).
Diabetes mellitus was present in 27.3% of STEMI patients and 28.6% of NSTEMI patients, whereas none of the control participants had this condition (p<0.001). Arterial hypertension was also frequently encountered among infarction patients, being reported in 64.8% of STEMI and 76.2% of NSTEMI cases, compared with its complete absence in the control group (p<0.001).
The lipid profile showed significant differences across groups. LDL-cholesterol values were highest in STEMI patients (median 133 mg/dL), compared with NSTEMI (103 mg/dL) and controls (110 mg/dL, p<0.001). HDL-cholesterol levels were significantly lower in STEMI (39.1 mg/dL) and NSTEMI (41.2 mg/dL) patients compared with controls (55.0 mg/dL, p<0.001).
With regard to lipoprotein(a), a significantly higher proportion of myocardial infarction patients presented values >30 mg/dL, specifically 56.8% in STEMI and 65.1% in NSTEMI, compared with 31.0% in the control group (p=0.002)
The subgroup analysis of patients with low lipoprotein(a) levels (<30 mg/dL, n=60) revealed differences between STEMI and NSTEMI patients(Table 2). The median age was significantly lower in the STEMI cohort (48.0 years) compared with NSTEMI patients (52.0 years, p=0.039).
With regard to the lipid profile, HDL-cholesterol values did not differ between the two groups (36.4 mg/dL in STEMI vs. 36.3 mg/dL in NSTEMI, p=0.607). In contrast, LDL-cholesterol was significantly higher in STEMI patients (129.4 mg/dL) compared with NSTEMI patients (80.5 mg/dL, p<0.001) (Figure 6).
Body mass index(BMI) was also higher in the STEMI group (30.5 kg/m²) comparing within NSTEMI (27.7 kg/m², p=0.021), suggesting an association between obesity and infarct type. Sex distribution was similar, with a high proportion of men in both groups (86.8% in STEMI and 86.4% in NSTEMI, p=1.000).
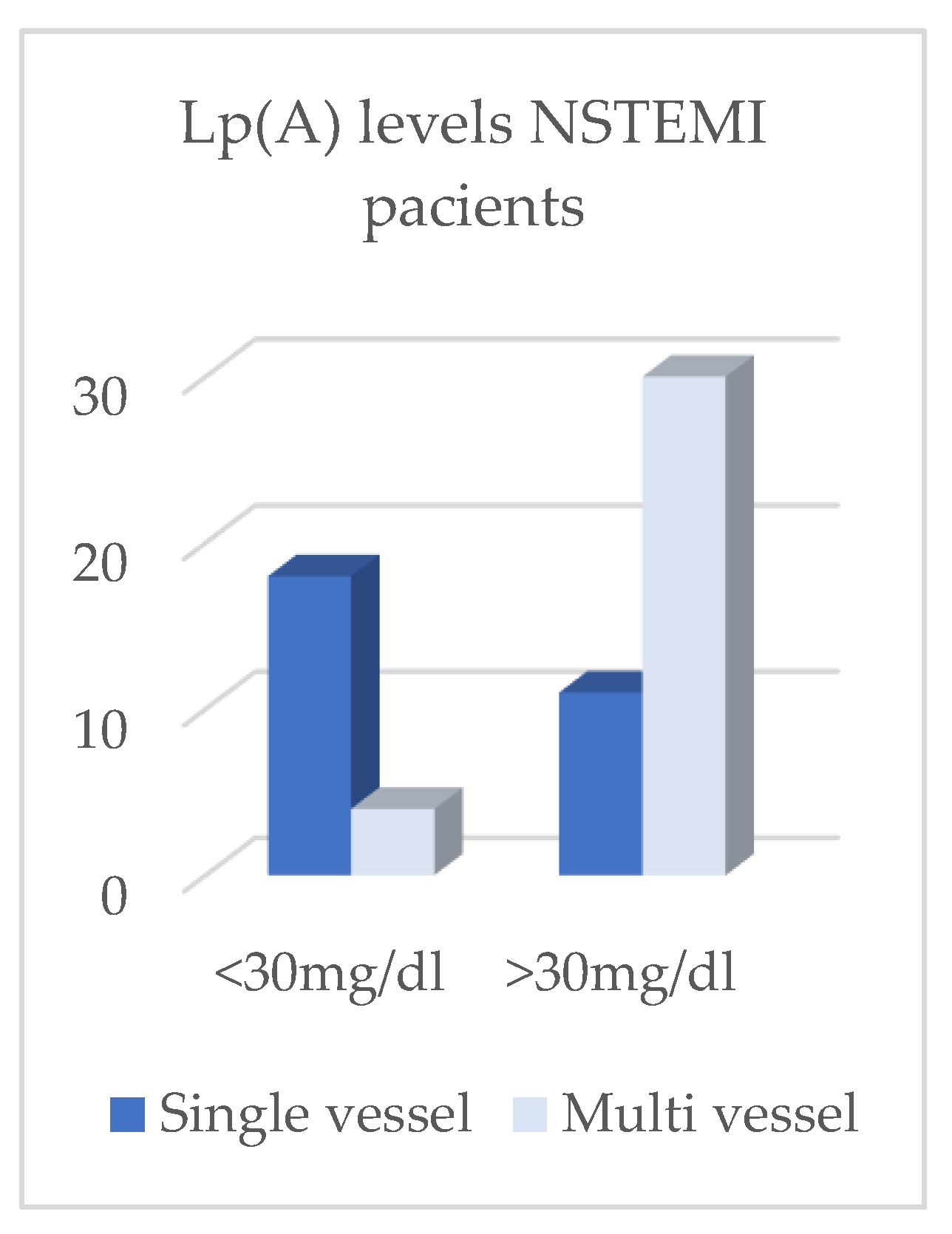
The assessment of coronary artery disease extent showed a comparable prevalence of single-vessel and multivessel lesions between the two subgroups. Single-vessel disease predominated (78.9% in STEMI and 81.8% in NSTEMI), while multivessel involvement was observed in 21.1% of STEMI patients and 18.2% of NSTEMI patients, with no statistically significant differences (p=1.000) (Figure 8, Figure 10, Figure 12 and Figure 13).
Figure 6.
Caption.
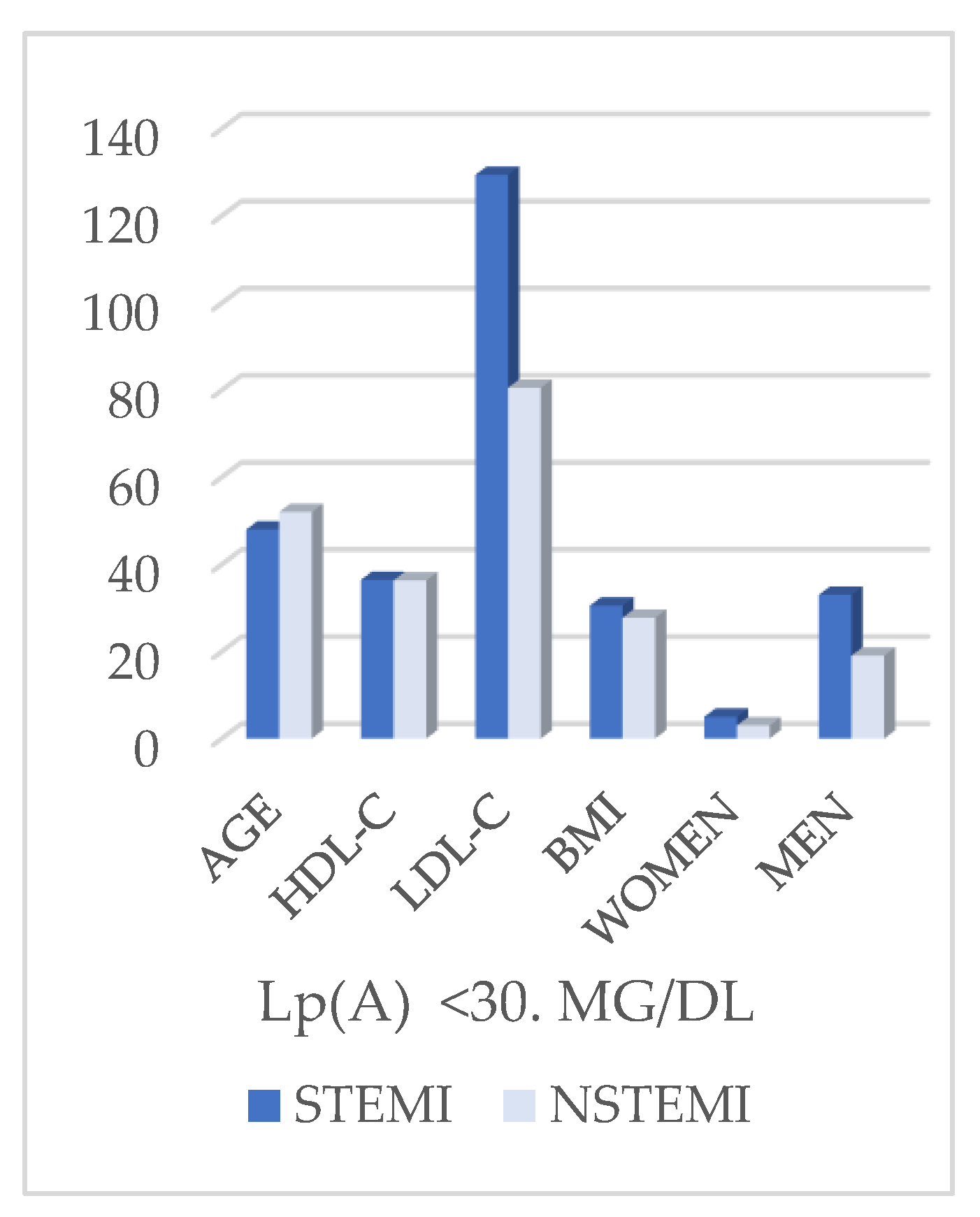
Figure 7.
Caption.
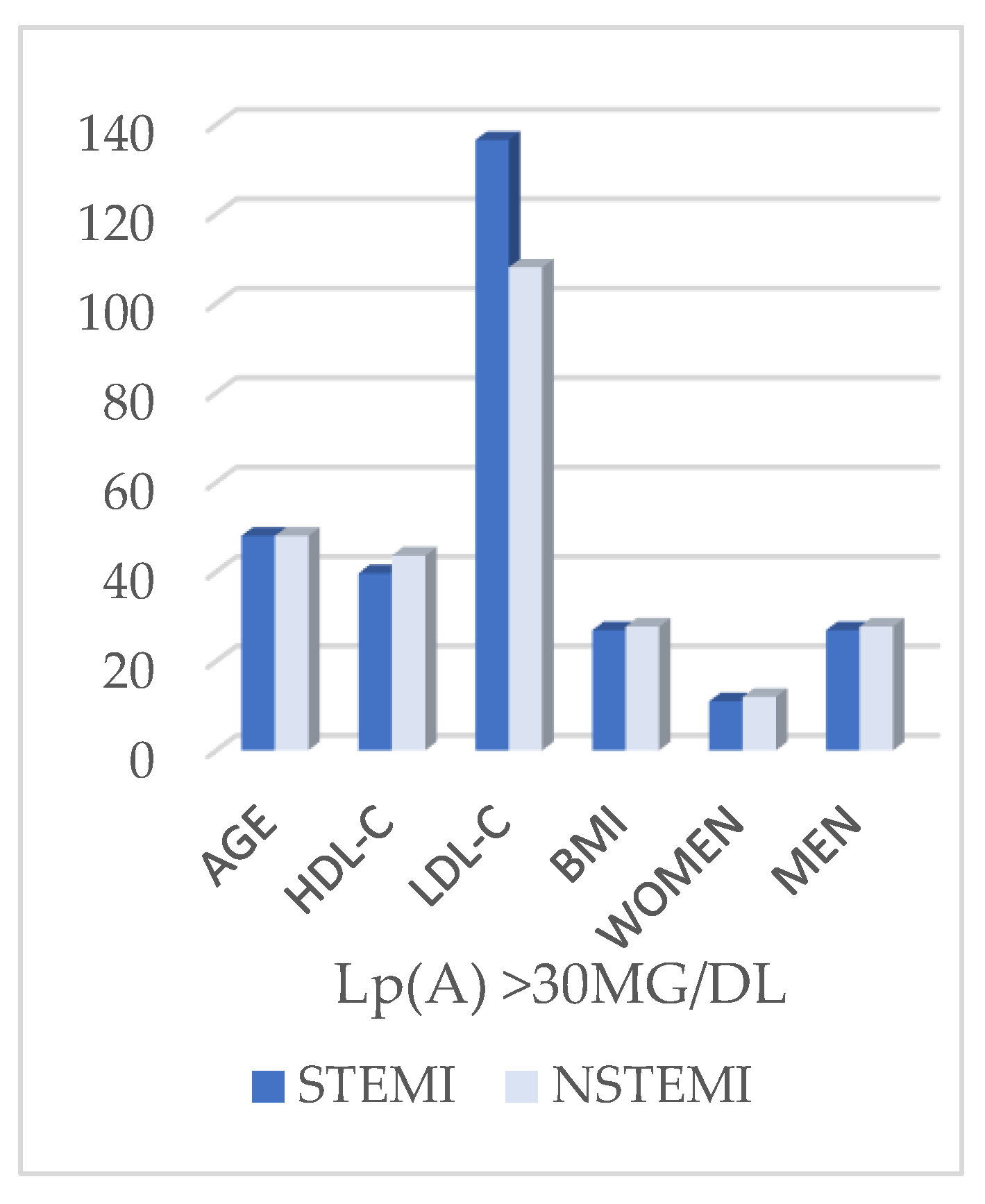
Figure 8.
Caption.
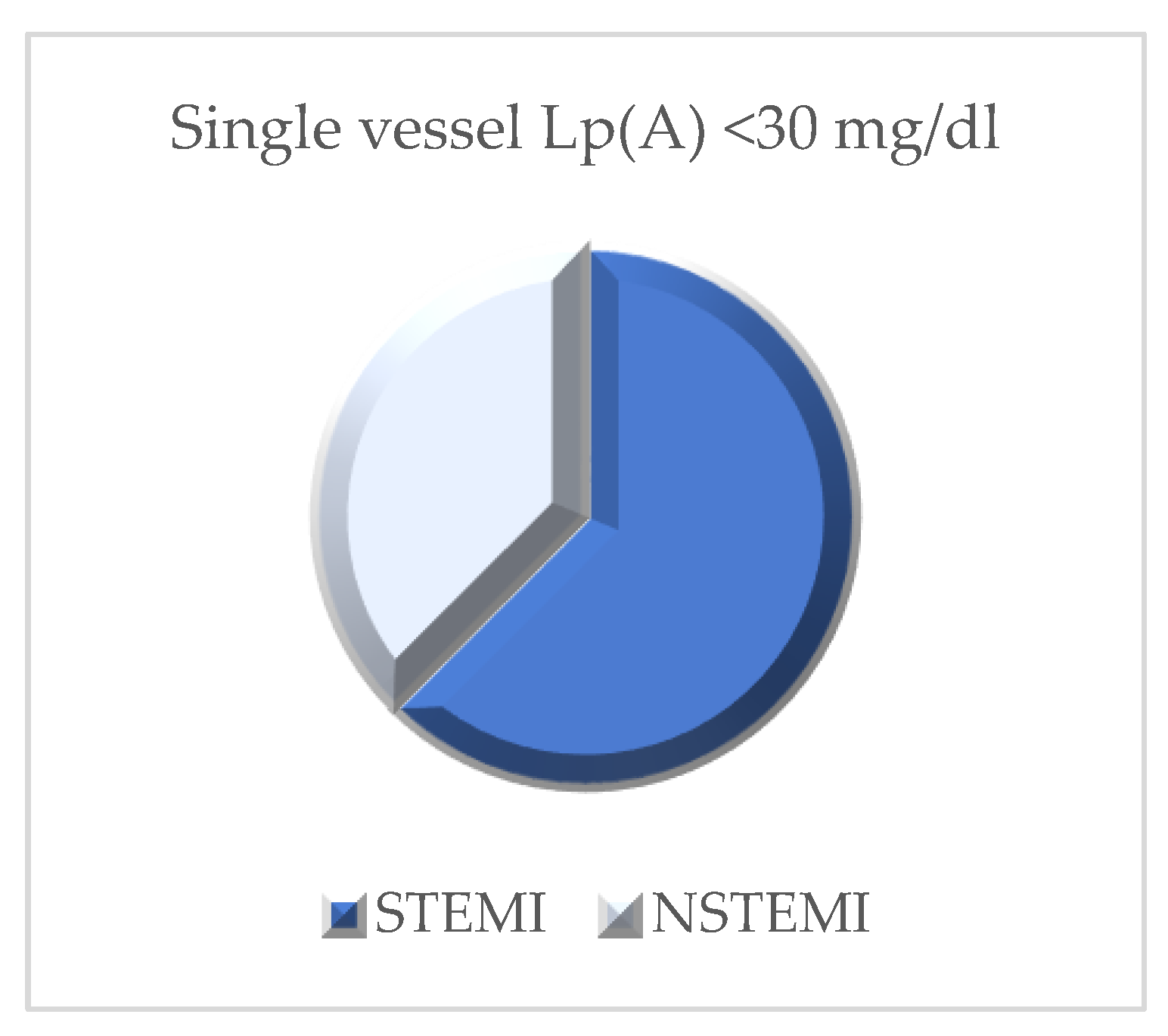
Figure 9.
Caption.
In the subgroup of patients with elevated lipoprotein(a) levels (>30 mg/dL, n=91) (Table 3), no significant differences were observed in median age between STEMI and NSTEMI patients (48.0 years vs. 48.0 years, p=0.251). HDL-cholesterol values were also comparable between the two groups (39.6 mg/dL in STEMI vs. 43.6 mg/dL in NSTEMI, p=0.089) (Figure 7), and body mass index showed similar values (26.9 vs. 27.7 kg/m², p=0.808). Sex distribution did not differ significantly, although men were more frequently represented in both cohorts (78.0% STEMI vs. 70.7% NSTEMI, p=0.474).
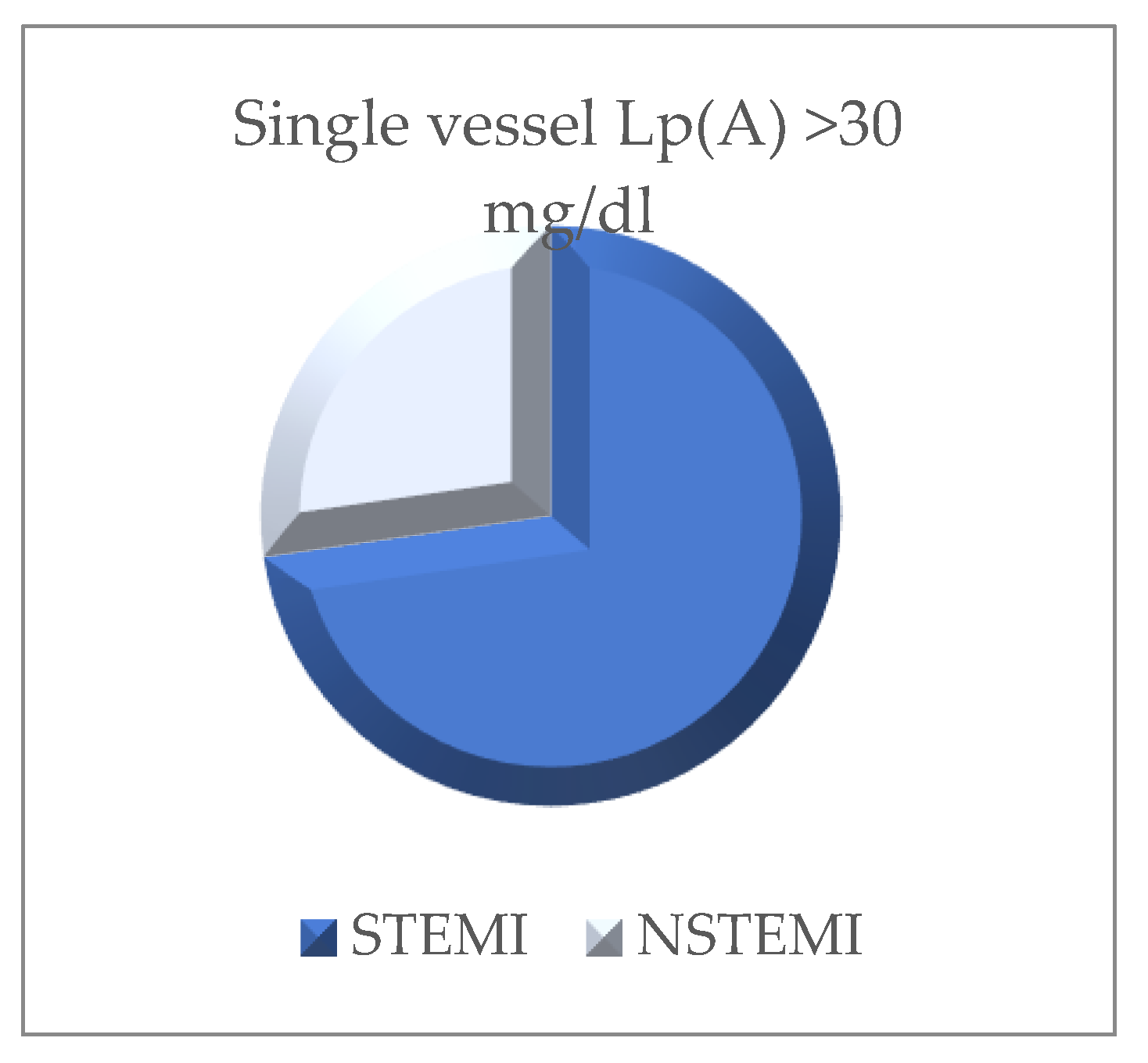
In contrast, important differences were found regarding the lipid profile and the extent of coronary artery disease.(Figure 9Figure 11Figure 12Figure 13) LDL-cholesterol was significantly higher in STEMI patients (137.5 mg/dL) compared with NSTEMI patients (108.0 mg/dL, p=0.004). Angiographic analysis revealed a distinct distribution: STEMI patients predominantly presented with single-vessel disease (64.0%), whereas NSTEMI patients more frequently exhibited multivessel disease (73.2%, p<0.001) (Figure 9Figure 11Figure 12Figure 13).
Figure 10.
Caption.
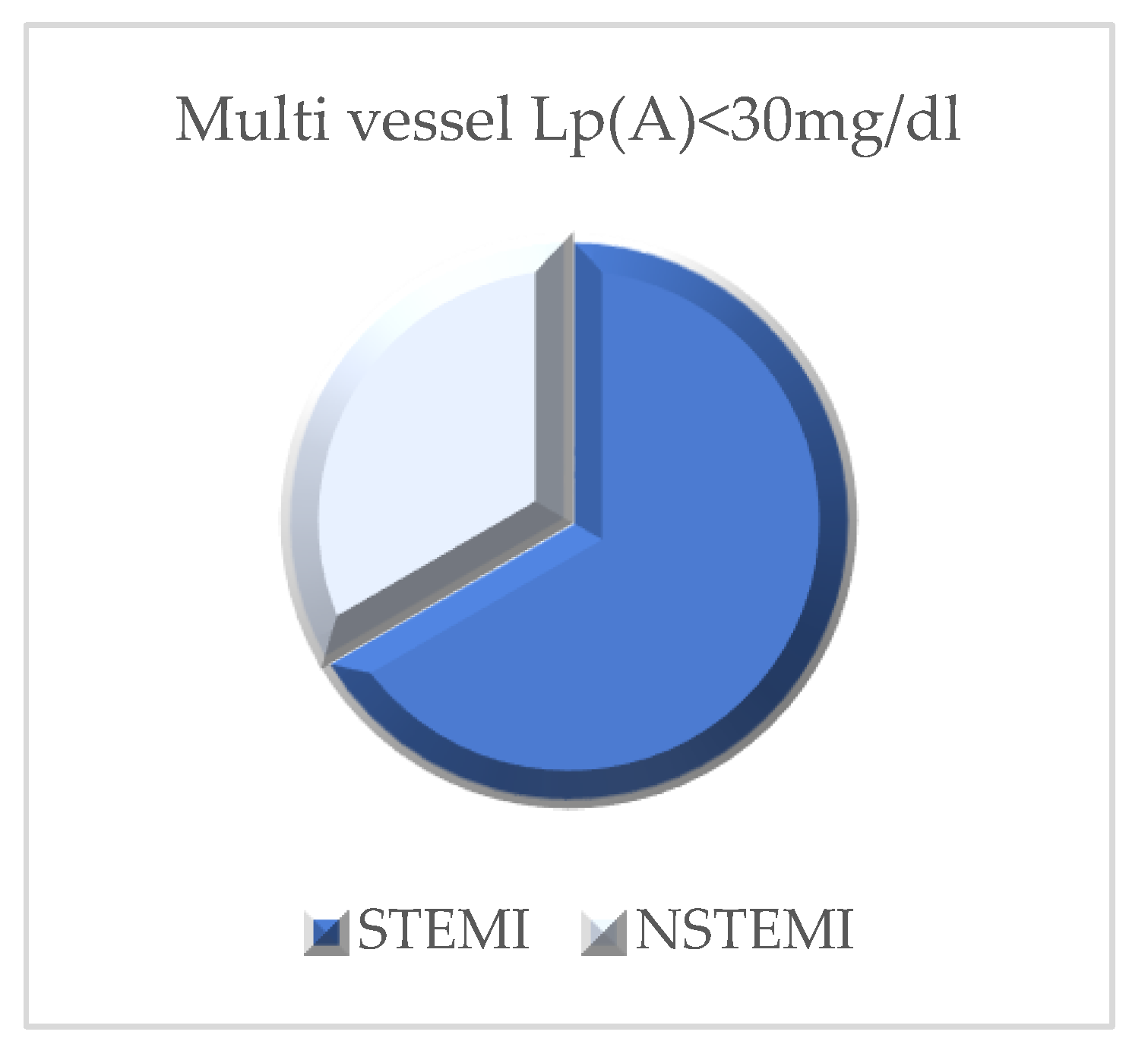
Figure 11.
Caption.
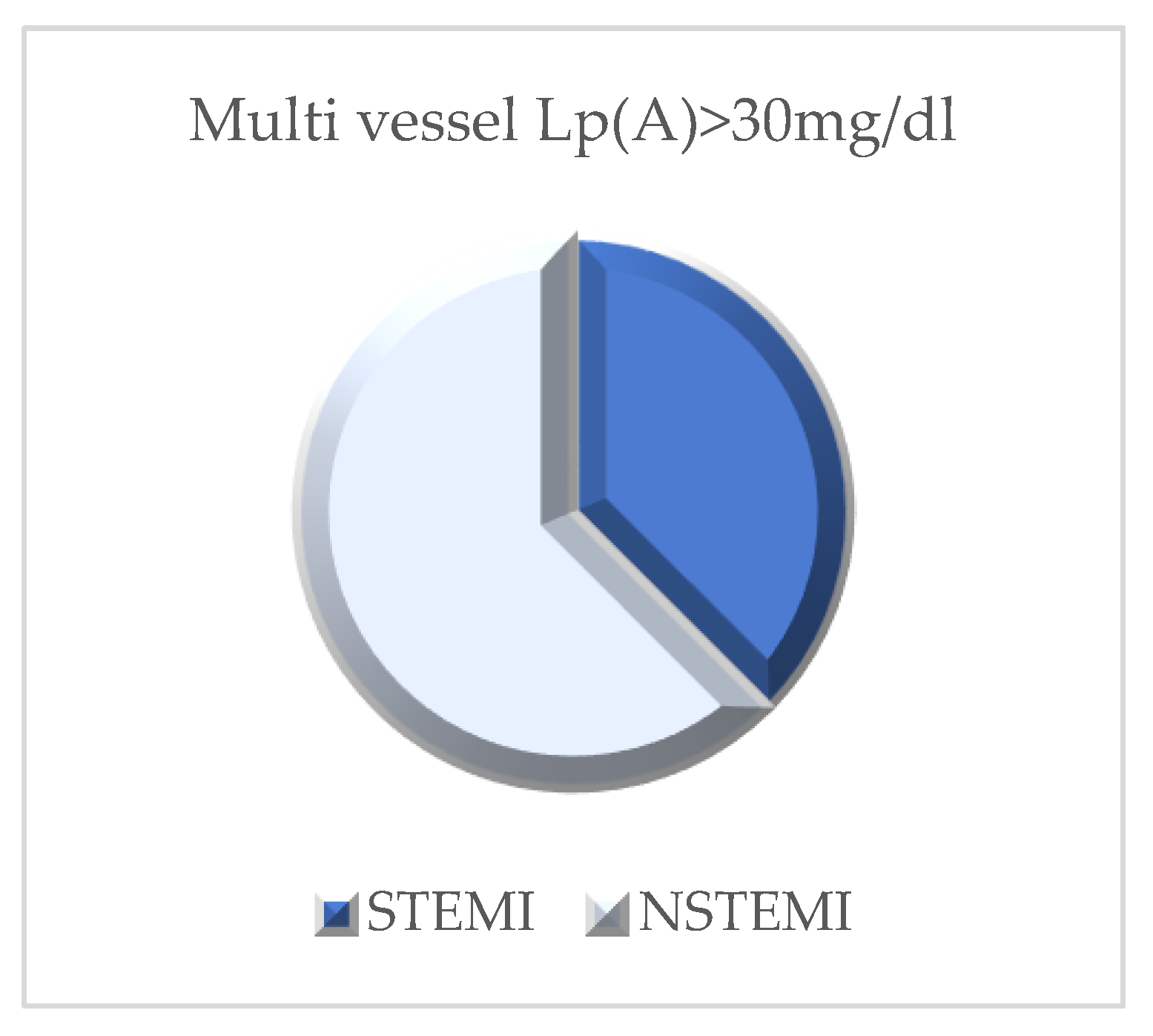
Figure 12.
Caption.
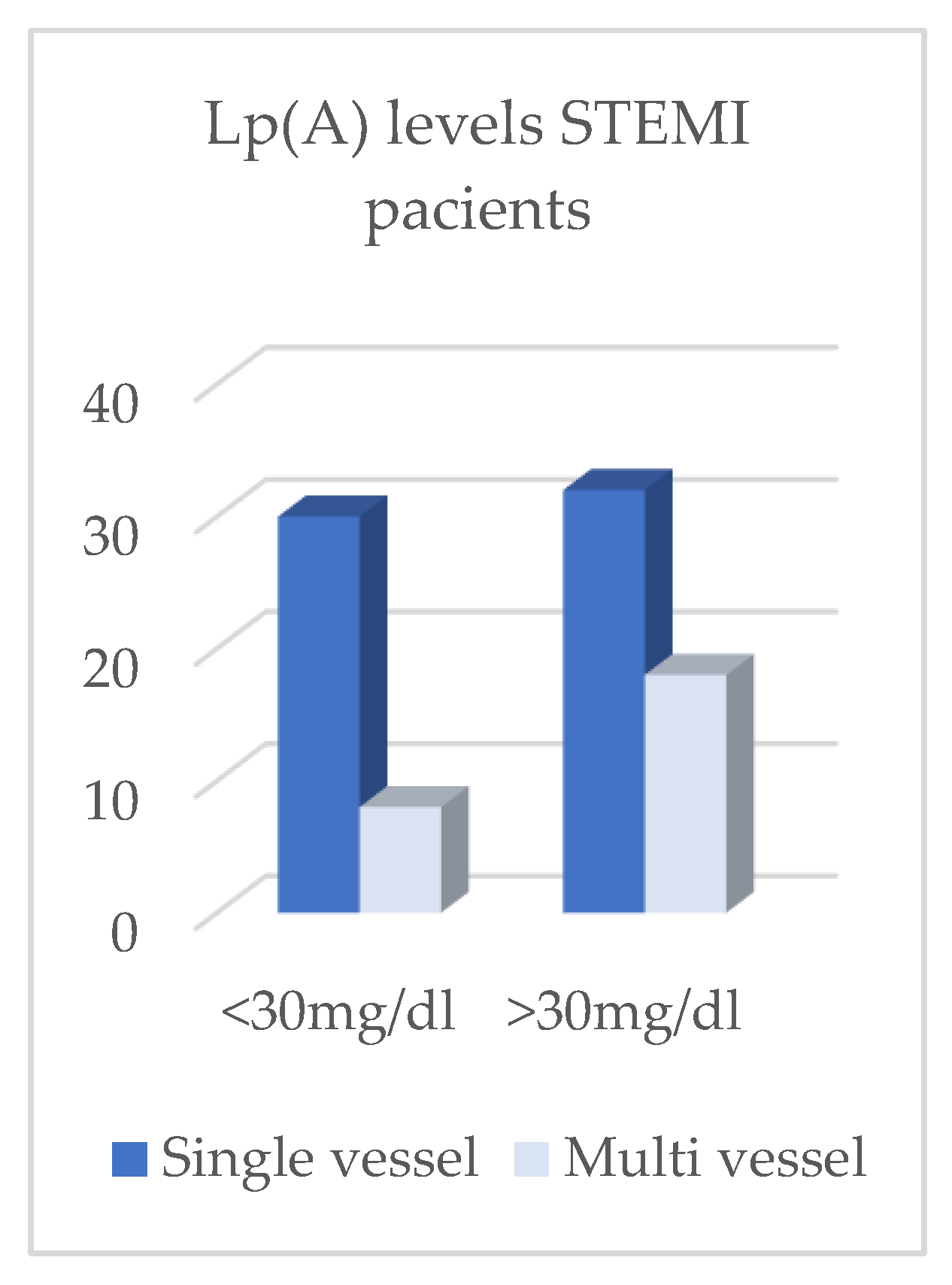
Figure 13.
Caption.
In summary, while LDL-cholesterol concentrations remained consistently higher among STEMI patients irrespective of lipoprotein(a) levels, elevated Lp(a) was strongly associated with an increased burden of multivessel coronary artery disease, predominantly in the NSTEMI cohort, thereby highlighting its potential contributory role in the pathophysiology and progression of diffuse atherosclerotic disease (Table 2, Figure 7).
In the NSTEMI cohort (n = 63, Table 4), elevated lipoprotein(a) [Lp(a) ≥30 mg/dL] was strongly associated with multivessel coronary artery disease. The estimated relative risk (RR) was 4.25 (95% CI, 1.73–10.45; p = 0.0016), indicating an approximately fourfold higher risk relative to patients with Lp(a) <30 mg/dL. Among the additional covariates examined, only body mass index (BMI) demonstrated a statistically significant association: per 5 kg/m² increase, RR 1.55 (95% CI, 1.01–2.38; p = 0.043). Male sex (RR 1.54; p = 0.130), diabetes (RR 1.29; p = 0.285), age (per +5 years; RR 1.05; p = 0.646), and LDL-C (per +10 mg/dL; RR 0.99; p = 0.773) were not statistically significant.
In the STEMI cohort (n = 88, Table 5) , Lp(a) ≥30 mg/dL remained independently associated with multivessel involvement, although with a more modest effect size: adjusted RR 1.78 (95% CI, 1.10–2.90; p = 0.020). In this cohort, diabetes was also significantly associated (RR 1.71; 95% CI, 1.07–2.74; p = 0.026), and higher LDL-C conferred additional risk (per +10 mg/dL, RR 1.05; 95% CI, 1.00–1.10; p = 0.044). Male sex (RR 1.37; p = 0.329), age (per +5 years; RR 0.98; p = 0.804), and BMI (per +5 kg/m²; RR 1.07; p = 0.471) were not significantly associated.
Comparative analyses showed that the association between Lp(a) ≥30 mg/dL and multivessel disease was stronger in NSTEMI than in STEMI (RR 4.25 vs 1.78) (Table 4 and Table 5). This differential magnitude suggests that elevated Lp(a) is more clinically informative for the extent of coronary involvement in NSTEMI, whereas in STEMI its effect persists but is accompanied by independent contributions from diabetes and from the atherogenic burden reflected by LDL-C.
Taken together, these findings indicate that an Lp(a) threshold of ≥30 mg/dL is a robust marker of multivessel coronary artery disease, particularly among patients with NSTEMI—whereas in STEMI, Lp(a) remains relevant but its effect is comparable to that of diabetes and more modest than in NSTEMI, with LDL-C also exerting an independent influence.
4. Discussion
Through this study and the results obtained, we sought to evaluate and highlight the role of lipoprotein (a) in young patients with acute myocardial infarction and to compare different cohorts of myocardial infarction presentation such as STEMI and NSTEMI, by examining its association with the extent of coronary artery disease. Our results show that elevated Lp(a) (≥30 mg/dL) are significantly associated with multivessel disease, with a stronger effect observed in patients with NSTEMI compared to those with STEMI. These findings highlight important pathophysiological differences between the two clinical entities and reinforce the role of Lp(a) as a relevant biomarker in coronary risk stratification.[1,6].
Consistent with data from the literature, we observed that patients with STEMI were generally more obese, more frequently smokers, and had higher LDL-C levels compared with patients with NSTEMI, suggesting a profile of acute plaque rupture triggered by metabolic and lifestyle-related risk factors.[5,6,7,8,9]. By contrast, patients with NSTEMI more frequently exhibited multivessel coronary artery disease, reflecting a more diffuse and chronic atherosclerotic burden, within which Lp(a) may exert a stronger pathogenic contribution. [8]This aligns with existing evidence showing that elevated Lp(a) levels promotes pro-atherogenic and pro-thrombotic pathways, leading to extensive coronary involvement rather than isolated plaque rupture.[11].
Regression analyses provide further support for this differential pattern. Among patients with NSTEMI, Lp(a) levels ≥30 mg/dL were associated with more than a fourfold increase in the risk of multivessel disease. In contrast, the effect size in STEMI was more modest (RR 1.78), with diabetes and LDL-C also emerging as independent contributors. Taken together, these results indicate that while Lp(a) is relevant in both clinical settings, it serves as a particularly strong predictor in NSTEMI, where it may help identify patients at higher risk of diffuse coronary involvement.[12] From a clinical standpoint, our results suggest that systematic Lp(a) testing could enhace risk stratification in young patients with myocardial infarction, particularly those presenting with NSTEMI. Early identification of elevated Lp(a) levels may inform more aggressive preventive strategies, including intensive lipid-lowering therapy, emerging Lp(a)-targeted agents currently under development, as well as closer surveillance to optimize secondary prevention.[13,14].
Our study also underscores the importance of interpreting Lp(a) levels in the context of other cardiometabolic risk factors. Within the STEMI cohort, diabetes and LDL-C retained significant associations with multivessel disease, underscoring the multifactorial nature of coronary risk in this group. This observation highlights that therapeutic strategies should not only address Lp(a), but also ensure rigourous management of traditional risk factors, particularly LDL-C and diabetes and early introduction of targeted therapy.[15,16,17,18,19].
Limitations
The sample size was relatively small and originated from a single center, which may limit the generalizability of the results. In addition, the absence of long-term follow-up prevents the evaluation of the prognostic impact of elevated Lp(a) levels on the risk of recurrent events.
5. Conclusions
Lipoprotein(a) exerts a substantially greater impact in NSTEMI than in STEMI. Among young patients with elevated Lp(a) levels (≥30 mg/dL), the likelihood of diffuse coronary artery disease is more than fourfold higher in NSTEMI, whereas in STEMI its contribution is comparatively modest and largely influenced by concomitant risk factors such as diabetes mellitus and elevated LDL cholesterol. These observations underscore fundamental pathophysiological differences between these infarct phenotypes and strongly support the systematic assessment of Lp(a) as an adjunctive tool for coronary risk stratification, particularly in young patients presenting with NSTEMI. Confirmation of these findings through large-scale, multicenter studies with extended follow-up is warranted to further elucidate the prognostic significance of Lp(a) in secondary prevention strategies.
Author Contributions
Conceptualization, S.I.C., I.C.B; methodology, I.C,B.; resources, A.M.B, I.C.B, M.T.C, I.D, M.I, G.C.T, C.M. writing—S.I.C., I.C.B, P.A.C and O.I.; writing—review and editing, . E.N.Ț and I.C.B., S.I.C. All authors have read and agreed to the published version of the manuscript.
Funding
The Article Processing Charge were funded by the University of Medicine and Pharmacy od Craiova, România.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of University of Medicine and Pharmacy of Craiova (181/09.07.2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Acknowledgments
The Article Processing Charge were funded by the University of Medicine and Pharmacy od Craiova, România.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| Lp(A) | Lipoprotein(A) |
| LDL-C | Low density lipoprotein cholesterol |
| HDL-C | High density lipoprotein cholesterol |
| HR | Hazard Ration |
| STEMI | ST-Elevation myocardical infarction |
| NSTEMI | Non-ST- Elevation myocardical infarction |
| RR | Relative risk |
| BMI | Body mass index |
| CI | Confidence Interval |
| P | P-value |
References
- Tsimikas S. A Test in Context: Lipoprotein(a): Diagnosis, Prognosis, Controversies, and Emerging Therapies. J Am Coll Cardiol [Internet]. 2017 Feb 14 [cited 2024 Sep 11];69(6):692–711. Available from: https://pubmed.ncbi.nlm.nih.gov/28183512/.
- Meyers HP, Bracey A, Lee D, Lichtenheld A, Li WJ, Singer DD, et al. Comparison of the ST-Elevation Myocardial Infarction (STEMI) vs. NSTEMI and Occlusion MI (OMI) vs. NOMI Paradigms of Acute MI. Journal of Emergency Medicine [Internet]. 2021 Mar 1 [cited 2025 Aug 25];60(3):273–84. Available from: https://pubmed.ncbi.nlm.nih.gov/33308915/. [CrossRef]
- Buciu IC, Tieranu EN, Pircalabu AS, Istratoaie O, Zlatian OM, Cioboata R, et al. Exploring the Relationship Between Lipoprotein (a) Level and Myocardial Infarction Risk: An Observational Study. Medicina 2024, Vol 60, Page 1878 [Internet]. 2024 Nov 16 [cited 2024 Nov 18];60(11):1878. Available from: https://www.mdpi.com/1648-9144/60/11/1878/htm. [CrossRef]
- Kronenberg, F. Lipoprotein(a). Handb Exp Pharmacol [Internet]. 2022 [cited 2024 Sep 13];270:201–32. Available from: https://pubmed.ncbi.nlm.nih.gov/36122123/.
- Țieranu EN; Cureraru SI; Târtea GC; Vlăduțu V-C; Cojocaru PA; Piorescu MTL; Dincă D; Popescu R; Militaru C; Donoiu I;.; et al. Acute Myocardial Infarction and Diffuse Coronary Artery Disease in a Patient with Multiple Sclerosis: A Case Report and Literature Review. J. Clin. Med. 2025, 14, 4304. [CrossRef]
- Cojocaru A; Zavaleanu AD; Călina DC; Gheonea DI; Osiac E; Boboc IKS; Militaru C; Militaru S; Buciu IC; Țieranu EN;.; et al. Different Age Related Neurological and Cardiac Effects of Verapamil on a Transgenic Mouse Model of Alzheimer’s Disease. Curr. Health Sci. J. 2021, 47, 263–269. [CrossRef]
- Volgman AS, Koschinsky ML, Mehta A, Rosenson RS. Genetics and Pathophysiological Mechanisms of Lipoprotein(a)-Associated Cardiovascular Risk. J Am Heart Assoc [Internet]. 2024 Jun 18 [cited 2025 Aug 25];13(12):33654. Available from: /doi/pdf/10.1161/JAHA.123.033654?download=true. [CrossRef]
- Zaheen M, Pender P, Dang QM, Sinha E, Chong JJH, Chow CK, et al. Myocardial Infarction in the Young: Aetiology, Emerging Risk Factors, and the Role of Novel Biomarkers. Journal of Cardiovascular Development and Disease 2025, Vol 12, Page 148 [Internet]. 2025 Apr 10 [cited 2025 Aug 25];12(4):148. Available from: https://www.mdpi.com/2308-3425/12/4/148/htm. [CrossRef]
- Młynarska E, Czarnik W, Fularski P, Hajdys J, Majchrowicz G, Stabrawa M, et al. From Atherosclerotic Plaque to Myocardial Infarction—The Leading Cause of Coronary Artery Occlusion. International Journal of Molecular Sciences 2024, Vol 25, Page 7295 [Internet]. 2024 Jul 2 [cited 2025 Aug 25];25(13):7295. Available from: https://www.mdpi.com/1422-0067/25/13/7295/htm. [CrossRef]
- Baumann AAW, Tavella R, Air TM, Mishra A, Montarello NJ, Arstall M, et al. Prevalence and real-world management of NSTEMI with multivessel disease. Cardiovasc Diagn Ther [Internet]. 2022 Feb 1 [cited 2025 Aug 25];12(1):11–11. Available from: https://cdt.amegroups.org/article/view/89578/html. [CrossRef]
- Patel D, Koschinsky ML, Agarwala A, Natarajan P, Bhatia HS, Mehta A, et al. Role of Lipoprotein(a) in Atherosclerotic Cardiovascular Disease in South Asian Individuals. J Am Heart Assoc [Internet]. 2025 Jul 15 [cited 2025 Aug 25];14(14):eJAHA. Available from: /doi/pdf/10.1161/JAHA.124.040361?download=true. [CrossRef]
- Buciu IC, Tieranu EN, Pircalabu AS, Zlatian OM, Donoiu I, Militaru C, et al. The Relationship between Lipoprotein A and the Prevalence of Multivessel Coronary Artery Disease in Young Patients with Acute Myocardial Infarction: An Observational Study. Biomedicines [Internet]. 2024 Sep 1 [cited 2024 Oct 13];12(9). Available from: https://pubmed.ncbi.nlm.nih.gov/39335672/. [CrossRef]
- Lopes Almeida Gomes L, Forman Faden D, Xie L, Chambers S, Stone C, Werth VP, et al. Modern therapy of patients with lupus erythematosus must include appropriate management of their heightened rates of atherosclerotic cardiovascular events: a literature update. Lupus Sci Med [Internet]. 2025 Apr 8 [cited 2025 Aug 25];12(1):e001160. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11979607/.
- Reyes-Soffer G, Yeang C, Michos ED, Boatwright W, Ballantyne CM. High lipoprotein(a): Actionable strategies for risk assessment and mitigation. Am J Prev Cardiol [Internet]. 2024 Jun 1 [cited 2025 Aug 25];18:100651. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11031736/. [CrossRef]
- Shiyovich A, Berman AN, Besser SA, Biery DW, Kaur G, Divakaran S, et al. Association of Lipoprotein (a) and Standard Modifiable Cardiovascular Risk Factors With Incident Myocardial Infarction: The Mass General Brigham Lp(a) Registry. Journal of the American Heart Association: Cardiovascular and Cerebrovascular Disease [Internet]. 2024 May 31 [cited 2025 Aug 25];13(10):e034493. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC11179826/. [CrossRef]
- Tsimikas S, Fazio S, Ferdinand KC, Ginsberg HN, Koschinsky ML, Marcovina SM, et al. NHLBI Working Group Recommendations to Reduce Lipoprotein(a)-Mediated Risk of Cardiovascular Disease and Aortic Stenosis. J Am Coll Cardiol. 2018 Jan 16;71(2):177–92. [CrossRef]
- Cojocaru, P.A.; Țieranu, M.L.; Piorescu, M.T.L.; Buciu, I.C.; Belu, A.M.; Cureraru, S.I.; Țieranu, E.N.; Moise, G.C.; Istratoaie, O. Myocardical Infarction in Young Adults: Revisiting Risk Factors and Atherothrombotic Pathways. Medicina 2025, 61, 1615. [Google Scholar] [CrossRef]
- Donoiu I, Târtea G, Sfredel V, Raicea V, Țucă AM, Preda AN, Cozma D, Vătășescu R. Dapagliflozin Ameliorates Neural Damage in the Heart and Kidney of Diabetic Mice. Biomedicines. 2023 Dec 16;11(12):3324. [CrossRef]
- Dhankhar S, Chauhan S, Mehta DK, Nitika, Saini K, Saini M, Das R, Gupta S, Gautam V. Novel targets for potential therapeutic use in Diabetes mellitus. Diabetol Metab Syndr. 2023 Feb 13;15(1):17. [CrossRef]
Figure 1.
Caption.
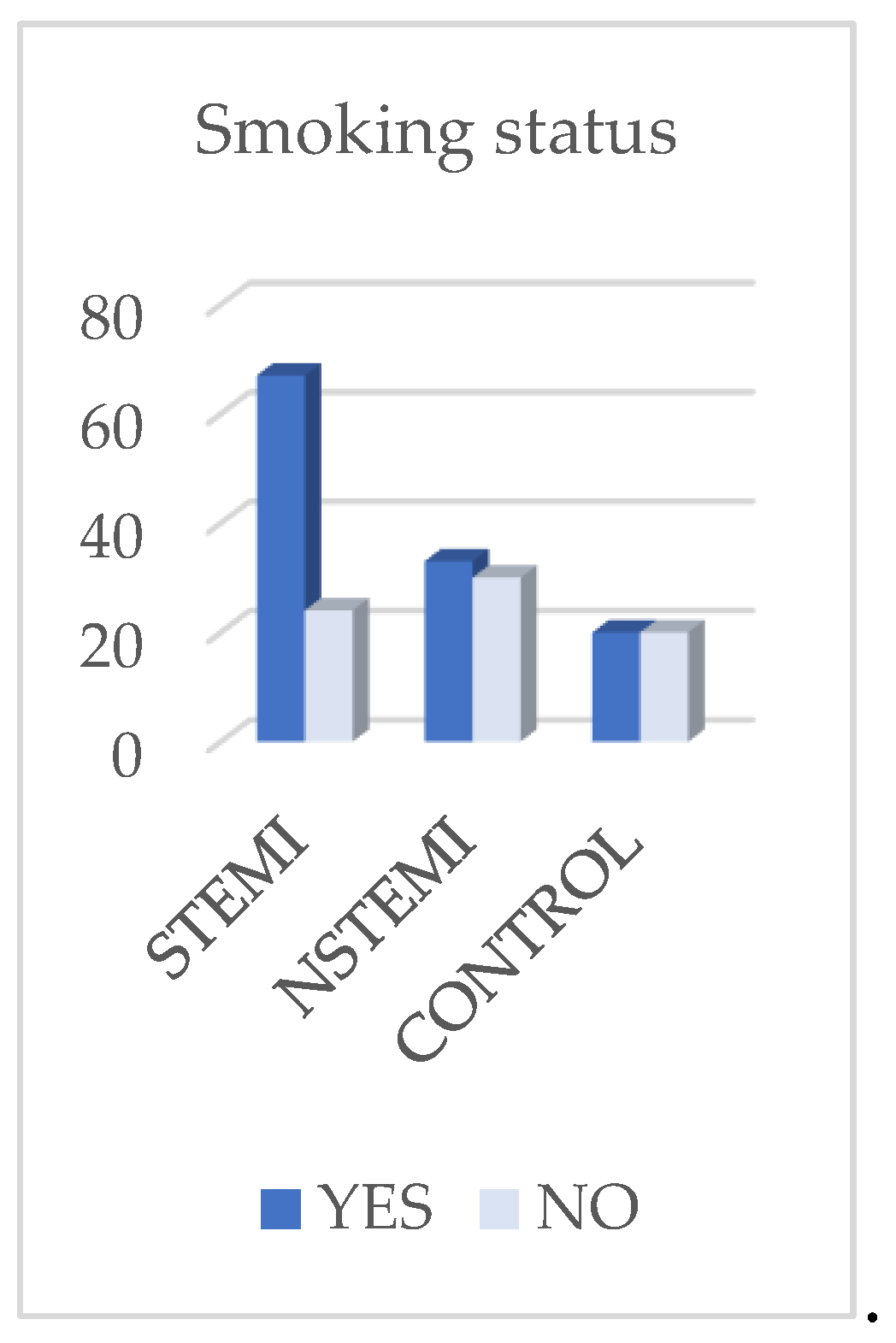
Figure 2.
Caption.
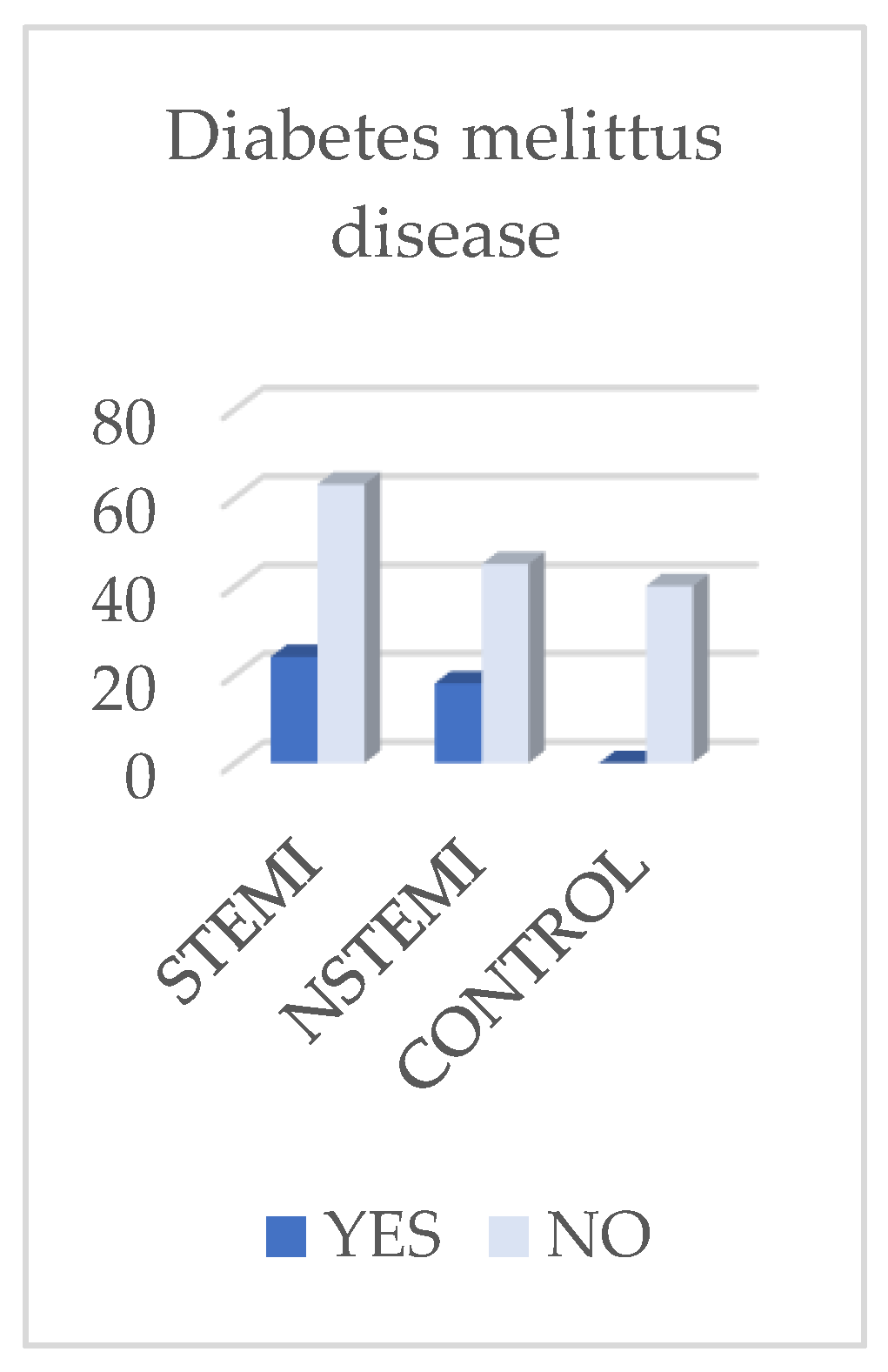
Figure 3.
Caption.
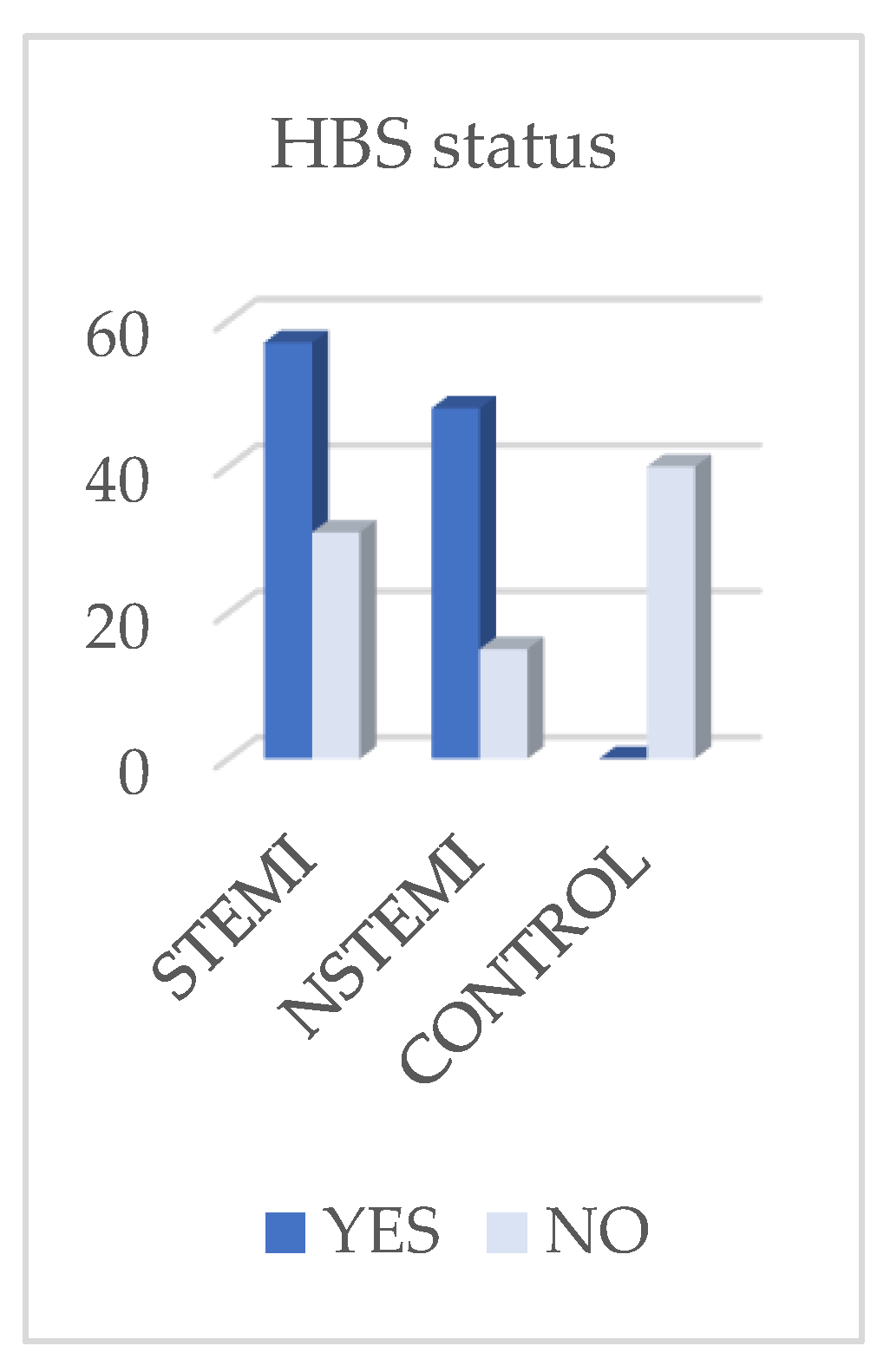
Figure 4.
Caption.
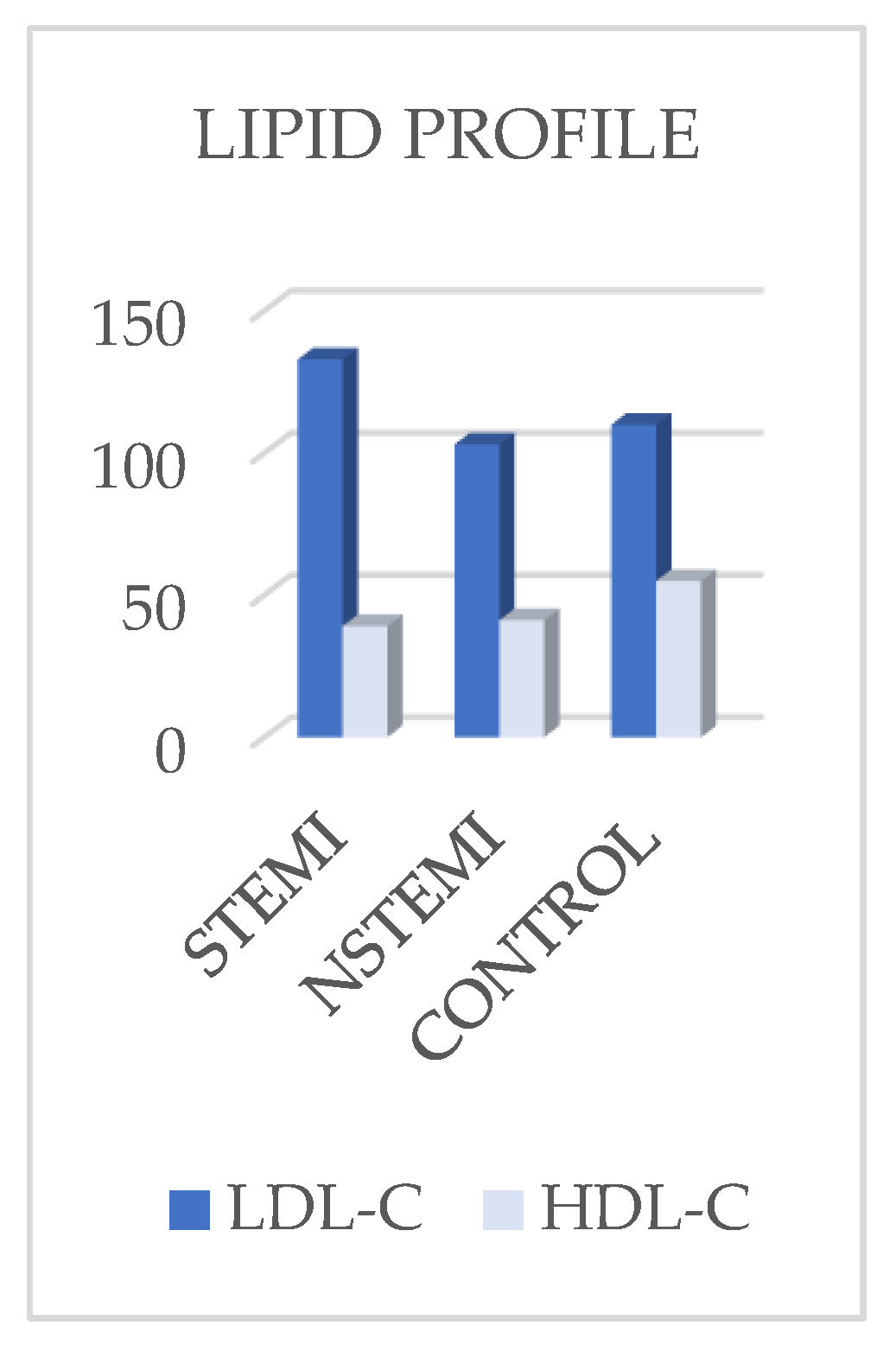
Figure 5.
Caption.
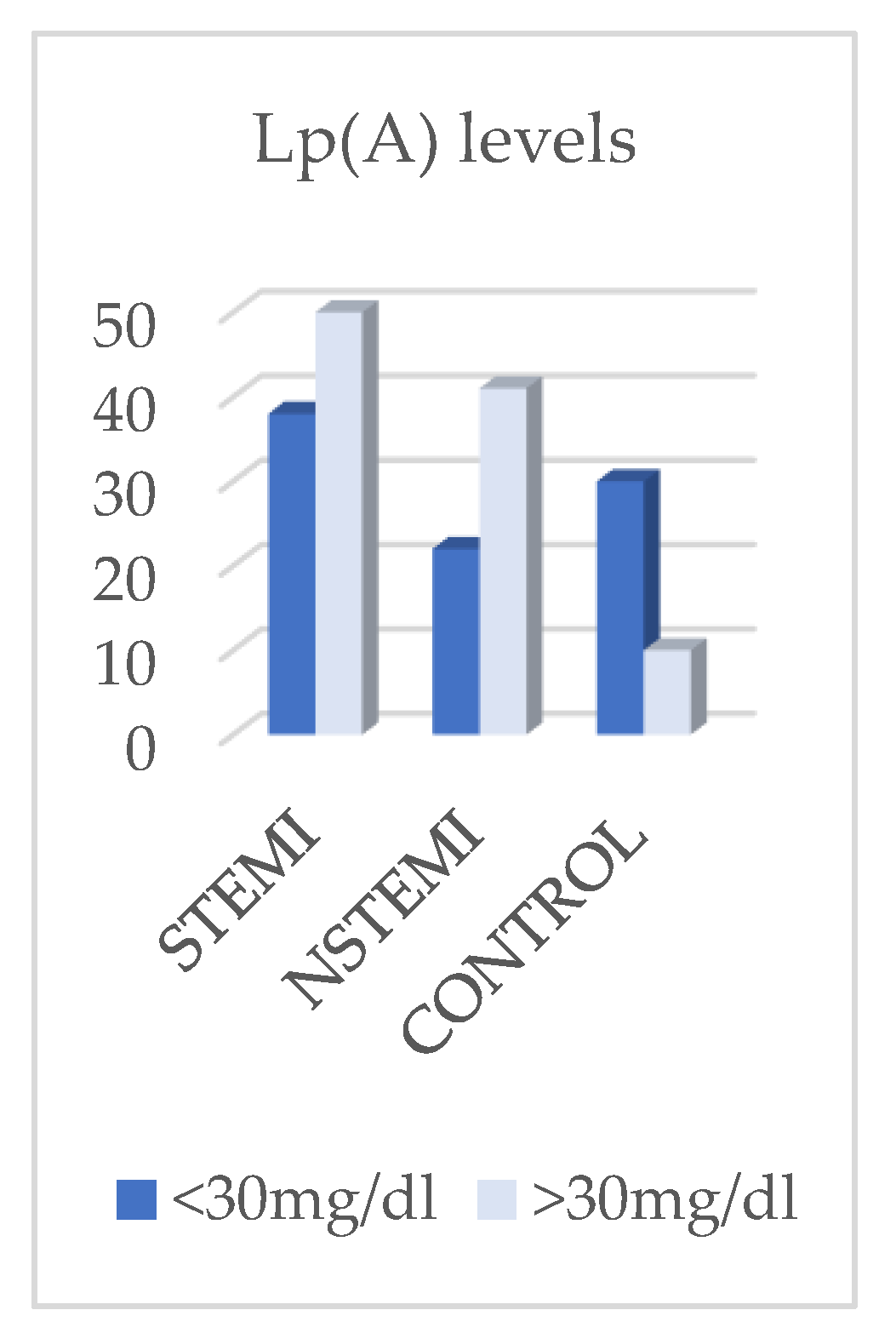

Table 1.
Clinical, demographic and laboratory characteristics of the studies groups.
| Parameter | STEMI n= 88 No. (%) Median(IQR) |
NSTEMI n= 63 No. (%) Median(IQR) |
CONTROL n=40 No. (%) Median(IQR) |
P | |
|---|---|---|---|---|---|
| Gender |
Men |
72(81,8%) |
48(76,2%) |
20 (50%) |
< 0,001 |
| Women |
16 (18,2%) |
15( 23,8%) |
20 (50%) |
< 0,001 |
|
| AGE | 48,0 (43,8 – 54,2) | 50,0 (46,0 – 53,0) | 34,0 (29,0 – 40,0) | < 0,001 | |
|
BMI |
Standard |
27 (30,7 %) |
12 (19,0 %) |
20 (64,3 %) |
< 0,001 |
| Overweight |
16 (18,2 %) |
42 (66,7 %) |
10 (23,8 %) |
< 0,001 |
|
| Obesity | 45 (51,1 %) | 9 (14,3 %) | 10 (23,8 %) | < 0,001 | |
|
Smoking status |
Smoke | 67 (76,1%) | 33 (52,4%) | 20 (50,0 %) |
0,002 |
| Non-smoke | 21 (23,9 %) | 30 (47,6 %) | 20 (50,0 %) | ||
| Dibetes mellitus |
YES | 24 (27,3 %) | 18 (28,6 %) | 0 (0 %) |
< 0,001 |
| NO | 64 (72,7 %) | 45 (71,4 %) | 40 (100 %) | ||
| HBP status | YES | 57 (64,8 %) | 48 (76,2 %) | 0 (0 %) |
< 0,001 |
| NO | 31 (35,2 %) | 15 (23,8 %) | 40 (100 %) | ||
| LDL Cholesterol | 133 (100 – 168) | 103 (79,0 – 121) | 110 (90,0 – 123) | < 0,001 | |
|
HDL Cholesterol |
39,1 (32,1 – 44,8) | 41,2 (36,3 – 51,9) |
55,0 (46,4 – 60,0) | < 0,001 | |
|
Lipoprotein (a) level |
Lp (a) ≤ 30 mg/dL |
38 (43,2 %) |
22 (34,9 %) |
30 (66,67 %) |
0,002 |
| Lp (a) > 30 mg/dL | 50 (56,8 %) |
41 (65,1 %) | 10 (33,33 %) | ||
Table 2.
-Analyses stratified by Lp(a) level (≤30 mg/dl.
| Parameter | STEMI (n = 38) | NSTEMI (n = 22) | p-value* |
|---|---|---|---|
| Age (years) | 48,0 (43,0 – 54,0) | 52,0 (51,0 – 54,5) | 0,039 |
| HDL-C (mg/dL) | 36,4 (31,7 – 44,5) | 36,3 (28,5 – 53,2) | 0,607 |
| LDL-C (mg/dL) | 129,4 (89,2 – 157,0) | 80,5 (67,9 – 113,2) | < 0,001 |
| BMI (kg/m²) | 30,5 (26,4 – 34,4) | 27,7 (26,4 – 28,6) | 0,021 |
| Men | 33 (86,8 %) | 19 (86,4 %) | 1,000 — |
| Women | 5 (13,2 %) | 3 (13,6 %) | |
| Sigle-Vessel Disease | 30 (78,9 %) | 18 (81,8 %) | 1,000 |
| Multi-Vessel Disease | 8 (21,1 %) | 4 (18,2 %) |
Table 3.
Analyses stratified by Lp(a) level >30 mg/dl.
| Parameter | STEMI (n = 50) | NSTEMI (n = 41) | p-value ✧ |
|---|---|---|---|
| Age (Years) | 48,0 (45,0 – 54,8) | 48,0 (43,0 – 50,0) | 0,251 |
| HDL-C (mg/dL) | 39,6 (33,1 – 49,9) | 43,6 (38,8 – 44,9) | 0,089 |
| LDL-C (mg/dL) | 137,5 (108,5 – 180,6) | 108,0 (93,0 – 145,0) | 0,004 |
| BMI (kg/m²) | 26,9 (24,2 – 32,1) | 27,7 (24,9 – 29,4) | 0,808 |
| Men | 39 (78,0 %) | 29 (70,7 %) | 0,474 — |
| Women | 11 (22,0 %) | 12 (29,3 %) | |
| Single-vassel disease | 32 (64,0 %) | 11 (26,8 %) | < 0,001 — |
| Multi-vessel disease | 18 (36,0 %) | 30 (73,2 %) |
Table 4.
Logistic regression in NSTEMI cohort.
| Predictor | RR | CI | p |
|---|---|---|---|
| Lp(a) ≥30 mg/dl (vs <30) | 4.25 | 1.73–10.45 | 0.0016 |
| Gender (men vs women) | 1.54 | 0.88–2.68 | 0.130 |
| Diabetus mellitus (yes or no) | 1.29 | 0.81–2.05 | 0.285 |
| Age(+5 years) | 1.05 | 0.86–1.29 | 0.646 |
| LDL-C (+10 mg/dl) | 0.99 | 0.95–1.04 | 0.773 |
| IMC (+5 kg/m²) | 1.55 | 1.01–2.38 | 0.043 |
Table 5.
Logistic regression in STEMI cohort.
| Predictor | RR | CI | p |
|---|---|---|---|
| Lp(a) ≥30 mg/dl (vs <30) | 1,78 | 1,10–2,90 | 0,020 |
| Gender (men vs women) | 1,37 | 0,73–2,56 | 0,329 |
| Diabetus mellitus (yes or no) | 1,71 | 1,07–2,74 | 0,026 |
| Age(+5 years) | 0,98 | 0,81–1,18 | 0,804 |
| LDL-C (+10 mg/dl) | 1,05 | 1,00–1,10 | 0,044 |
| IMC (+5 kg/m²) | 1,07 | 0,90–1,27 | 0,471 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



