
Submitted:
01 September 2025
Posted:
02 September 2025
You are already at the latest version
Abstract
(1) Background: Tobacco smoking remains a critical public health concern in Indonesia, particularly in Aceh Province, where male smoking prevalence reaches 56.12%. Cultural permissiveness and weak enforcement of tobacco control regulations have contributed to this high prevalence. Women, especially wives, are central figures in family health and may play an essential role in influencing household smoking behavior. However, their roles and strategies remain underexplored, especially in conservative cultural settings; (2) Methods: This qualitative study employed a Participatory Action Research (PAR) approach to examine the roles of women in controlling the smoking behavior of family members in Aceh. A total of 75 research subjects were selected from three districts (Aceh Singkil, Gayo Lues, and Pidie Jaya) using a combination of purposive sampling and snowball sampling methods. Data were collected through semi-structured in-depth interviews and were analyzed thematically using NVivo 15 software. The analysis framework was based on Lawrence Green’s PRECEDE model, which includes predisposing, enabling, and reinforcing factors; (3) Results: The study found that women demonstrated progressive attitudes toward smoking, evolving from passive acceptance to active responsibility. They employed both persuasive strategies (health education, emotional appeals, and motivation) and coercive actions (household smoking bans, threats, and withdrawal of privileges). Women also positioned themselves as health monitors and guardians within the household. Despite cultural limitations and gender hierarchy, many participants reported partial or complete success in encouraging their husbands to quit smoking, particularly when supported by religious norms and health awareness; (4) Conclusions: Women play a pivotal role in shaping smoking-related behavior in the family. Empowering women through participatory frameworks and culturally tailored interventions can enhance their effectiveness as health advocates. This study underscores the need to integrate gender-sensitive strategies into national tobacco control policies, especially in culturally conservative regions.
Keywords:
smoking cessation
; women's role
; family health
; participatory action research
; qualitative research
; Aceh
; Indonesia
1. Introduction
Tobacco use is one of the leading preventable causes of morbidity and mortality worldwide. According to the World Health Organization (WHO), tobacco kills more than 8 million people each year [1], including 1.2 million non-smokers exposed to secondhand smoke [2]. Despite global efforts to reduce tobacco consumption through regulatory policies, taxation, and public education campaigns, smoking remains prevalent in many low- and middle-income countries, particularly among men [3].
Indonesia ranks among the countries with the highest smoking prevalence in Southeast Asia. The 2018 Basic Health Research (Riskesdas) reported that 28.9% of the Indonesian population smokes, with 55.8% of adult males being active smokers [4]. In the province of Aceh, the situation is even more concerning, with male smoking prevalence reaching 56.12%, placing it among the highest in the country [5]. Cultural acceptance, weak enforcement of anti-smoking policies, and local norms that perceive smoking as part of male identity have all contributed to this public health challenge [6].
While tobacco control policies often focus on legislative action and mass media campaigns, less attention has been paid to the role of the family unit, especially women, in influencing smoking behavior at the household level [7]. Women, particularly wives and mothers, play a critical role in shaping family health practices. Their involvement in caregiving, health promotion, and behavioral monitoring positions them as potential agents of change in tobacco cessation efforts [8]. However, in patriarchal and culturally conservative societies such as Aceh, gender power dynamics, religious norms, and social expectations often limit women’s ability to intervene effectively in male-dominated behaviors such as smoking [9].
Several studies have examined social and environmental factors influencing smoking behavior. Still, there remains a lack of research exploring the active agency of women in tobacco control within traditional family systems [10]. The current literature does not sufficiently capture the strategies, constraints, and coping mechanisms employed by women who seek to reduce smoking behaviors in their households [11]. Furthermore, there is limited application of participatory frameworks that empower women not only as caregivers but also as community-based health advocates.
To address this gap, the present study explores the role of women in controlling the smoking behavior of family members in Aceh using a Participatory Action Research (PAR) approach. This method enables the co-construction of knowledge and community-led strategies grounded in local values and lived experiences. By doing so, the study aims to contribute to the development of more inclusive and culturally sensitive tobacco control interventions in Indonesia and similar contexts. This study makes a significant contribution to the tobacco control literature in low- and middle-income countries (LMICs) by offering a contextually grounded, community-based perspective on how women in culturally and religiously conservative regions such as Aceh, Indonesia, develop household-level smoking cessation strategies. Unlike most studies that focus on macro-level policies or quantitative data, this research fills a significant knowledge gap by presenting first-hand narratives of subjective experiences and relational dynamics that shape tobacco control within the domestic sphere.
1.1. Literature Review
1.1.1. Tobacco Use and Family Dynamics
Tobacco consumption remains a significant global public health issue, causing more than 8 million deaths annually [12]. In low- and middle-income countries, where smoking prevalence is higher among men, exposure to secondhand smoke often disproportionately affects women and children in the household [13]. The domestic setting becomes a critical environment for both exposure and intervention. Studies have highlighted the significant role of family dynamics in influencing smoking behaviors [14]. Family support, particularly from spouses, has a measurable impact on smoking cessation outcomes. Their research indicates that when family members actively support quitting efforts, the likelihood of successful cessation increases [15]. This underscores the necessity to explore the interpersonal and household context of smoking behavior beyond the individual smoker.
1.1.2. The Role of Women in Health Advocacy
Women are typically regarded as central health managers within the family, a role consistently observed in both global health discourse and local contexts, such as Indonesia, including Aceh. This positioning reflects their everyday responsibilities in ensuring household nutrition, caregiving, and health-related decision-making. As caregivers, mothers, and spouses, women hold substantial influence over health-related decisions, including diet, healthcare utilization, and lifestyle habits such as smoking [16]. In conservative or patriarchal societies, such as Aceh, this influence is often culturally embedded, although not always explicitly acknowledged [17]. Previous studies have demonstrated the informal yet powerful authority of women in promoting smoke-free environments at home [18]. For instance, preview research documented how women households used social persuasion and emotional appeals to alter husbands’ smoking behaviors [19]. Similar dynamics are seen in Southeast Asia, where women act as mediators between public health messages and family-level behavioral change [20].
1.1.3. Smoking Cessation and Family-Based Interventions
Effective smoking cessation often involves more than just individual willpower; it is also shaped by the environment in which the smoker resides. Family-based interventions have gained recognition for their potential to enhance the success of smoking cessation programs [21]. The social pressure and emotional attachment within families were more influential than public health campaigns alone [22]. Furthermore, interventions that include family education particularly those targeting wives and mothers have demonstrated improved outcomes in terms of smoking motivation and relapse prevention [23]. Such findings emphasize the need to empower non-smoking family members, especially women, as key actors in cessation programs.
1.1.4. The PRECEDE Model as a Behavioral Framework
The PRECEDE-PROCEED model developed serves as a strategic planning framework for health promotion and behavioral interventions [24]. The PRECEDE component (Predisposing, Reinforcing, and Enabling Constructs in Educational Diagnosis and Evaluation) is particularly relevant to this study, as it offers a systematic approach to identifying behavioral determinants [25]. Predisposing factors include knowledge, beliefs, values, and attitudes that may influence readiness to change. Enabling factors refer to conditions that facilitate or hinder the change process, such as access to resources or services [26]. Reinforcing factors include social support or feedback that sustains behavioral change, such as encouragement from religious leaders or local regulations. Numerous studies that have applied the PRECEDE model to tobacco control have found it effective in identifying barriers and mobilizing community-based strategies [27]. Its flexibility allows for adaptation to cultural settings, making it suitable for application in Aceh.
1.1.5. Participatory Action Research (PAR) and Community Engagement
PAR is a collaborative research approach that actively involves community members in identifying problems and developing solutions [28]. It is grounded in empowerment and co-creation of knowledge, particularly relevant when addressing behavior deeply rooted in culture and social norms [29]. Preview research argues that PAR facilitates genuine community ownership of health programs, which leads to greater sustainability and relevance [30]. In tobacco control, PAR enables women to share their experiences and influence interventions that reflect their realities [31]. The other researcher demonstrated that involving women in designing smoke-free campaigns in low-income settings led to higher compliance and engagement [32]. In the context of Aceh, PAR supports the inclusion of women not only as study participants but also as agents of transformation, bridging public health goals with cultural realities.
1.2. Conceptual Framework of Study
This study proposes an emergent conceptual framework based on the thematic findings described above. The framework illustrates the mechanisms through which women influence smoking behavior in the household and redefine gendered roles in health promotion. Figure 1 highlights how women act as central agents in promoting family health by influencing behaviors related to smoking through a combination of internal motivation and external support. Their role is shaped by enabling factors, such as access to health services, economic capacity, and education, as well as by reinforcing factors like support from religious leaders and encouragement from family. When these elements align, they facilitate behavior change and lead to a decrease in smoking among family members, underscoring women’s strategic position in health advocacy within households.
1.3. Research Questions
To understand the sociocultural dynamics and participatory role of women in promoting smoking cessation within Acehnese households, this study was guided by a series of research questions rooted in the PRECEDE model (Predisposing, Enabling, Reinforcing factors). These questions were designed to explore not only individual behavior but also structural and cultural influences that shape women’s capacity as health advocates in their families. The participatory action research (PAR) framework enabled researchers and participants to collaboratively examine and reflect on women who demonstrated the ability to intervene directly in their household’s smoking behavior by implementing smoke-free rules, placing visual reminders (e.g., no-smoking signs), engaging in emotional dialogue with their husbands, and leveraging religious and community figures to reinforce anti-smoking messages. The following research questions were formulated:
What roles do women play in influencing the smoking cessation behavior of their family members in Acehnese households?
- What are the predisposing factors (e.g., knowledge, attitudes, and intentions) that affect women’s involvement in supporting smoking cessation within the family?
- How do enabling factors (e.g., access to health services, economic conditions, and health education) facilitate or hinder women’s efforts in promoting smoke-free home environments?
- What reinforcing factors (e.g., religious values, family support, and local regulations) contribute to the effectiveness of women’s advocacy in controlling smoking behavior at home?
- How do women perceive their roles and responsibilities as health advocates within their households and communities concerning smoking behavior?
2. Materials and Methods
2.1. Study Design
This study employed an independent, exploratory qualitative design, guided by the Participatory Action Research (PAR) framework and the PRECEDE-PROCEED model [33]. Rather than implementing structured interventions, the study examined the cultural, social, and behavioral factors that influence women’s roles in household smoking cessation. Emphasis was placed on the co-construction of knowledge, where women and their families collaboratively developed practical strategies such as creating smoke-free zones, setting no-smoking times (e.g., during meals or around children), and displaying handwritten reminders. These strategies emerged through mutual dialogue and negotiation, reflecting women’s growing agency in health-related household decisions. Data were collected through two rounds of semi-structured interviews conducted at participants’ homes between June 2023 and March 2024. The first session gathered initial narratives, while the second session validated transcripts and confirmed emerging themes, thereby enhancing the trustworthiness of the findings. This participatory, iterative method underscores the importance of lived experiences in shaping culturally sensitive health advocacy and promoting behavioral change.
2.2. Study Setting and Participants
The study was conducted in three districts in Aceh Province, Indonesia: Aceh Singkil, Gayo Lues, and Pidie Jaya. These areas were intentionally chosen to reflect a diversity of local cultural and socioeconomic conditions. A total of 75 female participants were recruited through purposive and snowball sampling techniques. The inclusion criteria included women aged 18–50 years who were married and residing in the same household as a family member who had quit smoking for at least one year, had lived in the selected location for a minimum of one year, were physically and mentally healthy, and were willing to participate and provide informed consent. This study is categorized as participatory because it engaged women in reflecting on their roles and eliciting their lived experiences and insights, which are expected to serve as the foundation for designing future promotive public health programs.
2.3. Data Collection and Saturation
This study collected data through in-depth, semi-structured interviews conducted between June 2023 and March 2024 in participants’ homes, using either Bahasa Indonesia or the Acehnese dialect, depending on each participant’s language preference. To enhance data credibility, each participant was interviewed twice the first session aimed to gather initial narratives, while the second was conducted to verify transcripts and confirm emerging themes. The smoking status of husbands was determined through subjective self-reports provided by their wives, based on daily observations within the household. No biometric assessments or clinical verification methods were employed, as the study’s qualitative orientation emphasized capturing the women’s lived experiences and perceived relational dynamics rather than objectively measured behaviors. In this context, smoking cessation was operationally defined as the husband’s conscious effort to refrain from smoking within the home, particularly in the presence of children or other family members. This definition reflects a behavioral and relational shift rather than clinically confirmed abstinence.
2.4. Data Analysis
Thematic analysis was conducted using NVivo 15 software to facilitate systematic data coding and the identification of themes. The process included First-cycle coding – the initial open coding of interview transcripts to identify relevant statements and meanings - and second-cycle coding, which involved grouping and refining codes into broader categories and themes. Themes were organized in alignment with Lawrence Green’s PRECEDE model, focusing on predisposing, enabling, and reinforcing factors that influence smoking cessation behaviors in the family.
2.5. Data Trustworthiness (Validity and Reliability)
To establish the validity and reliability of the qualitative data, Lincoln and Guba’s four trustworthiness criteria were applied: Credibility: Achieved through prolonged engagement, triangulation across participant backgrounds and locations, and member checking via follow-up interviews. Transferability: Enhanced by providing thick descriptions of cultural context and participant experiences from three diverse districts. Dependability: Ensured through a transparent audit trail of data collection and analysis procedures and the consistent application of the interview protocol. Confirmability: Supported by the use of direct participant quotations and reflective journaling to minimize researcher bias.
2.6. Ethical Considerations
The study received ethical approval from the Ethics Committee of Syiah Kuala University, No. 102/EA/FK/2023. All participants signed informed consent forms after being informed of the research objectives, procedures, and their right to withdraw at any time. Confidentiality was maintained by anonymizing all participant identifiers. The study adhered to the ethical principles outlined in the Declaration of Helsinki and its subsequent amendments.
3. Results
3.1. Subject Characteristics
This participatory qualitative study investigated the role of women in influencing smoking cessation within families in three underprivileged districts of Aceh Province—Aceh Singkil, Gayo Lues, and Pidie Jaya. Drawing on data from 75 female participants, the analysis revealed how women act as agents of change by leveraging their social roles to promote smoke-free households. The findings were categorized into three domains: (1) Predisposing factors, including personal attitudes and knowledge about smoking; (2) Enabling factors, such as access to information and household economic dynamics; and (3) Reinforcing factors, including religious guidance and community norms. Women contributed significantly as caregivers, motivators, and informal health advocates, influenced by cultural, religious, and socioeconomic contexts. Supporting this, Table 1 presents the participants’ sociodemographic profiles, highlighting their maturity, diverse educational backgrounds, domestic responsibilities, and prior exposure to health education factors that shaped their capacity to support cessation behaviors in their households. These insights lay the groundwork for developing culturally grounded, community-based interventions in Aceh.
3.2. Data Validity
Table 2 presents the assessment of qualitative data trustworthiness based on Lincoln and Guba’s four criteria: credibility, transferability, dependability, and confirmability. Each aspect is clearly defined and accompanied by specific strategies implemented in this study to ensure methodological rigor in data collection and analysis processes. Table 2 presents the assessment of qualitative data trustworthiness based on Lincoln and Guba’s Refour criteria: credibility, transferability, dependability, and confirmability. Each aspect is defined and elaborated with specific processes undertaken in this study to ensure the rigor of data collection and analysis. The table also outlines key findings linked to each criterion and illustrates how these were applied within the research context. Through strategies such as prolonged engagement, triangulation, thick contextual descriptions, audit trails, and reflective journaling, the study ensures that the findings are both valid and reliable. This structured assessment strengthens the methodological integrity and supports the robustness of the participatory research outcomes in exploring women’s roles in controlling smoking behavior within Acehnese families.
3.3. Research Main Finding
Table 3 highlights five key themes that describe women’s strategies in promoting smoke-free households in Aceh. These include emotional motivations and assertive actions grounded in family health concerns, efforts to seek accurate health information, and the influence of religious teachings and cultural norms. Community support further legitimizes women’s advocacy, while personal empowerment enables them to become agents of change. Together, these factors illustrate a complex interplay of personal, social, and institutional elements that shape women’s leadership in tobacco control at the household level.
3.3.1. Women’s Perceived Role as Health Advocates in the Family
Table 4 reports how women take on proactive roles as health advocates within their families through three distinct forms. First, as social control agents, they apply persuasive, emotional, and religious strategies to discourage smoking indoors, particularly to protect children. Second, they act as family health protectors by physically asserting boundaries, such as posting “no smoking” signs to create a safer, smoke-free home environment. Third, women serve as health education communicators, using media and storytelling to raise awareness among children and spouses, and empowering children to reinforce anti-smoking messages. These roles reflect women’s growing agency and strategic efforts to safeguard family health.
Figure 2 illustrates the proportions of the most dominant roles played by women in supporting smoking cessation within their families. The chart reveals that 42% of the women acted as social control agents, emphasizing their responsibility to monitor and influence smoking behaviors among family members. Meanwhile, 33% served as family health protectors, focusing on maintaining a healthy, smoke-free environment at home. The remaining 25% took on the role of health education communicators, actively disseminating information and raising awareness about the dangers of smoking. This distribution reflects the multifaceted involvement of women in family health management, particularly in tobacco control. Their roles extend beyond traditional caregiving; they embody moral authority, provide behavioral guidance, and offer educational outreach. These findings highlight the strategic and culturally embedded role of women as health advocates within the household, especially in the Acehnese context.
3.3.2. Influence of Predisposing Factors on Women’s Involvement
Table 5 outlines how predisposing factors influence women’s active participation in protecting their families from smoking exposure. The process begins with an awareness of the dangers of secondhand smoke, often gained through health education or community counseling. This newfound knowledge prompts a sense of personal concern, especially regarding the health of their children. As awareness deepens, women experience a stronger motivation to act, such as asking their husbands to avoid smoking around children. This leads to a growing sense of responsibility, where women perceive themselves as primary guardians of family health and feel morally obligated to intervene. These predisposing factors foster a transformation in women’s roles from passive household caretakers to proactive health advocates within the home.
Figure 3 illustrates the distribution of female participants based on their level of knowledge about the health risks associated with smoking. Among the 75 women interviewed, 35 demonstrated a high level of knowledge, 25 had moderate knowledge, and 15 showed a low level of knowledge. While this bar chart presents only a descriptive overview and does not imply a causal relationship, qualitative interviews revealed that participants with higher levels of knowledge tended to be more actively involved in supporting smoking cessation efforts within the household. This finding highlights the potential influence of health literacy on women’s roles as health advocates. The narratives suggest that improved understanding of smoking-related dangers empowers women to initiate persuasive communication, establish smoke-free zones, and engage family members in dialogue about the harms of tobacco. Therefore, while the chart does not statistically confirm causation, it visually supports the qualitative insight that enhanced awareness is often accompanied by increased motivation and engagement in promoting a healthier domestic environment.
3.3.3. Supportive Enabling Conditions Facilitating Women’s Actions
Table 6 highlights that various enabling conditions significantly strengthen women’s involvement in promoting smoke-free households. Social support from family members and fellow women provides psychological encouragement to take action. Community-level campaigns and meetings enhance collective awareness and solidarity. Additionally, support from health institutions and the availability of educational materials help women translate knowledge into concrete actions. Environmental backing and moral messages from religious leaders further legitimize women’s roles as health advocates. Altogether, these factors create a supportive environment that empowers women to serve as active agents of change within their households.
3.3.4. Reinforcing Support from Community and Religious Institutions
Table 7 reports reinforcing support from the community and religious institutions. Support from both the community and religious institutions plays a crucial role in strengthening women’s involvement in creating smoke-free households. At the community level, encouragement from village leaders and the integration of smoking-related issues into public health activities help establish strong social legitimacy for women to take action. Collective efforts, such as the installation of banners and public campaigns, further contribute to raising collective awareness. Meanwhile, religious institutions offer profound moral reinforcement. Messages from religious leaders emphasizing that smoking harms the family serve as powerful ethical justifications for women to advocate for change. Additionally, religious gatherings such as sermons and Friday prayers function as platforms for health advocacy, positioning mosques as centers for public education. This combination of social and spiritual reinforcement empowers women with greater confidence and motivation to take on their roles as guardians of family health.
3.3.5. Perceived Impact on Smoking Behavior within the Household
Table 8 highlights the tangible impact of women’s advocacy on smoking behaviors within households. Many participants observed a reduction in smoking frequency, often shifting the activity outdoors or away from children, while others successfully established smoke-free zones at home through rules and symbolic reminders. Several women reported that their husbands showed signs of cessation progress, with gradual reductions in daily cigarette use, and in some cases, achieving complete cessation. Beyond behavioral outcomes, the findings also underscore the perceived self-efficacy of women. Witnessing change reinforced their belief that their actions mattered, boosting confidence to continue advocating for health within their families and communities. Together, these outcomes illustrate both practical behavioral changes and the empowerment of women as effective agents in promoting smoke-free households.
The pie chart in Figure 4 presents the distribution of perceived changes in smoking behavior among household members, as reported by the participants. A total of 42.7% of women observed a reduction in smoking frequency, 29.3% reported complete cessation, and 28% created smoke-free zones within their homes. These findings demonstrate how women’s sustained advocacy efforts, through emotional appeals, persistent reminders, and health communication, lead to fundamental behavioral changes within the household. The highest proportion of responses indicating reduced smoking frequency suggests a gradual shift in family habits influenced by consistent interpersonal engagement. The observation of nearly a third of participants experiencing complete cessation highlights the effectiveness of culturally and religiously grounded persuasion. Meanwhile, the establishment of smoke-free areas in domestic settings demonstrates increased awareness and respect for the health of others, particularly children and elderly family members. Collectively, these outcomes underscore the pivotal role women play in fostering a healthier home environment and demonstrate their capacity to drive meaningful change through advocacy, communication, and the support of enabling social conditions.
3.3.6. Challenges and Adaptive Strategies in Influencing Behavior
Table 9 reveals the barriers women encounter when advocating for smoke-free households, as well as the adaptive strategies they employ to overcome them. Many participants face gender-based resistance, where their efforts are dismissed due to patriarchal attitudes that minimize women’s authority. Cultural norms often frame smoking as a masculine right, making it difficult to challenge male behavior. Additionally, communication barriers, such as avoidance or dismissal during discussions, further complicate their efforts to advocate. Despite these challenges, women demonstrate resilience and creativity. They use emotional and child-centered appeals, highlighting the impact of smoke on their children’s health to evoke empathy. Others opt for indirect storytelling, using examples of neighbors or relatives to convey the dangers of smoking subtly. Some women strategically involve third-party influencers, such as religious leaders, to reinforce their message with social and moral authority. These adaptive approaches illustrate women’s agency in navigating complex household dynamics to protect their families’ health.
3.3.7. Transformation of Gender Role Perception
Table 10 highlights a significant shift in women’s perceptions of their roles within the household, particularly regarding smoking behavior control. Women have begun to exhibit greater self-confidence and awareness of their personal agency (Emerging Empowerment), challenge longstanding patriarchal norms that have previously silenced their voices (Challenging Traditional Roles), and expand their roles as protectors of family health and role models for other women (Role Expansion). This transformation reflects a movement toward more active female engagement as change agents in fostering a healthier and more equitable home environment.
Interview results revealed varying levels of smoking behavior change among husbands. Most participants reported a reduction in smoking frequency or relocation of smoking activities to outdoor areas. At the same time, a smaller number indicated that their husbands had entirely quit smoking, ranging from 6 months to over a year. These findings highlight a continuum of behavioral change rather than a uniform cessation pattern.
Figure 5 illustrates the evolving perception of gender roles among women participants, particularly in relation to their involvement in family health decisions. A majority of respondents (60%) reported increased confidence in their role as health advocates, signaling a significant shift in self-perception and agency within their households. These women now view themselves not only as caregivers, but also as key actors in shaping family health behaviors, especially in promoting smoke-free environments. Meanwhile, 25% of participants expressed that they now share an equal role in health-related decision-making with their husbands, indicating progress toward gender parity in household leadership. This suggests that health advocacy can be a powerful entry point for negotiating shared authority in domestic matters. Only 15% of respondents noted no significant change in their perceived roles, which may reflect persistent barriers such as strong patriarchal norms, lack of support, or limited exposure to health education.
4. Discussion
The discussion in this study centers on the transformative role of women as key agents in promoting tobacco control within the household setting, drawing on qualitative insights from Aceh, Indonesia. In a region deeply rooted in cultural and religious values, women were found to actively shape smoke-free environments through advocacy, emotional communication, and social persuasion. Their actions reflect a dynamic interplay between gender, health literacy, and community norms, where empowerment serves as both a catalyst and a product of health interventions at the family level. By examining how women negotiate influence within traditionally male-dominated households, this study situates their contributions within broader efforts to promote public health equity and behavioral change in low-resource, culturally embedded contexts.
Notably, the smoking status of husbands in this study was reported through the narratives of their wives, based on everyday observations within the household. No objective verification methods, such as clinical assessments or direct observation, were employed. This approach is consistent with the study’s qualitative aim to capture lived experiences and perceived realities, rather than to quantify smoking behavior. Rather than a limitation, the subjective nature of this data reflects the central focus on understanding how women interpret, respond to, and act upon smoking within their domestic environments.
Building on this, the study explicitly highlights the role of women as agents of change in household-level tobacco control. Interview findings revealed that women were not merely passive recipients of secondhand smoke exposure, but actively contributed to shaping smoke-free home environments through emotional communication, social persuasion, and health advocacy. These narratives highlight the importance of empowering women in household health decision-making and demonstrate how agency is exercised through relational strategies and informal negotiation, thereby underscoring their central role in promoting healthier family practices.
Women play a central role as agents of change in promoting family health, particularly in reducing exposure to tobacco smoke within the household. Through emotional appeals, interpersonal communication, and role modeling, they actively educate family members and establish rules to create a smoke-free home environment. Previous studies have shown that women often serve as key drivers of health promotion due to their moral and emotional roles as mothers and wives [34]. Therefore, empowering women through enhanced health literacy and social support is crucial for strengthening their impact on behavioral change toward a healthier family lifestyle.
Knowledge and attitudes serve as key predisposing factors influencing women’s participation in advocating for smoke-free environments. The higher their understanding of the health risks associated with smoking, particularly secondhand smoke, the more proactive and confident they become in initiating behavioral change within the household. This correlation is supported by previous research, which highlights that increased health literacy significantly enhances women’s engagement in health-promoting behaviors [35]. Thus, educational interventions that improve women’s awareness are essential to fostering their role as effective advocates for smoking cessation in family settings.
Enabling conditions such as access to health information, prior involvement in education campaigns, and exposure to community outreach programs significantly enhance women’s capacity and motivation to advocate for smoke-free households. These factors not only equip women with the necessary knowledge but also build their confidence and communication skills, enabling them to influence family behavior. Studies have shown that environments with supportive health infrastructure and regular public health messaging empower women to take active roles in shaping household norms and protecting family well-being [36]. Such conditions are, therefore, essential in translating awareness into concrete advocacy actions.
Social and religious legitimacy play a crucial role in strengthening women’s ability to take assertive action in promoting health within the family, particularly regarding smoking behavior. Support from spiritual leaders, customary laws, and prevailing community norms provides women with moral and social justification to speak out and influence change. This legitimacy not only protects them from social resistance but also amplifies their authority in traditionally patriarchal contexts. Prior research emphasizes that religious and cultural endorsement can significantly boost women’s participation in public health advocacy, turning personal concern into socially recognized action [37].
Women in the study reported tangible changes in household smoking behaviors as a result of their advocacy efforts. These changes included a reduction in smoking frequency, the establishment of designated smoke-free zones, and, in some cases, complete cessation, particularly among their spouses. Such transformations were attributed to a combination of persistent communication, emotional appeals, health education, and social reinforcement. These findings underscore the influential role women play in shaping healthier domestic environments, aligning with previous studies that highlight the effectiveness of female-led health interventions within families [38].
Women employed adaptive strategies to overcome social and patriarchal barriers when promoting smoke-free behaviors within the household. Faced with resistance from their husbands or constrained by traditional gender norms, they resorted to indirect yet effective methods, such as initiating informal discussions, expressing emotional concerns related to family health, and involving influential third parties, like religious leaders or children. These approaches reflect their ability to navigate complex power dynamics while maintaining cultural harmony. Previous studies have similarly noted that women often rely on relational communication and community figures to assert influence in health matters within patriarchal settings [39].
Women’s involvement in health advocacy represents a significant transformation in gender roles, shifting from traditional domestic responsibilities to emerging leadership roles in the family and community health domain. This transition is characterized by increased confidence, assertiveness, and influence in shaping health-related decisions, particularly regarding smoking behaviors. Rather than being confined to caregiving tasks, women are now seen and see themselves as proactive health agents. This role expansion aligns with broader patterns of gender empowerment observed in health promotion literature, where women’s participation in public health efforts is linked to both individual agency and structural support [40]. Such a shift not only enhances family well-being but also contributes to long-term gender equity in decision-making spheres.
The role of emotion and interpersonal communication emerges as a crucial strategy in women’s advocacy for healthier family environments. By employing messages grounded in affection, empathy, and concern, particularly for children’s well-being, women can persuade family members to reduce or quit smoking effectively. Emotional appeals resonate more deeply within familial relationships, fostering a sense of guilt or responsibility in smokers. For instance, reminders framed around the health risks to children or expressions of maternal concern tend to generate more receptive responses. These communication styles, rooted in empathy and relational bonds, have been identified in previous studies as practical tools for initiating behavior change within domestic settings [41]. Thus, emotional and empathetic communication strengthens women’s influence and reinforces their role as trusted advocates in the household.
Community-based and gender-sensitive health education programs have shown a significant impact in empowering women as key agents of change in promoting healthy behaviors within families. When women are actively involved as participants, facilitators, or peer educators, these programs become more relatable and culturally aligned, increasing their acceptance and sustainability. Research has demonstrated that such gender-inclusive approaches enhance the credibility of health messages and improve adherence to behavior change, especially in patriarchal communities where women’s voices may otherwise be marginalized [42]. By integrating women’s lived experiences and leadership roles into health interventions, these programs not only address immediate issues, such as tobacco exposure, but also contribute to long-term shifts in gender norms and family health decision-making dynamics.
This study contributes to the development of gender and health literacy in local communities by emphasizing the importance of culturally grounded, gender-responsive approaches in public health interventions. By recognizing women not merely as passive recipients but as active health advocates shaped by local norms and values, the research highlights how gender-sensitive frameworks rooted in community identity can enhance the relevance and effectiveness of health programs. The integration of local wisdom, religious teachings, and familial structures into advocacy strategies fosters trust and engagement, ultimately leading to more sustainable behavioral changes [43]. These findings align with global recommendations that stress the intersection of gender equity and health education in achieving community health resilience [44]
5. Conclusions
Based on the findings, this study concludes that women play a central role as agents of change in controlling smoking behavior at the household level in Aceh, Indonesia. They actively take on roles as social regulators, health communicators, and family protectors through empathetic interpersonal approaches, knowledge of smoking hazards, and the social and religious legitimacy they receive. Predisposing factors such as awareness levels, enabling conditions such as access to health information and prior educational experiences, and support from social institutions, including religious leaders and community norms—further strengthen their capacity to act.
Tangible behavioral changes, such as reduced smoking frequency, the establishment of smoke-free zones, and even complete cessation among spouses, demonstrate the effectiveness of women’s advocacy efforts. Despite facing social barriers and patriarchal norms, women developed adaptive strategies, including informal discussions, emotional appeals, and the involvement of third parties (e.g., religious leaders or children). This also reflects a transformation in gender roles from traditional domestic roles to leadership in family health matters. The study highlights that empowering women through health literacy and community support significantly contributes to creating smoke-free home environments and fostering healthier family behavior.
Author Contributions
Conceptualization, H.S., M.M., and D.S.; methodology, H.S., M.M., and D.S.; software, H.S.; validation, H.S., M.M., and D.S.; formal analysis, H.S.; investigation, H.S., M.M., and D.S.; resources, H.S., M.M., and D.S.; data curation, H.S., M.M., R.I and D.S.; writing—original draft preparation, H.S., M.M., and D.S.; writing—review and editing, H.S., M.M., D.S., and R.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data supporting this study are not publicly available due to ethical restrictions.
Acknowledgments
The authors would like to thank the lecturers, curriculum developers, and policy stakeholders who participated in this study, as well as the institutional representatives who facilitated the research process.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Lu, W.; Aarsand, R.; Schotte, K.; Han, J.; Lebedeva, E.; Tsoy, E.; Maglakelidze, N.; Soriano, J.B.; Bill, W.; Halpin, D.M. Tobacco and COPD: presenting the World Health Organization (WHO) tobacco knowledge summary. Respiratory Research 2024, 25, 338. [Google Scholar] [CrossRef]
- Lee, J.-w.; Yang, W.; Kim, Y.-S.; Kim, Y.; Yoo, H.-S.; Kang, H.-T. Exposure to secondhand smoke and a tobacco-specific carcinogen in non-smokers. Korean Journal of Family Medicine 2022, 43, 117. [Google Scholar] [CrossRef]
- Bafunno, D.; Catino, A.; Lamorgese, V.; Del Bene, G.; Longo, V.; Montrone, M.; Pesola, F.; Pizzutilo, P.; Cassiano, S.; Mastrandrea, A. Impact of tobacco control interventions on smoking initiation, cessation, and prevalence: a systematic review. Journal of Thoracic Disease 2020, 12, 3844. [Google Scholar] [CrossRef]
- Dai, X.; Ng, M.; Gil, G.F.; Morgan, B.W.; Anderson, J.A.; Adnani, Q.E.S.; Aji, B.; Aljunid, S.M.; Amul, G.G.H.; Anwar, S.L. The epidemiology and burden of smoking in countries of the Association of Southeast Asian Nations (ASEAN), 1990–2021: findings from the Global Burden of Disease Study 2021. The Lancet Public Health 2025, 10, e442–e455. [Google Scholar] [CrossRef]
- Sufri, S.; Nurhasanah, N.; Ahsan, A.; Saputra, I.; Jannah, M.; Yeni, C.M.; Mardhiah, A.; Bakri, S.; Usman, S. Barriers and opportunities for improving smoke-free area implementation in Banda Aceh city, Indonesia: a qualitative study. BMJ open 2023, 13, e072312. [Google Scholar] [CrossRef]
- Dono, J.; Miller, C.; Ettridge, K.; Wilson, C. The role of social norms in the relationship between anti-smoking advertising campaigns and smoking cessation: a scoping review. Health education research 2020, 35, 179–194. [Google Scholar] [CrossRef] [PubMed]
- Bird, Y.; Kashaniamin, L.; Nwankwo, C.; Moraros, J. Impact and effectiveness of legislative smoking bans and anti-tobacco media campaigns in reducing smoking among women in the US: a systematic review and meta-analysis. In Proceedings of the Healthcare; 2020; p. 20. [Google Scholar]
- César-Santos, B.; Bastos, F.; Dias, A.; Campos, M.J. Family nursing care during the transition to parenthood: a scoping review. In Proceedings of the Healthcare; 2024; p. 515. [Google Scholar]
- Ahmad, N.; Zamri, Z.H.; Omarali, N.S. Islamic nations’ approaches to combating gender discrimination against women: An examination of the southeast Asia region. De Jure: Jurnal Hukum dan Syar’iah 2024, 16, 501–530. [Google Scholar]
- Jafari, A.; Mahdizadeh, M.; Peyman, N.; Gholian-Aval, M.; Tehrani, H. Exploration the role of social, cultural and environmental factors in tendency of female adolescents to smoking based on the qualitative content analysis. BMC Women’s Health 2022, 22, 38. [Google Scholar] [CrossRef]
- Martinez Leal, I.; Taing, M.; Correa-Fernández, V.; Obasi, E.M.; Kyburz, B.; Le, K.; Koshy, L.; Chen, T.A.; Williams, T.; Casey, K. Addressing smoking cessation among women in substance use treatment: A qualitative approach to guiding tailored interventions. International Journal of Environmental Research and Public Health 2021, 18, 5764. [Google Scholar] [CrossRef] [PubMed]
- He, H.; Pan, Z.; Wu, J.; Hu, C.; Bai, L.; Lyu, J. Health effects of tobacco at the global, regional, and national levels: results from the 2019 global burden of disease study. Nicotine and Tobacco Research 2022, 24, 864–870. [Google Scholar] [CrossRef]
- Yang, L.; Wu, H.; Zhao, M.; Magnussen, C.G.; Xi, B. Prevalence and trends in tobacco use, secondhand smoke exposure at home and household solid fuel use among women in 57 low-and middle-income countries, 2000–2018. Environment International 2022, 161, 107142. [Google Scholar] [CrossRef] [PubMed]
- Ninkron, P.; Nakamadee, B.; Mahamit, W.; Suesuwan, W.; Sukkul, K. Multi-sector Development of Measures and Interventions to Prevent New Smokers Among Youths Living in Underprivileged Housing Projects in Thailand. Journal of Prevention 2024, 45, 521–543. [Google Scholar] [CrossRef]
- Esan, O.M. The Implementation of an Evidence-Based Smoke Cessation Program to Decrease the Incidence of Smoking Among Adult Smokers. Aspen University, 2024.
- Yoosefi Lebni, J.; Mohammadi Gharehghani, M.A.; Soofizad, G.; Khosravi, B.; Ziapour, A.; Irandoost, S.F. Challenges and opportunities confronting female-headed households in Iran: a qualitative study. BMC women’s health 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Lopes Cardozo, M.T.; Srimulyani, E. Analysing the spectrum of female education leaders’ agency in Islamic boarding schools in post-conflict Aceh, Indonesia. Gender and Education 2021, 33, 847–863. [Google Scholar] [CrossRef]
- Lyall, V.; Guy, J.; Egert, S.; Pokino, L.-A.; Rogers, L.; Askew, D. “They were willing to work with me and not pressure me”: a qualitative investigation into the features of value of a smoking cessation in pregnancy program for aboriginal and torres strait islander women. International journal of environmental research and public health 2021, 18, 49. [Google Scholar] [CrossRef]
- Rosemary, R. Women’s interpretation of anti-smoking messages in Indonesia: An audience analysis. 2020.
- Kandula, N.R.; Patel, K.M.; Lancki, N.; Welch, S.; Bouris, A.; Marquez, D.X.; Liem, R.; Rastogi, M.; Roy, R.; Bharucha, H. South Asians Active Together (SAATH): Protocol for a multilevel physical activity intervention trial for South Asian American mother and daughter dyads. Contemporary clinical trials 2022, 120, 106892. [Google Scholar] [CrossRef]
- Sim, I.; Hwang, E.; Sin, B. A self-reflection program for smoking cessation in adolescents: a phenomenological study. International Journal of Environmental Research and Public Health 2020, 17, 1085. [Google Scholar] [CrossRef] [PubMed]
- Ho, Y.-C.L.; Mahirah, D.; Ho, C.Z.-H.; Thumboo, J. The role of the family in health promotion: a scoping review of models and mechanisms. Health promotion international 2022, 37, daac119. [Google Scholar] [CrossRef]
- Li, L.; Wang, J.; Xia, W.; Li, W.H.; Weng, X.; Song, P. Smoking cessation and relapse-prevention interventions tailored for expectant and new fathers: protocol of a systematic review and network meta-analysis. BMJ open 2023, 13, e071745. [Google Scholar] [CrossRef] [PubMed]
- Esquenazi-Karonika, S. PLANNING MODELS FOR THEORY-BASED HEALTH PROMOTION INTERVENTIONS. Health Behavior: Theory, Research, and Practice.
- He, Y.-Y.; Huang, W.-H.; Tung, C.-Y. A cross-sectional study applying the PRECEDE model to explore factors influencing epidemic prevention behaviors among preschool educators. BMC Public Health 2024, 24, 3486. [Google Scholar] [CrossRef]
- Fakha, A.; Groenvynck, L.; de Boer, B.; van Achterberg, T.; Hamers, J.; Verbeek, H. A myriad of factors influencing the implementation of transitional care innovations: a scoping review. Implementation science 2021, 16, 1–24. [Google Scholar] [CrossRef]
- Xie, Y.J.; Tian, L.; Deng, Y.; Yang, L.; Cheung, K.; Li, Y.; Wang, H.H.; Hao, C.; Siu, G.K.H.; Zhang, Q.; et al. Use of the PRECEDE-PROCEED Model in Piloting Vaccine Promotion and Infection Self-Protection: Intervention Development and Effectiveness Examination. Vaccines (Basel) 2024, 12. [Google Scholar] [CrossRef]
- De Oliveira, B. Participatory action research as a research approach: Advantages, limitations and criticisms. Qualitative Research Journal 2023, 23, 287–297. [Google Scholar] [CrossRef]
- Skipper, Y.; Pepler, D.J. Knowledge mobilization: Stepping into interdependent and relational space using co-creation. Action Research 2021, 19, 588–605. [Google Scholar] [CrossRef]
- Mabetha, D.; Ojewola, T.; Van Der Merwe, M.; Mabika, R.; Goosen, G.; Sigudla, J.; Hove, J.; Witter, S.; D’Ambruoso, L.; Platform, O.b.i.c.t.V.A.w.P.A.R.W.M.D.o.H.L. Realising radical potential: building community power in primary health care through Participatory Action Research. International Journal for Equity in Health 2023, 22, 94. [Google Scholar] [CrossRef] [PubMed]
- Trisnowati, H.; Ismail, D.; Padmawati, R.S.; Utarini, A. Developing a framework for youth empowerment to prevent smoking behavior in a rural setting: study protocol for a participatory action research. Health Education 2021, 121, 30–47. [Google Scholar] [CrossRef]
- Vijayaraghavan, M.; Hartman-Filson, M.; Vyas, P.; Katyal, T.; Nguyen, T.; Handley, M.A. Multi-level influences of smoke-free policies in subsidized housing: applying the COM-B model and neighborhood assessments to inform smoke-free policies. Health Promotion Practice 2025, 26, 142–157. [Google Scholar] [CrossRef]
- Suprapto, N.; Sunarti, T.; Wulandari, D.; Hidayaatullaah, H.N.; Adam, A.S.; Mubarok, H. A systematic review of photovoice as participatory action research strategies. International Journal of Evaluation and Research in Education 2020, 9, 675–683. [Google Scholar] [CrossRef]
- Estebsari, F.; Kandi, Z.R.K.; Bahabadi, F.J.; Filabadi, Z.R.; Estebsari, K.; Mostafaei, D. Health-related quality of life and related factors among pregnant women. Journal of Education and Health Promotion 2020, 9, 299. [Google Scholar] [CrossRef]
- Ghorbani-Dehbalaei, M.; Loripoor, M.; Nasirzadeh, M. The role of health beliefs and health literacy in women’s health promoting behaviours based on the health belief model: a descriptive study. BMC women’s health 2021, 21, 421. [Google Scholar] [CrossRef] [PubMed]
- Karp, C.; Wood, S.N.; Galadanci, H.; Kibira, S.P.S.; Makumbi, F.; Omoluabi, E.; Shiferaw, S.; Seme, A.; Tsui, A.; Moreau, C. ‘I am the master key that opens and locks’: Presentation and application of a conceptual framework for women’s and girls’ empowerment in reproductive health. Social Science & Medicine 2020, 258, 113086. [Google Scholar]
- Zeinali, Z.; Muraya, K.; Molyneux, S.; Morgan, R. The use of intersectional analysis in assessing women’s leadership progress in the health workforce in LMICs: a review. International Journal of Health Policy and Management 2021, 11, 1262. [Google Scholar] [CrossRef]
- Mukherjee, S.; Kumar, A. Fostering Women’s Empowerment through Men’s Involvement in Family Planning Initiatives and Effective Strategies: A Systematic Review. Available at SSRN 4967810 2024. [Google Scholar]
- McBride, H.L.; Kwee, J.L. Inside and out: How western patriarchal cultural contexts shape women’s relationships with their bodies. International perspectives in values-based mental health practice: Case studies and commentaries.
- Diprose, R. Brokerage, power and gender equity: How empowerment-focused civil society organisations bolster women’s influence in rural Indonesia. Journal of International Development 2023, 35, 401–425. [Google Scholar] [CrossRef]
- Dong, C.; Morehouse, J. Toward a caring government: Advancing ethical government public relations with a care-based relationship cultivation model. Journal of Public Relations Research 2022, 34, 179–207. [Google Scholar] [CrossRef]
- Patel, P.; Meagher, K.; El Achi, N.; Ekzayez, A.; Sullivan, R.; Bowsher, G. “Having more women humanitarian leaders will help transform the humanitarian system”: challenges and opportunities for women leaders in conflict and humanitarian health. Conflict and health 2020, 14, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ridho, A.; Sa’ad, A. Reconstruction of Theological Narrative: Integration of Local Wisdom into Religious Practices for Social Cohesion in Multicultural Societies of Southeast Asia. Islam Transformatif: Journal of Islamic Studies 2024, 8, 220–242. [Google Scholar] [CrossRef]
- Eboagwu-ijah, P.I.; Abwami, I.M. Exploring Gender Dynamics in Climate Resilience and Health Promotion Initiatives: A Case Study of Rural Communities in Abuja, Nigeria. Policy Strategy 2024, 21, 159. [Google Scholar]
Figure 1.
A conceptual framework of the role of women in family health, encompassing predisposing, enabling, and reinforcing factors that contribute to the reduction of smoking behavior within the household environment.
Figure 1.
A conceptual framework of the role of women in family health, encompassing predisposing, enabling, and reinforcing factors that contribute to the reduction of smoking behavior within the household environment.
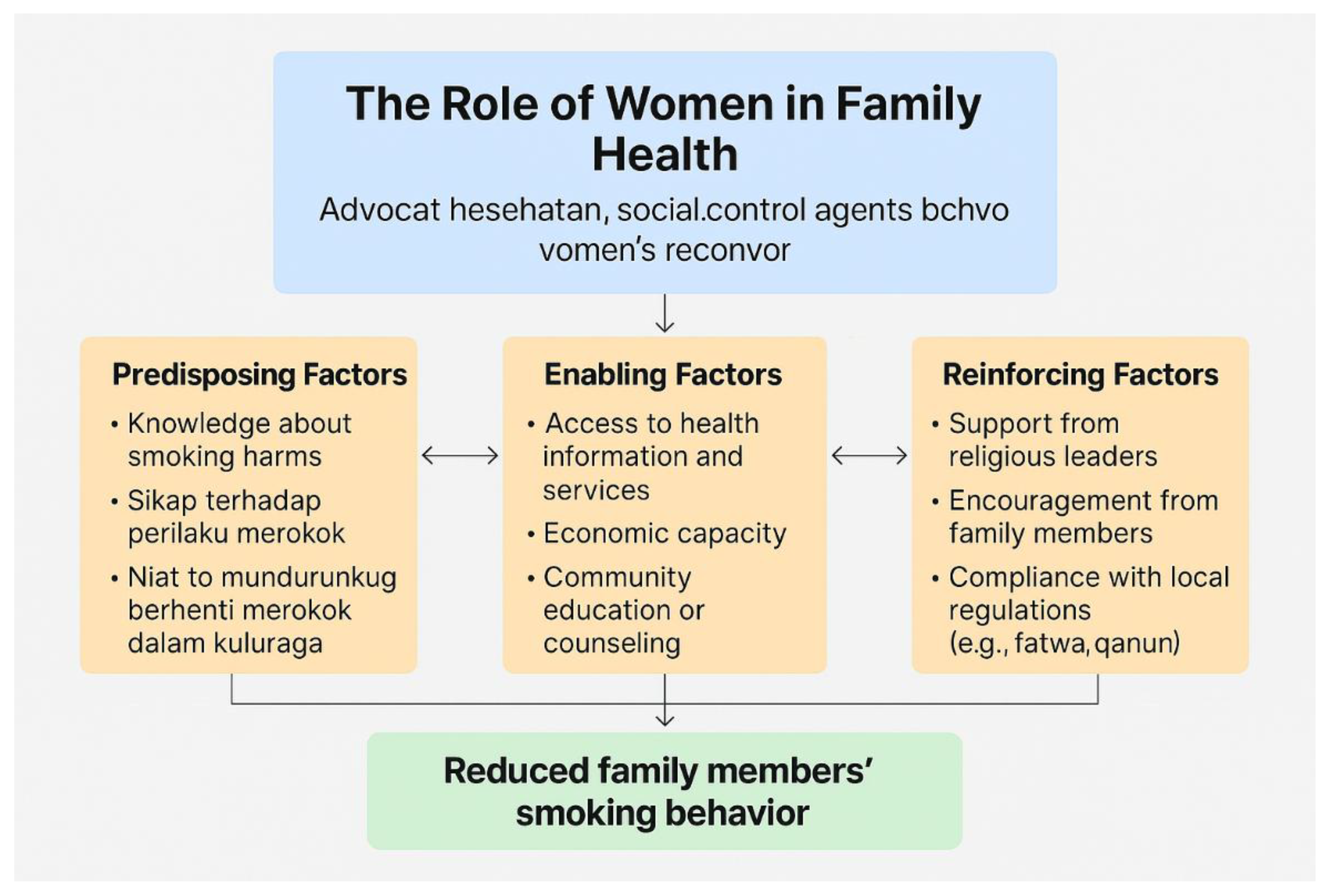
Figure 2.
Proportions of Dominant Roles Played by Women in Supporting Smoking Cessation in the Family.
Figure 2.
Proportions of Dominant Roles Played by Women in Supporting Smoking Cessation in the Family.
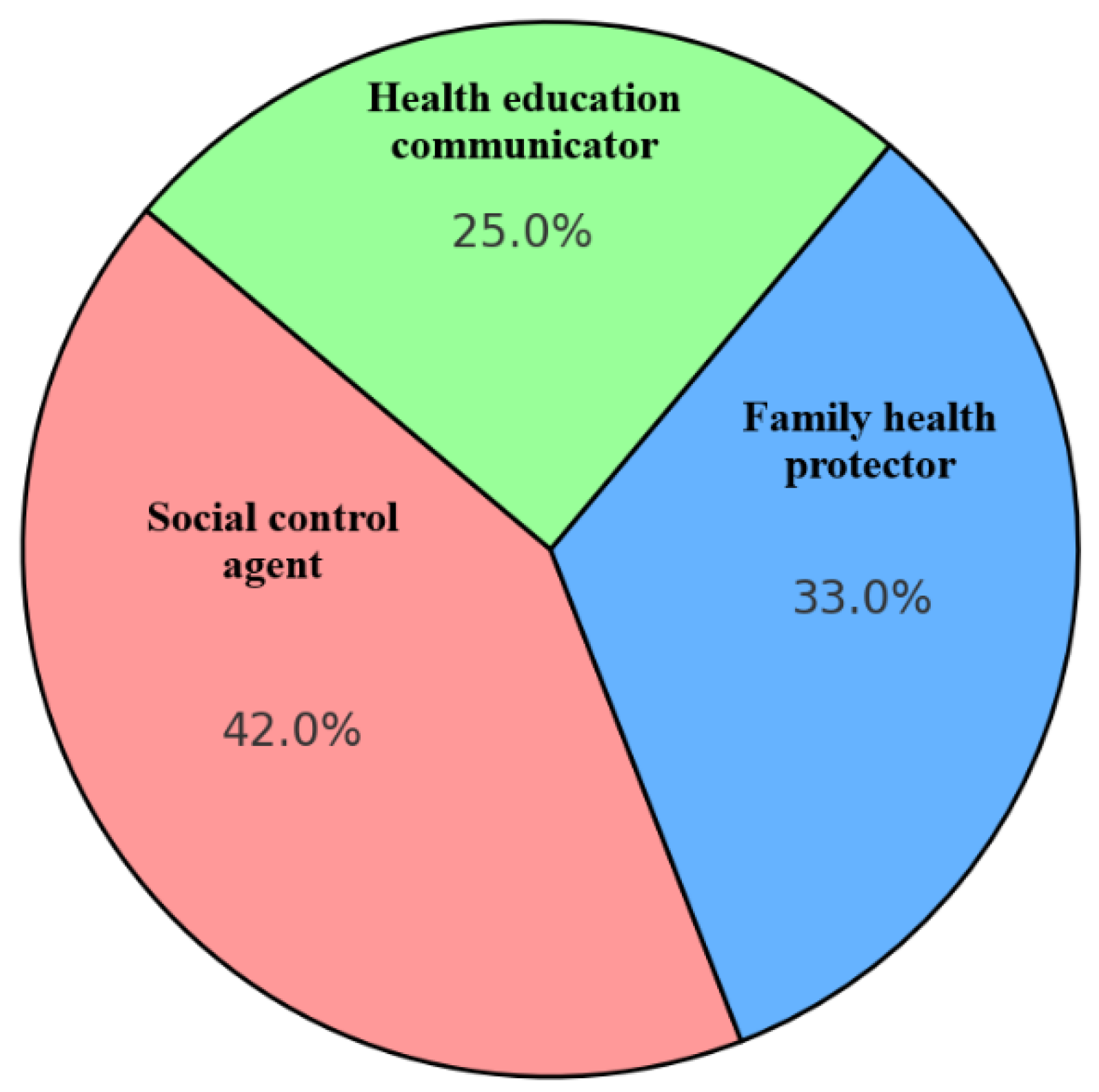
Figure 3.
Frequency of Participants by Knowledge Level on Smoking Risks.
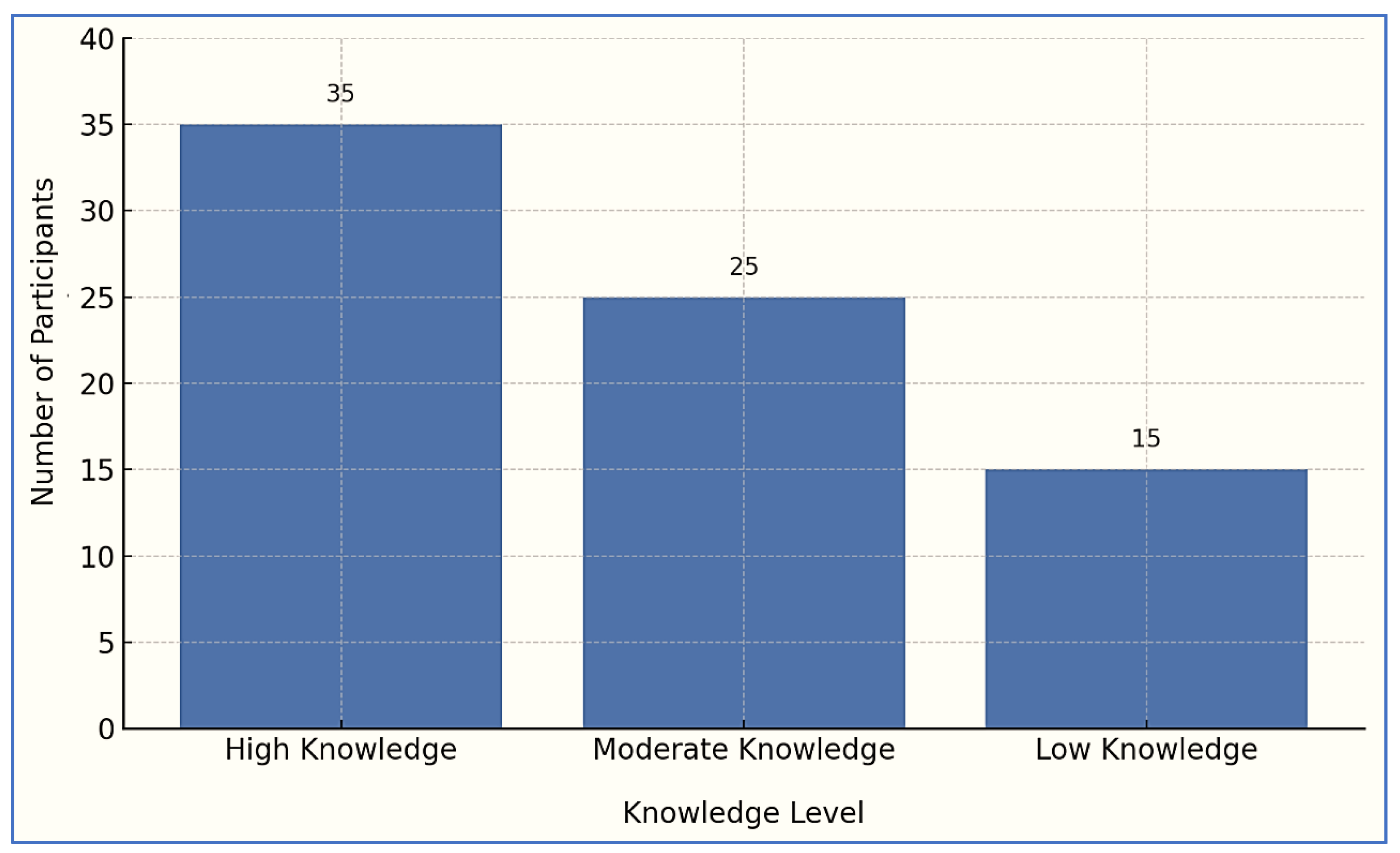
Figure 4.
The proportion of Reported Smoking Behavior Changes within the Household.
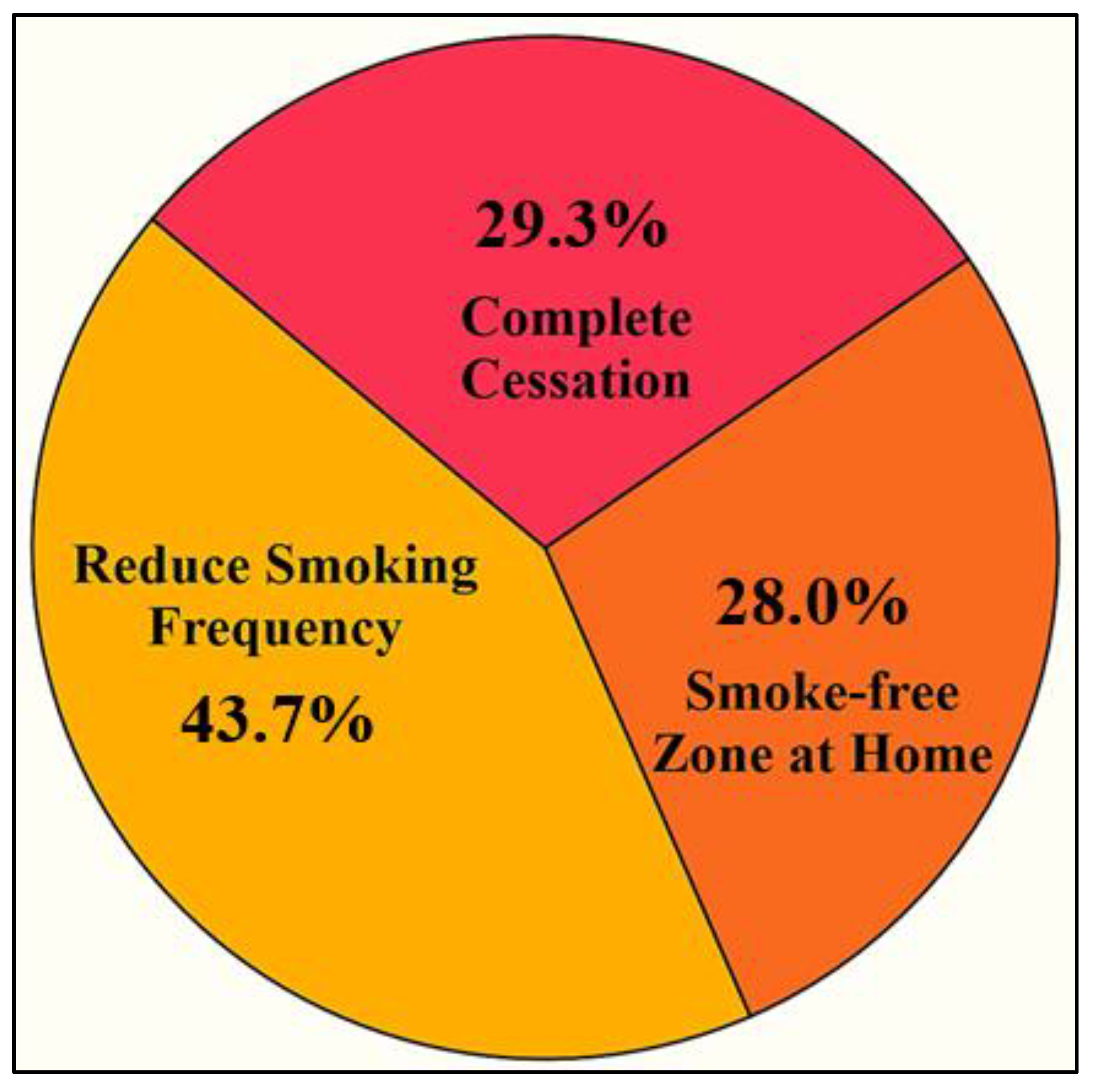
Figure 5.
Transformation of Gender Role Perception Among Women Participants.
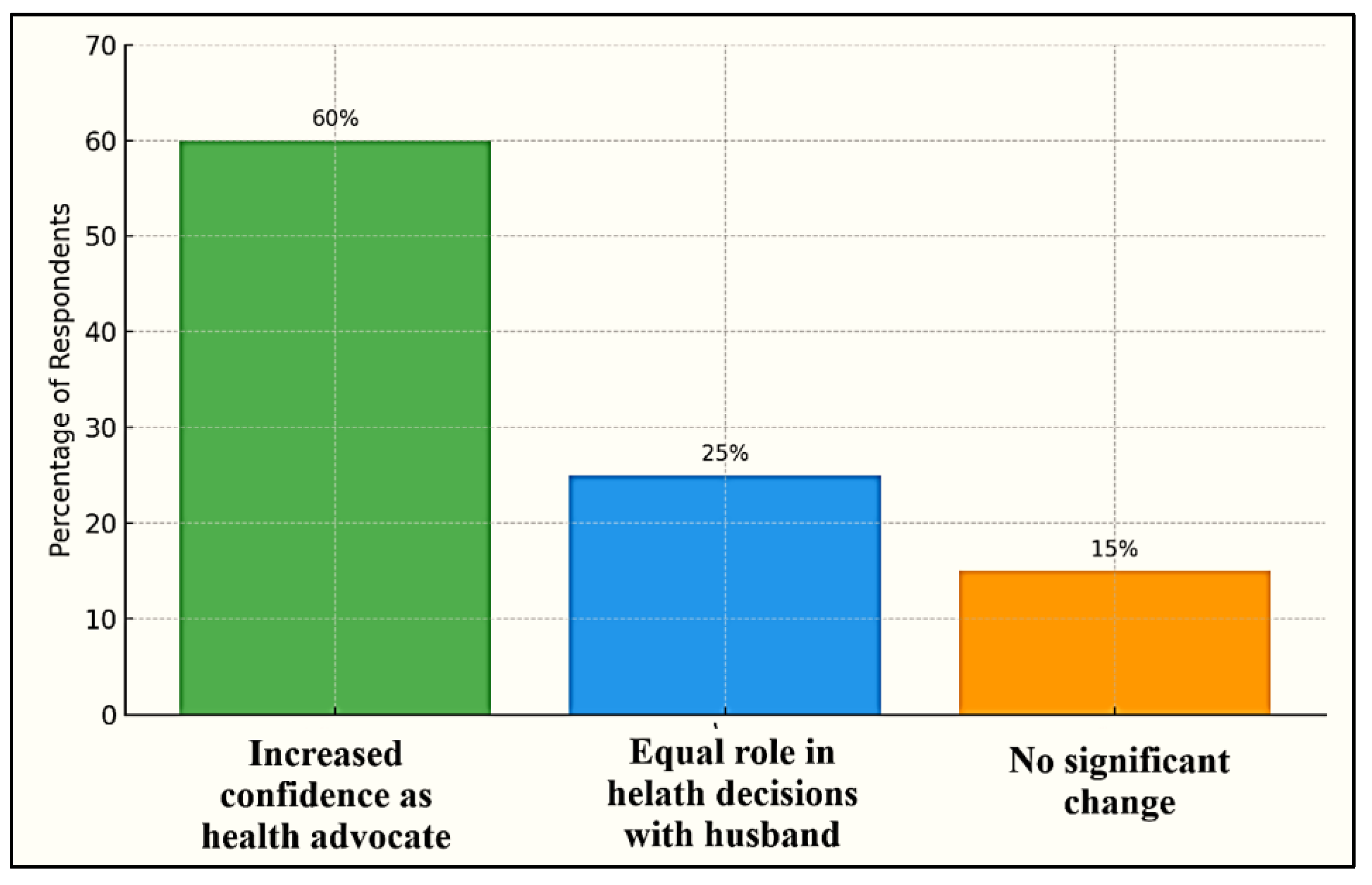

Table 1.
Characteristics of Study Participants.
| Variable | Category | N | Percentage (%) | Reason Required |
|---|---|---|---|---|
| District | Aceh Singkil | 20 | 26.7 | Represents diverse geographical and cultural settings in the Aceh Province |
| Gayo Lues | 30 | 40.0 | ||
| Pidie Jaya | 25 | 33.3 | ||
| Age Group | 18–29 years | 21 | 28.0 | Age influences maturity, experience, and responsibilities within the household. |
| 30–39 years | 27 | 36.0 | ||
| 40–50 years | 27 | 36.0 | ||
| Education Level | Primary school | 25 | 33.3 | Educational attainment affects health literacy, attitudes, and communication capacity. |
| Secondary school | 34 | 45.3 | ||
| Higher education | 16 | 21.3 | ||
| Employment Status | Housewife | 33 | 44.0 | Employment status reflects both economic capacity and social role, influencing household behavior. |
| Informal worker | 26 | 34.7 | ||
| Civil servant/teacher / etc. | 16 | 21.3 | ||
| Exposure to Health Education | Yes | 49 | 65.3 | Assesses the impact of public health campaigns or counseling on behavior awareness |
| No | 26 | 34.7 | ||
| Years Living in Community | < 5 years | 15 | 20.0 | The duration of residence influences community ties, access to information, and cultural adaptation. |
| 5–10 years | 30 | 40.0 | ||
| > 10 years | 30 | 40.0 | ||
| Religious Involvement | Active | 38 | 50.7 | Religious involvement affects value orientation, including perceptions of smoking. |
| Occasionally active | 26 | 34.7 | ||
| Not Active | 11 | 14.6 | ||
| Community Participation | Yes | 49 | 65.3 | Participation in social groups (e.g., health posts and religious gatherings) supports social control roles. |
| No | 26 | 34.7 | ||
| Family Smoker | Husband / former smoker | 75 | 100.0 | Central to the study: assessing women’s role in supporting smoking cessation in family settings |
Data Processing, 2025.
Table 2.
Trustworthiness of the Qualitative Data.
| Trustworthiness Aspect | Definition | Process | Findings | Application in This Study |
|---|---|---|---|---|
| Credibility | Confidence in the truth and authenticity of the data and research findings. | In-depth interviews conducted twice (verification & clarification) Triangulation across locations and participant backgrounds Member checking of interview results |
Consistent data and emerging thematic patterns across participants from different regions. | Achieved through prolonged engagement, regional triangulation, and participant data verification. |
| Transferability | The extent to which findings can be applied to other similar contexts. | Selection of regions with socioeconomic variation Detailed description of local context Comprehensive profiling of participant backgrounds |
The findings may apply to other areas with similar social conditions. | Ensured through rich contextual descriptions of three underprivileged districts in Aceh. |
| Dependability | Consistency of the research process and results over time. | Documentation of procedures Use of a consistent interview protocol Systematic storage of recordings and transcripts |
Findings are traceable to original data and show analysis stability. | Maintained through audit trails and consistent interview procedures across all research subjects. |
| Confirmability | The neutrality of the data: ensuring findings originate from participants, not researcher bias. | Reflective journaling Direct quotations from participants Cross-validation of codes and themes by research team |
The findings reflect the participants’ voices and perspectives without the researcher’s influence. | Upheld through researcher reflexivity, documentation, and the use of direct participant quotations. |
Data Processing, 2025.
Table 3.
Summary of Main Themes, Sub-Themes, and Representative Quotes from Participants.
| Main Themes | Sub-Themes | Descriptions | Illustrative Quotes |
|---|---|---|---|
| Women’s Role in Household Tobacco Control | Emotional Motivation | Concern about husband’s and children’s health; fear of disease | “I told him, if you love your kids, stop smoking.” (P-13, Aceh Singkil) |
| Domestic Negotiation | Dialogues, compromises, or conditions to restrict smoking | “I said, you can smoke outside, not in front of the kids.” (P-27, Pidie Jaya) | |
| Assertive Persuasion | Open confrontation or assertive language | “I was angry when he smoked near our baby. I threw the cigarette.” (P-45, Gayo Lues) | |
| Health Literacy and Information Seeking | Seeking Trusted Sources | Use of health workers, religious leaders, or TV programs | “I heard from the midwife that secondhand smoke is dangerous.” (P-31, Gayo Lues) |
| Misinformation or Lack of Access | Lack of proper knowledge or exposure to misleading info | “They say herbal cigarettes are safe, so he switched to those.” (P-8, Aceh Singkil) | |
| Cultural and Religious Framing | Religious Advice | Using Islamic teachings to discourage smoking | “I reminded him that harming health is against Islam.” (P-22, Pidie Jaya) |
| Gender Norms | Reinforcement of masculine decision-making | “It’s hard. He is the man of the house.” (P-60, Aceh Singkil) | |
| Community-Level Influence | Peer Pressure and Role Models | Observing neighbors/friends who quit smoking as examples | “He stopped because his brother stopped first.” (P-48, Gayo Lues) |
| Community Support and Sanctions | Community norms, bans, or support groups | “In our village, the mosque banned smoking near the entrance.” (P-19, Pidie Jaya) | |
| Participatory Empowerment | Reflective Learning | Women reflect on their own power and voice | “I never thought I could make him quit. But I did.” (P-7, Gayo Lues) |
| Aspirations for Advocacy | Hope to help others and become health agents | “I want to help other mothers do the same.” (P-33, Aceh Singkil) |
Data Processing, 2025.
Table 4.
Women’s Role as Health Advocates in the Family.
| Role | Description | Quote |
|---|---|---|
| Social Control Agent | Women implement unwritten rules to limit smoking indoors, especially near children, using persuasive, emotional, and religious-based approaches. | “If my husband wants to smoke, I tell him not to do it inside the house. I feel sorry for the children...” (P34), Aceh Singkil. |
| Family Health Protector | Women proactively create a smoke-free home environment by posting homemade signs, signaling their health priorities, and protecting their children. | “I put a paper sign saying ‘no smoking’ near the kitchen... our children’s health matters more.” (P11), Pidie Jaya |
| Health Education Communicator | Women use media (videos, stories, experiences) to educate both children and spouses about the harms of smoking, empowering children to remind fathers. | “I once had the children watch a video... So they’d be afraid and remind their father too.” (P07), Gayo Lues. |
Data Processing, 2025.
Table 5.
Influence of Predisposing Factors on Women’s Involvement.
| Theme | Sub-theme | Meaning/Insight | Quote |
|---|---|---|---|
| Influence of Predisposing Factors | Awareness of smoking risks | Knowledge gained from health education or community-based counseling triggers concern. | “I didn’t know how harmful secondhand smoke was until I heard it from the clinic.” – P05 |
| Personal health concern | Women begin to relate the risks of smoking to real dangers affecting their children. | “Now that I understand the risks, I feel I must protect my children.” – P19. | |
| Motivation to take action | Internal drive increases after understanding the consequences of smoking in the household | “After learning about the effects, I told my husband to stop smoking around the kids.” – P27 | |
| Perception of responsibility | Women perceive themselves as protectors of family health and feel compelled to act | “If not me, who else will warn him? I’m responsible for our children’s safety.” – P33 |
Data Processing, 2025.
Table 6.
Supportive Enabling Conditions Facilitating Women’s Actions.
| Theme | Sub-theme | Quote |
|---|---|---|
| Social Support | Support from family members | “My eldest child told his father not to smoke inside, that really helped.” – P09. |
| Encouragement from other women | “My neighbor also told her husband to stop smoking, so I followed her steps.” – P15. | |
| Community Support | Village leader’s campaign against smoking | “Our village head told us to create a smoke-free home.” – P12 |
| Community meetings raising awareness. | “We often discuss this in village women’s gatherings.” – P17. | |
| Institutional Encouragement | Support from local health institutions | “The health clinic staff encouraged me to talk to my husband.” – P20 |
| Access to Educational Resources | Availability of visual aids or pamphlets | “We got leaflets and stickers from the community meeting.” – P11 |
| Environmental Support | Clean air campaigns in the neighborhood | “The whole neighborhood is now trying to keep the air clean.” – P29 |
| Faith-based Encouragement | Religious messages supporting health | “Our imam once said that smoking harms the family, which touched many hearts.” – P18 |
Data Processing, 2025.
Table 7.
Reinforcing Support from Community and Religious Institutions.
| Theme | Sub-theme | Quote |
|---|---|---|
| Community Reinforcement | Public endorsement of anti-smoking behavior | “When the village chief supports no-smoking rules, everyone pays more attention.” – P10. |
| Integration in community health activities | “We included smoking discussions during health events in the village.” – P23. | |
| Visibility of collective actions | “We put up banners about smoke-free homes around the neighborhood.” – P06. | |
| Religious Reinforcement | Religious leaders promoting health values | “Our imam said smoking is harmful, and as Muslims we should avoid harming others.” – P16. |
| Alignment with religious morals | “It’s easier to advise my husband when I remind him of what the ustadz said at the mosque.” – P28. | |
| Religious gatherings as platforms for advocacy | “We often hear health messages during Friday prayers.” – P30. |
Data Processing, 2025.
Table 8.
Perceived Impact on Smoking Behavior.
| Theme | Sub-theme | Quote |
|---|---|---|
| Behavioral Change in Household | Reduced frequency of smoking | “He still smokes, but now only outside the house—not around the children anymore.” – P12 |
| Smoke-free zones created at home | “I put up a no-smoking sign in our living room, and he respects it now.” – P28. | |
| Cessation Progress | Gradual reduction leading to quitting | “He used to smoke five times a day, now maybe once, sometimes not at all.” – P39. |
| Complete cessation achieved | “He hasn’t touched a cigarette in six months since I talked to him seriously.” – P41. | |
| Perceived Self-Efficacy of Women | The belief that action makes a difference | “I didn’t think he’d listen, but now I believe I can influence change.” – P07. |
| Increased confidence in advocacy role | “Seeing him stop gave me the confidence to keep reminding others too.” – P24 |
Data Processing, 2025.
Table 9.
Challenges and Adaptive Strategies in Influencing Smoking Behavior Within the Household.
| Theme | Sub-theme | Quote |
|---|---|---|
| Challenges in Advocacy | Gender-based resistance | “He told me I’m just a woman, I shouldn’t be telling him what to do.” – P34. |
| Cultural and patriarchal norms | “In our culture, men think smoking is their right. It’s hard to change that.” – P22. | |
| Communication barriers | “He just walks away when I bring up the topic of smoking.” – P18. | |
| Adaptive Strategies | Emotional and child-centered appeal | “I waited until he was calm. Then I told him how our child coughs whenever he smokes inside.” – P41 |
| Indirect discussion and storytelling | “I didn’t argue. I shared a story about a neighbor’s husband who got sick from smoking.” – P07. | |
| Involving third-party influencers | “When the imam mentioned it during the sermon, he started to feel embarrassed.” – P53. |
Data Processing, 2025.
Table 10.
Transformation of Gender Role Perception.
| Theme | Sub-theme | Quote |
|---|---|---|
| Emerging Empowerment | Increased confidence in decision-making | “I used just to follow what he said, but now I speak up for our children.” – P25. |
| Recognition of personal agency | “I realized I could change things at home, even if I’m just a housewife.” – P14. | |
| Challenging Traditional Roles | Questioning gendered expectations | “Why is it only men who can decide everything? We care about health too.” – P38. |
| Breaking the silence on harmful habits | “Before, I stayed quiet. Now, I tell him directly that smoking is dangerous.” – P47. | |
| Role Expansion | Taking leadership in household health | “I’m the one who reminds everyone about health now, including my husband.” – P30. |
| Becoming a role model for other women | “I hope my story encourages more women to speak up.” – P12 |
Data Processing, 2025.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



