
Submitted:
28 August 2025
Posted:
29 August 2025
You are already at the latest version
Abstract
The government of Ghana, in partnership with HIV-focused civil society organisations, has implemented interventions and programmes to promote consistent and correct condom use with lubricants to combat HIV transmission and acquisition among key populations, including men who have sex with men (MSM), a population disproportionately affected by the HIV epidemic. Despite these interventions, consistent condom use with lubricants among MSM remains low. Other interventions that also support HIV prevention and care for MSM are also being affected by the United States policy shift on financial aid. This study sought to identify interventions that exist to promote the consistent and correct use of condoms with lubricants among MSM in Ghana, while exploring related challenges faced by both service providers and MSM, as well as potential opportunities for improvement. This research employed an exploratory study design. We conducted face-to-face semi-structured interviews among sixteen individuals: seven MSM, four healthcare professionals, and five individuals from civil society organisations. Each interview lasted around 30 to 47 minutes, and all data were collected between April 7- May 2, 2025. The interviews were recorded, and audio files were transcribed verbatim, reviewed, deidentified, and then captured on Atlas.ti version 24 to organise the data. A professional coder generated the codes, after which thematic content analysis was used to develop recurring themes, and sub-themes were formulated. The study identified interventions such as provision/distribution of free condoms and lubricants, education/risk-reduction counselling, dissemination of HIV preventive information, free HIV testing services, and outreach programmes such as peer-led outreaches, MSM community-based outreach programmes, and online outreach volunteer programmes. The main challenges affecting service providers and MSM included stigmatisation of MSM and service providers, discrimination, criminalisation of same-sex sexual activities, human rights violations, inadequate government funding, financial difficulties, not disclosing HIV/STIs status to sexual partners, skipping counselling and HIV education sessions, and partners' refusal to use condoms. The emerged suggestions for improvement of condom services included legislative amendments, policy reforms, continuous education/counselling, provision of free condoms and lubricants, local production of condoms and sachet lubricants, and applying differentiated service delivery models to improve condom and lubricant distribution. The study identified interventions for the promotion of consistent and correct use of condoms with condom-compatible lubricants among the MSM. It further provides insights into service providers’ and MSM challenges, and proposed strategies for ongoing and future improvement. The above findings could support and guide the design of an evidence-based model to improve consistency and correct use of condoms with condom-compatible lubricants among MSM in Ghana.
Keywords:
men who have sex with men
; consistent and correct condom use with lubricants
; HIV
; condom
; lubricant
; unprotected sex
; anal sex
; Ghana
1. Introduction
The spread of the human immunodeficiency virus (HIV) continues to be a major public health concern among Ghanaian key populations, especially men who have sex with men (MSM) [1], whose chance of acquiring or transmitting HIV is almost 20 times greater in unprotected anal sexual intercourse compared to unprotected vaginal sex [2,3,4]. A report from the Ghana Men’s Study III indicated that the prevalence of HIV among MSM has increased from 18.1% in 2017 to 26.1% in 2023 [5]. It is very crucial to use condoms with condom-compatible lubricants as an interventional strategy consistently to stop the spread of HIV among MSM, other sexual minority groups, and the general population [6,7]. According to the United States Agency for International Development (USAID) [8], condoms are effective in preventing HIV transmission by up to 90%, especially when they are used correctly and consistently with the proper lubricant [8]. Among key populations such as gay men, consistent condom use has been reported to effectively reduce the spread of HIV by 70% among individuals who have partners living with HIV, 72% among receptive partners, and 63% among insertive partners [9].
In the recent past, Ghana’s Ministry of Health, in partnership with other non-governmental organisations, developed and implemented several interventions, such as the Ghana National Condom and Water-based Lubricants Programming Strategy 2014-2019, to improve accessibility and reduce the rate of HIV and other sexually transmitted infections (STIs) [10]. Despite the effectiveness of using condoms with lubricants in preventing HIV spread, the prevalence among MSM in Ghana continues to increase disproportionately [11], whilst consistent condom use with lubricants remains low [12]. A study conducted by Abdulai and colleagues among MSM in Ghana using nationwide survey data revealed that only 38.9% of MSM used condoms with condom-compatible lubricants with all sexual partners [12]. Even though consistent and correct usage of condoms with water-based lubricants is effective in preventing HIV transmission [13,14,15,16], the distribution of condoms in prevention programmes remains low (30%), and accessibility is still a challenge for most MSM [5].
Although Ghana’s National HIV and AIDS Strategic Plan for 2021–2025 recognises the specific health needs of MSM [17], nothing has been done to create a conducive atmosphere that makes it easy to access HIV prevention tools such as condoms and lubricants, as well as other interventions and quality healthcare [18]. Factors such as fear of stigmatisation, discrimination, and criminalisation make it difficult for most of the MSM to have easy access to HIV prevention interventions [19,20,21]. Sociocultural norms and social stigma also disrupt national HIV prevention initiatives, discouraging MSM from seeking the necessary healthcare. [18,22]. The Ghanaian laws further criminalise and impose punitive measures against same-sex sexual behaviours; individuals who engage in same-sex activities can be imprisoned for up to three years under section 104 (1)(b) of the Sexual Offences Act, Criminal Code 1960 [23]. The Ghanaian cultural and societal norms also consider individuals in same-sex activities as deviants in society [24,25]. For instance, a survey conducted in Ghana revealed that over 85% of Ghanaians believe that homosexual relationships are not consistent with Ghanaian customs and values and that they undermine the fundamental social structure of Ghanaian society and are, therefore, unacceptable. [22]. The punitive measures against activities of MSM not only weaken efforts to make access to condoms, lubricants, and other interventions easier [26], but also limit the efforts of service providers to reach them with HIV prevention services and other health interventions [27].
In this regard, we carried out a qualitative study involving MSM and stakeholders in HIV prevention, particularly healthcare service providers, technical coordinators, and programme managers from civil society organisations (CSOs), to identify interventions for consistent and correct use of condoms with lubricants among MSM in Ghana, users’ and service providers’ related challenges, and opportunities for improvement. Findings from this study will guide and support the development of an evidence-based integrated model to improve the availability and accessibility of HIV prevention tools, thus enhancing the consistency of the correct use of condoms with condom-compatible lubricants among the MSM population in Ghana [28,29].
2. Materials and Methods
2.1. Study Design and Study Setting
This research employed an exploratory study design where semi-structured interviews [30] were conducted among sixteen individuals: MSM, healthcare service providers in HIV prevention, and HIV-focused programme managers from CSOs to identify interventions for consistent and correct use of condoms with lubricants among MSM in Ghana, user and service providers’ related challenges, and opportunities. The study participants were selected from twelve out of the sixteen regions of the Republic of Ghana. Ghana shares borders with Burkina Faso to the north, Togo to the east, Ivory Coast to the west, and the Gulf of Guinea to the south. Ghana’s administrative capital is Accra, in the Greater Accra Region, and the country is known for its natural resources and agriculture, especially gold and cocoa, which remain a major source of foreign income [31].
2.2. Sample Size and Recruitment Procedure
The study sample comprises sixteen consenting adults. Of these sixteen adults, seven were MSM, four healthcare service providers who work in the area of HIV prevention, as well as two technical coordinators and three programme managers from HIV focused CSOs that offer interventions on condom and lubricant use to key populations. The recruitment of the study participants was done in consultation with the Ghana AIDS Commission (GAC), which has a long history of working with MSM, MSM leaders, and the HIV focused CSOs. For the recruitment of MSM participants, a well-known staff member of GAC first contacted MSM leaders to share information about the research. Those who expressed interest in knowing more about the research were given the contact information of the GAC staff member for further engagement. The GAC staff member provided the research study information letter and the personal information letter to each potential participant, and those who agreed to participate in the study were given the researcher’s contact details for engagement at a convenient time. Potential participants who contacted the researcher were then selected for the study, and appointment dates were set for the interviews at their chosen location and time. For the healthcare service providers, a formal letter was written to their facility heads for approval to invite healthcare service personnel working in HIV prevention and care who provide services to MSM to participate in the study. After receiving notices from the facility heads, the researcher and the GAC staff member visited the healthcare facilities to meet with the potential participants. After explaining the research objectives, risks, and benefits to them, those who agreed to participate were selected, and appointment dates were subsequently set for the interviews at their convenience and location. The same approach was then used to select the programme managers and other participants from the CSOs.
2.3. Inclusion and Exclusion Criteria
Table 1 below shows the criteria for the selection of study participants for the study.
2.4. Data Collection
Semi-structured face-to-face interviews were conducted to collect participants’ information in private rooms at either the workplace or a location chosen by each participant for convenience, privacy, and safety. During the face-to-face interview sessions, only the interviewer (researcher), interviewee (participant), and the note-taker (GAC staff member) were present. The research objectives and a review of the privacy declaration were clarified before the interview. All participants gave written informed consent to voluntarily participate in the research and be audio recorded. All interviews were conducted using the interview guide. The interview guide consisted of two main parts: the first for the MSM and the second for the service providers. All the interviews were conducted in English, and each lasted around 30 to 47 minutes per participant. All the data were collected from 7th April 2025 to 2nd May 2025.
2.5. Data Analysis
After the interviews, the first author (RA) transcribed the audio interview recordings verbatim. The interview transcripts were then deidentified by removing any information that could be used to trace or identify the participants. A comprehensive review and re-review of all the transcripts was done by the first author (RA) and an external coder to become familiar with the content. The reviewed transcripts were then uploaded to Atlas.ti version 24 to organise the data. After reading the entire dataset, the professional coder independently used Atlas to generate the codes, and any differences were resolved using an intercoder agreement. This was done by employing an inductive coding approach. The coder then finalised the codes. Thematic content analysis was then utilised to create themes and sub-themes from the codes.
2.6. Ethical Considerations
This research paper is part of the first author’s (RA) doctoral study and was conducted in accordance with the Declaration of Helsinki. The study received ethics approvals (REC-2742-2024) (Appendix A) from the Research and Ethics Committee of the University of Johannesburg and the Ghana Health Service Ethics Review Committee (GHS-ERC:007/01/25) (Appendix B). The doctoral study also falls under a broader research project at the South African Medical Research Council (SAMRC)/the University of Johannesburg (UJ) Pan African Centre for Epidemic Research (PACER) Extramural Unit funded project, namely “Harnessing Big Heterogeneous Data to Evaluate the Potential Impact of HIV Responses Among Key Populations in Generalized Epidemic Settings in Sub-Saharan Africa” (REC-1504-2023). Before the informed consent was obtained, the study participants were provided with the full research details, including the objectives, methods, anticipated benefits, and possible risks. Voluntary and written informed consents were taken in private rooms at a convenient location of each participant’s choice. They were informed that the decision to participate in the research rested solely on them, and no form of coercion, deceit, or influence was used on them. The note-taker signed a confidentiality agreement to ensure no information would be divulged without the participant’s permission. Pseudonyms were used for each participant to ensure that no identifiable information was found in the interview transcripts.
3. Results
3.1. Characteristics of the Study Participants
Table 2 shows the characteristics of service providers and MSM who participated in the study. For the MSM participants, four of them were gay, two were bisexual and one was Queer, indicating the diversify nature of their sexual orientations. All the MSM participants were between 20 and 31 years old, with one (1) of them in the early 20s, middle 20s (2), late 20s (2), and two in their early 30s. The majority (5) of them were employed. The majority of the service providers were females (7) and two males, with their ages ranging from 29 to 56 years. Three (3) participants were in their 40s, three in their 50s, two (2) in their 30s, and one in the late 20s. Four service providers were nurses, two technical coordinators from a governmental organisation, and three managers from HIV focused civil society organisations.
3.2. Interventions for Consistent and Correct Use of Condoms with Condom-Compatible Lubricants Among MSM in Ghana
This section has two main parts, namely, service providers’ and MSM responses to interventions for consistent and correct use of condoms with compatible lubricants. The first part describes the themes and subthemes that emerged from the service providers’ interviews, while the second part also discusses the same for MSM. Figure 1 shows the four main themes and their subthemes that arose from the service providers’ responses. They include interventions/current services provided to MSM, accessibility of services, challenges experienced by service providers, and suggestions for improving ongoing and future services.
Theme 1: Interventions/current services provided to MSM
Despite the higher prevalence of HIV among the MSM population in Ghana, the magnitude of consistent condom use with condom-compatible lubricants remains significantly low. Therefore, the authors were interested in identifying what interventions exist to improve the consistency of the correct use of condoms with condom-compatible lubricants. Theme 1, which consists of five subthemes, addresses the abovementioned question.
Sub-theme 1.1: Providing condoms and lubricants.
The participants stated that to ensure that MSM use condoms consistently with condom-compatible lubricants, they provide them with free condoms and water-based lubricants as an interventional strategy. However, some of the participants also stated that sometimes they do not have enough lubricants to give out to MSM compared to the condoms.
“For the MSM, we do supply them with their condoms. The condoms that are available are already lubricated, so we don’t have plain condoms and lubes. There are lubricated condoms that are available that we give to them”. (Service provider H, 56 years old, female)
“We give them condoms and lubes, just that with the lubes we don’t have the quantity that we need, but for condoms, we have enough condoms”. (Service provider I, 45 years old, female)
“OK, so currently we have the flavoured condoms that are available at the Community level. We also have water-based lubricants, like in the sachet form, so the lubricants come in 5ml per sachet, and then we also have condoms. Usually, these condoms are no-label condoms, but they are they are flavoured condoms, so we have the strawberry flavour, we have banana flavour, and we have the lemon flavour. So, we have basically three main flavours that we use for our prevention programming”. (Service provider M, 39 years old, male)
Sub-theme 1.2: Pre-exposure prophylaxis and post-exposure prophylaxis services
The Participants mentioned that in order to maximise the effectiveness of consistent condom use with lubricants in preventing HIV/STIs transmission, they encourage the MSM to adopt a combination prevention strategy by taking the PrEP and post-exposure prophylaxis (PEP). Even though PrEP offers protection against the transmission of new HIV infections, it does not protect against other STIs. Therefore, MSM are strongly advised to use the combination prevention intervention to benefit fully from the synergistic protection that both condoms with lubricants and PrEP confer.
“Apart from the condoms, we also give them the PrEP and the PEP”. (Service provider H, 56 years old, female)
“And you know that the major prevention intervention approach we have for the MSM community is condom and lubricant programming, even though we have PrEP as part of the prevention programme that we implement when it comes to combination prevention approaches”. (Service provider M, 39 years old, male)
“So basically, we do PrEP services at our end, and so when they come, it’s the whole package. So, we give them the PrEP medication in addition to the condom and lubricant programming”. (Service provider N, 31 years old, female)
Sub-theme 1.3: Counselling and education
Education and counselling emerged as effective interventions to promote the consistency of the correct use of condoms with compatible lubricant. The education enlightens MSM on HIV prevention strategies, correct and consistent usage of condoms with lubricants, benefits of safe sex, and risks of transmission. The risk-reduction counselling enables MSM to make an informed decision to practice safe sex.
“So, we have the peer educators, who are also MSMs who know their members very well and even where they can find them, and so we work through them to distribute condoms and lubricants and also educate them on how to use the condoms with the lubricants correctly and consistently. And we also do HIV sensitisation and screening among the population, making sure that they are properly educated on HIV and STIs preventive measures”. (Service provider P, 47 years old, male)
“There are other interventions, such as training peer educators to reach out to the community, to give education. So, the education is such that it is basically informing the volunteers about what HIV is and how to prevent it. So, we have something that we call prevention info as part of the education that we do. So, under prevention info, which is prevention information, they speak about HIV, the modes of transmission, and then how to prevent HIV, which is the usage, the correct and consistent use of condoms with lubricants, and the use of PrEP and then PEP”. (Service provider O, 29 years old, female)
“You know, we also give them education and sometimes even counsel them on the consistent and regular use of condoms and the lubricants. When you give them the condoms and you counsel and educate them, you know, they embrace everything. They absorb everything quickly, and then they feel the importance of using the lubricants with the condoms. So, the counselling and education go well. “ (Service providers J, 48 years old, female)
“So, during their refills, whenever they visit the clinic, we educate and remind them of the continuous use of these things, and then we supply them when they need be”. (Service provider L, 52 years old, female)
Sub-theme 1.4: Outreach programmes
Community outreach programmes, online and peer-led outreach programmes, are essential strategies for promoting consistent and correct use of condoms with lubricants among MSM by creating awareness and also giving them the opportunity to get access to free condoms and lubricants.
“The Commission (GAC) came out with several interventions to support MSMs, one of the key ones is the peer-led outreach that is using their own people to help them”. (Service provider K, 50 years old, female)
“OK, so we work on the Global Fund Grant Cycle 7 Projects and our target population, specifically, is MSM and transgender populations. And we have condom and lubricant programming, and the Community outreach intervention that we implement under the Global Fund Grant Cycle 7 Project. Now, basically, we are heavy on the condom and lubricant programming, and we rely on peer outreach volunteers as another form of interventional strategy, and the community outreaches to get condoms and lubricants to the MSM communities across the various districts that we work in “. (Service provider M, 39 years old, male)
“There are other interventions, such as training peer educators to reach out to the community, and outreach programmes by volunteers to give education. Apart from organising community outreach programmes where we distribute condoms and lubricants to them, and also give them education, the peer educators also used to do peer-led outreach to visit, educate, and distribute condoms and lubricants to them”. (Service provider O, 29 years old, female)
Sub-theme 1.5: HIV prevention and testing
Testing for HIV is a very useful intervention for promoting consistent condom use with lubricants. Participants elaborated that individuals who test for HIV and know their status tend to use condoms with lubricants more consistently.
“We provide the full package, like testing for HIV, distributing flyers, and some of these Flyers educate them about condom and lubricant use”. (Service provider P, 47 years old, male)
Theme 2: Accessibility of services
Having easy access to HIV/STIs preventive tools, such as condoms and lubricants, is very important to ensure consistent usage. The study participants indicated that MSM who have easy access to condoms and lubricants are more likely to practice safe sex compared to those who have difficulties in accessing them. This theme identified the various routes through which condoms and lubricants are made available to the MSM population. The theme has two subthemes, namely awareness of the services and healthcare facilities.
Sub-theme 2.1: Awareness of the services and enhanced access through a peer-led approach
The service providers elaborated that creating awareness of an implemented interventional strategy helps increase individuals’ access and uptake. The service providers indicated that using platforms such as social media, outreach programmes, and the use of mobile vans creates more awareness about the use of condoms with lubricants for safe sex and also makes accessibility very easy.
“OK, so our major yielding point has been social media. There are trained cadres who are online on the various social media platforms, who get them to us, and who try to link them to us. We use digital platforms like social media. We also have Facebook, we have WhatsApp, and we have other dedicated platforms like Instagram”. (Service provider L, 52 years old, female)
“Ok, so some of the ways to reach out to them are community outreach programmes, the peer-led outreach programmes, that is, using their own people to help them; we train these peer-led groups to distribute condoms and water-based lubricant, directly to MSMs within their communities. The West African AIDS Foundation (WAAF) also uses the mobile spot to distribute condoms and lubricants to MSM. Well, for example, WAAF has a mobile van that goes out to provide services for their MSM clients”. (Service provider K, 50 years old, female)
“Ok. So, we mostly use peer educators and community outreach programmes to be able to distribute condoms and lubricants to them. So, you know, the MSM, they have something like cells or like circles. So, we have the peer educators, who are also MSMs who know their members very well and even where they can find them, and so we work through them to distribute condoms and lubricants”. (Service provider P, 47 years old, male)
Sub-theme 2.2: Healthcare facilities
The healthcare facilities, particularly the clinics, serve as vital conduits for making condoms and lubricants easily accessible to MSM. Some of the service providers confirmed that some of the easiest ways for MSM to get free condoms and lubricants are the clinics and drop-in centres when they visit the facilities for their refills, or HIV/STIs testing services.
“So as a clinical nurse at my place, it’s normally the walk-in that we do, but then we have the programming aspects that they also sometimes go do the distribution through community outreaches. But pertaining to me, we do give them the condoms and the lubricants when they come to the clinic”. (Service provider N, 31 years old, female)
“Another area that we’ve also leveraged is the drop-in centres. So, we have drop-in centres among the non-governmental and civil Society organisations implementing MSM programmes where it’s very convenient for the client or the person to go and access condoms and lubes”. (Service provider K, 50 years old, female)
Theme 3: Challenges experienced by service providers
Regarding providing services to the MSM community, the authors were also very interested in identifying the challenges or barriers confronting the service providers and exploring how those challenges or barriers could be addressed or mitigated from the service providers’ perspectives. Theme 3 identified the barriers or challenges the service providers face in delivering their services to the MSM community. It consists of four subthemes, which are elaborated below.
Sub-theme 3.1: MSM compliance
Most of the service providers mentioned that they have challenges with some MSM not complying with directives such as using condoms with lubricants consistently, disclosing their HIV/STIs status to their partner, and also not making themselves available for detailed education on HIV/STIs prevention strategies, as well as risk-reduction counselling services.
“I see that if you have your preferred choice of sexual behaviour, and then you know that these are the risks that are involved, I think that you should even get your condom by yourself to protect yourself. You shouldn’t even wait for the health facilities to give it to you. We are giving it to them, but we still realise that the usage of the condom with lube is low. I have a typical story here where one person who was coming in as HIV negative MSM, we kept talking to him, giving him the condoms, and PrEP. We kept encouraging him to be coming, but little did we know that he was not using them consistently. We are giving them the condoms and PrEP, we are giving them the counselling, but the usage is low. Other challenges that we are facing, especially for my facility. I think that though we are doing a lot of education on protected sex, we don’t know whether it is really sinking in, or a behavioural thing that they still think that it’s better to do the lube alone without the condom. It’s something that is quite worrying “. (Service provider H, 56 years old, female)
“We do give them condom and lubricant education, but it’s not that intensive. So, the education that we give to them at the healthcare facility is not that detailed because most of them are usually in a hurry to leave”. (Service provider N, 31 years old, female)
“For those who quickly rush out because they are in a hurry to leave after receiving their condoms without the education and the counselling, the majority of them come with their partner, and you will see that all of them have tested either positive for STIs or even HIV”. (Service provider J, 48 years old, female)
Sub-theme 3.2: Challenge in providing services
The service providers highlighted that some of the difficulties they face while providing services are shortages of supplies, such as condoms and lubricants.
“So when there are delays in the supply chain, it affects all of us. There will definitely be delays in bringing them into the country, and also when it comes to in-country, I think there’s also a delay between the FDA approval of these condoms and it being offloaded into the country. I heard we pay taxes and some charges at the port. We also have challenges sometimes with lubes. So, there are shortages, sometimes also with condoms, and therefore we may have an abundance of condoms here that we can distribute, but we wouldn’t have lubes to distribute, water-based lubricants to distribute, because sometimes there are shortages of lubes in the system”. (Service provider K, 50 years old, female)
Sub-theme 3.3: Availability of funds.
One of the challenges that emerged was the government’s inability to procure condoms and lubricants, and a lack of funds to purchase condoms by MSM when donor-funded commodities run out. The service providers elaborated on how difficult it can be for some MSM to purchase their condoms and lubricants in times of shortages, or even getting transportation fare to get them to clinics to access these services. They also highlighted that it is sometimes difficult for them to use their income to chase other organisations for condoms and lubricants for their MSM clients. Inadequate funds from the government to purchase enough condoms and lubricants is a significant barrier to them.
“The other challenge, too, is that of finance, because when it comes to them buying the lubricant, it’s really a challenge, so you give them condoms, ask them to go and buy the lubricants, and they are not able to buy them. And then another challenge, too, is how to even sometimes get TNT (transport fare). You know, some of them, because of the stigma, they’ve even lost their jobs, and when it comes to them picking up a car to your place, though, they might not spend any huge amount of money, but sometimes even what they will use to buy water, some of them don’t have”. (Service provider I, 45 years old, female)
“The Ghana Government does not make enough provision for funds to be allocated in the budget for such activities to be given free to these community members”. (Service provider K, 50 years old, female)
“I sometimes have to chase it from the National AIDS control programme, at times the Ghana AIDS Commission. So, with all these other areas that I’m looking at to get these supplies, I will need a vehicle, delivery, transportation, or something. But because it is not coming from the mainstream medical stores that the hospital knows, it becomes difficult because it looks like an extra burden going out of the usual way to get supplies. Sometimes it’s done with our money. Sorry to say, but that’s the reality”. (Service provider L, 52 years old, female)
Sub-theme 3.4: Stigma towards MSM
Stigmatisation of MSM is a huge barrier to accessing HIV/STIs prevention and treatment services. Most MSM suffer human rights violations, and same-sex activities are also being criminalised by existing laws in the country. These make it a challenge for them to freely access intervention tools due to the fear of being identified or bullied by others.
“Ok. So, one of our main challenges currently is that, because of the USAID policy shift on aid, the CSOs who are implementing HIV prevention programmes and activities are having serious challenges because they are not supposed to target KPs such as the MSM. They can provide services to the general population but can’t target any key population; otherwise, they are breaching the agreement”. (Service provider P, 47 years old, male)
“Yeah, most of the challenge is that. They stigmatise themselves first, and they feel that if anybody sees them, it’s a problem. So, self-stigma and discrimination by others are a barrier, especially for those living with HIV. So, sometimes they stigmatise themselves, and others also stigmatise them. That alone doesn’t make most of them come out to access HIV intervention services”. (Service provider J, 48 years old, female)
“Well, the challenges are enormous, honestly. They cut across various angles, ranging from human rights violations, abuse, and one major challenge we have faced as an organisation is the Human Sexual Rights and Family Values Bill that was introduced in 2021 and was passed by Parliament in 2023, I think last year. The challenge is that it created a hostile environment, and it pushed a lot of the KP Community into hiding, so it became very difficult to reach them and provide them services and those who will even come forward to access services are always also kind of like afraid and agitated and all that, so these are some of the main challenges that we’ve encountered. Human rights violations in terms of physical abuse, emotional abuse and harassment towards the MSM community are some of the major challenges that we continue to face in our implementation, and in fact also the programme staff as well also tend to face a lot of challenges in terms of our safety and security as well”. (Service provider M, 39 years old, male)
Theme 4: Suggestions for improving ongoing and future services
Having identified the challenges or barriers that confront the service providers, the authors further explored how those challenges or barriers could be addressed or mitigated from the service providers’ perspectives. Theme 4 addresses these barriers or challenges with three subthemes, namely, continued service delivery, government legislation and policy reforms, and improving service delivery.
Sub-theme 4.1: Continued service delivery
The service providers reaffirmed that, despite the challenges facing them, there is a need to continue providing HIV prevention education and risk-reduction counselling, using peer-led outreach programs to get hard-to-reach members, and the continuous provision of free condoms and lubricants.
“I think that education has to go down well to be able to eliminate the stigma. The sensitisation of the public has gone down; therefore, we need to sensitise the general public to know that everyone has what they want to do. So, you don’t need to look down on someone. Just like how some are doing on malaria and TB, the education has to be intensified so that people will accept it. We should also educate and sensitise both healthcare workers and the general public on the implications of the stigma and how bad it can be for all of us as a country in terms of achieving HIV epidemic control and eliminating STIs “. (Service provider I, 45 years old, female)
“The Ghana Government must make a provisional allocation of funds to be used in the budget for the procurement of condoms and lubricants to be given free to these community members in the short term”. (Service provider L, 52 years old, female)
Sub-theme 4.2: Government legislation and policy reforms
Men who have sex with men in Ghana face serious issues with regard to certain unfriendly legal provisions in the Criminal Offences Act, 1960. The current laws criminalise and discriminate against them. The service providers are of the opinion that the government must be committed to amending the laws that criminalise MSM and also make policy reforms that specifically target the needs of MSM to ensure that they live freely without fear and also have easy access to HIV prevention interventions.
“OK. So, as we talked about policies, I think policy reforms and constitutional reforms are very essential in addressing the stigma, discrimination, and the hostility. So in order to be able to address stigma and discrimination, human rights abuses and violations and all the issues that exist within the key population implementation space, we really need reforms and the reforms must include decriminalisation of existing laws that criminalise the activities of MSM and other communities that have been raised under these laws, otherwise, any other policy we implement will be in vain because if the very community you are implementing those programmes for, are criminalised of course everything will be in vain, we have instances where our team has gone for an outreach and police have arrested them because they are suspected to be part of a certain community or they are suspected to be provided services or supporting the activities of MSM”. (Service provider M, 39 years old, male)
Sub-theme 4.3: Improving service delivery
The service providers reiterated that it is absolutely important that measures are put in place to improve the services being delivered to the MSM community. These should enable them to have a continuous supply and easy access to condoms and lubricants.
“The provision of services to MSM communities must rely more on the use of peer educators to deliver their services. For instance, we, at the Ghana AIDs Commission, when we have condoms, we have ways in which we are able to channel some to the MSM community. That is where we mostly use their peer educators. So, it is necessary that more peer educators are trained for this purpose. Service providers also need to train their staff to be understanding and empathetic to handle MSM-related issues and provide services to them without any form of judgment or prejudice”. (Service provider P, 47 years old, male)
“Again, in terms of condoms and lubricant distribution, we can also use the condom vending machines at strategic places to deliver them. We must have the condom vending machines at strategic locations where we can feed the condoms in so that people could just put in a 20 pesewa coin and it dispenses it for them”. (Service provider P, 47 years old, male)
“The government should also incentivise some of the local manufacturing and pharmaceutical companies to start producing condoms and sachet lubricants to be used locally and stop relying on foreign AIDS”. (Service provider M, 39 years old, male)
As already mentioned above, Figure 2 shows the five main themes and subthemes that arose from MSM responses to interventions for consistent and correct use of condoms with condom-compatible lubricants. The themes are as follows: MSM awareness of service programmes and consistent condom use with lubricants, MSM understanding of consistent condom use with lubricants, MSM experiences of service programmes and condom use, challenges encountered in service provision and condom use, and MSM suggestions for ongoing and improved services.
Theme 1: MSM awareness of available services and consistent condom use with lubricants
Men who have sex with men are a unique population of individuals with specific HIV/STIs prevention needs. The MSM population has a lower prevalence of consistent condom use with condom-compatible lubricants, yet they are the most affected in terms of HIV prevalence in the country. The consistent and correct use of condoms with condom-compatible lubricants has been reported worldwide as the most effective strategy in the prevention of HIV/STIs. The authors were interested in finding out MSM’s awareness level of programmes or interventions that exist to ensure that MSM use condoms with condom-compatible lubricants correctly and consistently. Theme 1, consisting of two subthemes, addresses the above.
Sub-theme 1.1: Awareness of Service Programmes
The participants expressed their awareness of interventions that have been implemented by some HIV/STIs-focused civil society organisations to enable them to protect themselves from HIV/STIs.
“OK, so I know about the Epic programme. I know sharper programmes. I know sharp programmes. And then there is a recent programme also going on, which is. I have forgotten the full name, but I know I also know about the NFM 3 projects. So, Epic focuses on interventions such as community outreaches or reaching out to MSM, or let’s say, MSM community members. Educating us on HIV, condoms, and the correct use of condoms and lubricants. The Epic programme also comes with distributing condoms and sometimes lubricants and counselling MSM community members. Also, those who are eligible to be enrolled on PrEP and those who test positive are also initiated on ARVs, and that applies to all the prevention programmes I have mentioned”. (MSM A, 28 years old, Gay)
“Yeah. Ok, I know about some NGO’s like WAAF and HFFG that have some interventions in place for the MSM community members. Emmm, because of the stigma, we prefer vulnerable populations so that we are not easily identified and harmed. Both WAAF and HFFG have interventions that enable the community members to use condoms and lube consistently and correctly so that we can protect ourselves from HIV and other STIs. They give us education on the correct and consistent use of condoms with lubricants. Again, they organise outreach programmes where they give us condoms and lube, that’s the water-based one. Apart from the education they give us and the sharing of the condoms and lubes, they also train some of the vulnerable people to become peer educators who also check on us and distribute condoms and lubricants to us. The peer educators always make sure that we have what we need to protect ourselves”. (MSM D, 30 years old, Gay)
Sub-theme 1.2: Awareness of condoms and lubricants
The MSM study participants also identified and elaborated on some of the condoms and lubricants available to them, their preferences, and the ones they usually get from the civil society organisations and the clinics or hospitals.
“For the condoms, I only knew about those they sell in the pharmacy, like ..eemm the latex condoms, Durex, Fiesta Classic condoms, and flavoured condoms and also a UK-based condom called Skyn condom, until I started going for outreach programmes where we always get the programme condoms or the non-branded ones. And for the lubes, I know of water and oil-based lubes, but we don’t always get the lubes from our people”. (MSM B, 25 years old, Bisexual)
“As for the condoms and lubes, I know Durex, latex, flavoured, silicone lubricant, water-based lubricant ..eemm, but I personally use the programme condoms and the water-based lubricants. There are times that I don’t have water-based lubricants, so I also use oil-based lubricants. emmm.. that is baby oil that I buy from cosmetic shops”. (MSM E, 26 years old, Bisexual)
“Yeah. I know Durex, latex, the flavoured condoms, and the programme, or the non-branded condoms. Ok, and as for the lubricant, I know only about silicone and water-based ones. Yes, personally, I use the water-based lubricant. We get them without paying anything, but in most cases we don’t get the lubes from the store, so I buy my own lubes, but it’s expensive”(MSM D, 30 years old, Gay)
Theme 2: MSM understanding of consistent condom use with lubricants
In the fight against the spread of new HIV/STI infections among MSM, the consistent and correct use of condoms with the right lubricants is very important. Therefore, understanding this concept is very crucial. The authors sought to explore how MSM in Ghana understand what is meant by consistent condom use with condom-compatible lubricants, and this was addressed by two subthemes, namely: understanding reasons for consistent use of condoms with lubricants for ease of penetration and prevention of HIV and STIs transmission and understanding that condoms must be used with lubricants consistently.
Sub-theme 2.1: Understanding reasons for consistent use of condoms with lubricants for ease of penetration and prevention of HIV and STIs transmission
Most of the MSM study participants expressed their views on how they understood consistent and correct use of condoms with lubricants. Some of them, however, expressed their opinions on the reasons for using condoms with lubricants consistently.
“I don’t think it would be comfortable or safe to use a condom without the lubricant. So yeah, I think it’s definitely better to use condoms with the lubricant every time. I mean, when you apply the right lubricant, it makes the penetration easy without friction; condoms also don’t break unless one doesn’t open them appropriately, and then sex becomes pleasurable. The most important thing is that using it together with the lubricant protects oneself from HIV and STIs, since there is no skin-to-skin contact, there can’t be transmission”. (MSM F, 30 years old, Queer)
“I think both are important because personally, I know people who are like, oh, the condom alone doesn’t make them have that sexual urge, it looks like it prevents them from having that intimate feeling. But when they are used with the lubricants, they become more, they have more of the body touch, more like the body touch. So, I think both work perfectly. Yes, yes, yes, it also allows for smooth penetration and in that case, there is little or no chance for the condom to break; hence, using both condoms with lubricants ensures safety and prevents someone from getting HIV or STIs from an infected person”. (MSM G, 26 years old, Bisexual)
Sub-theme 2.2: Understanding that condoms must be used with lubricants consistently
The participants again expressed their opinions on the understanding of how condoms must be used with lubricants correctly and consistently.
“So, how well I understand it is that I know that I have to use the condom with the lubricant...emm, the water-based lubricant anytime that I sleep with someone. And it gives the opportunity not to be infected with STIs or HIV.”. (MSM A, 28 years old, Gay)
“For me, what I know is that if you use the condoms with the lubricants to protect yourself, it’s more protective than other stuff because even though we know about PrEP, which we also use but the PrEP can only prevent you from HIV and not other STIs you can get them. So, by using condoms with lube, I think you are free. So, we must always use the condoms with the lubes every time to protect ourselves. This is how I understand consistent and correct use”. (MSM E, 26 years old, Bisexual)
Theme 3: MSM experiences of service programmes and condom use
This theme aimed to find out the experiences of the participants about the services they receive in terms of the accessibility and effectiveness of the interventions for the promotion of consistent and correct condom use with lubricants. The 3 addresses this, and it comprises four subthemes elaborated below.
Sub-theme 3.1: Experience the outreaches and provision of condoms and lubrication, together with counselling and education, as very effective (7)
Here, the MSM participants expressed their opinions on which of the interventions works better for them in terms of effectiveness as it relates to protecting oneself from contracting HIV/STIs. Most of the participants indicated that using the combination of prevention interventions works better for them in terms of protection against contracting HIV and STIs.
“Ok, like I said earlier, all the interventions that I know of are effective collectively. Just one single intervention cannot be that effective in making sure that condoms with lubes are used consistently and correctly. We need the education, giving out the free condoms and the lubes and the counselling to make it work”. (MSM D, 30 years old, Gay)
“Ok. As for the interventions, I will say that combining the education and the advice that they give us, counselling us, and also getting access to the condoms and lubes from outreach programmes, in my view, is effective. Because if I have the condom or lube and I don’t know how to use it properly, it cannot protect me from HIV or STIs. What I want to say is that the education, the counselling, and having the condoms and lubes all combined make it effective”. (MSM B, 25 years old, Bisexual)
Sub-theme 3.2: Do not use the programme condoms, so have no opinion (2)
Some of the participants stated clearly that since they do not use the programme condoms, they do not have any opinion on their effectiveness.
“About the effectiveness of the various programmes or interventions, that will be very hard to say because it will be a bias for me to say that a particular programme is not really effective when I’m linked to a different programme and not that one. Well, I can’t speak much about what I don’t know”. (MSM C, 21 years old, Gay)
Sub-theme 3.3: All participants prefer the use of condoms together with lubricant
During anal sexual intercourse, there is a greater likelihood of experiencing condom breakage if additional lubrication is not provided hence, it is very important to consistently use the condoms with condom-compatible lubricants. The participants expressed their views on using condoms with lubricant.
“Yes, I always use condoms and lubricants anytime. That’s more consistent and correctly, like using all the time, no matter who you are. I like to learn and do research, so I know the figures. I mean the HIV prevalence. I think that as of now, it is at 26.1. People are infected with HIV, so if you really want to protect yourself, you know, you have to use it always. So, for me personally, I use them always. Using condoms with lubricants is very good because when I started using them, I didn’t experience friction anymore during penetration…eemm and now the pleasure is much more enjoyable, especially with the Skyn condom, and I also don’t experience condom breakage when I use the condom with the water-based lube. When the condom doesn’t break, it saves me from any sexually transmitted infection and HIV”. (MSM B, 25 years old, Bisexual)
“Ok, personally, for me, I prefer to use condoms with lube, which is the best because it makes penetration easy, reduces friction, and even enhances pleasure. The condoms don’t break or tear when lubricants are used, so they prevent skin contact and prevent one from contracting STIs and HIV. “(MSM D, 30 years old, Gay)
Sub-theme 3.4: Condoms and lubricants are easily accessible (8)
One of the most important things to consider with regard to using condoms with lubricants consistently is accessibility. Individuals who have easy access to condoms and lubricants are more likely to use them consistently compared to those who experience difficulties in accessing them. Most of the participants indicated that accessibility is not a difficult issue for them.
“Yes. Wherever I need condoms and lubes, I call my peer educator, and he comes home to give me some, even if it’s midnight, because we stay in the same area. And for the lubricants, I make sure to buy some from the pharmacy because the lubes are not always available from him”. (MSM B, 25 years old, Bisexual)
“Yes, I have easy access to the condoms in particular. Immediately, I’m short on items, some of them I have their numbers, I just call them, and they bring me some, and even the peer educator who mostly comes to me, I have his contact, so anytime that I need something, I just have to contact him”. (MSM E, 28 years old, Bisexual)
Theme 4: Challenges encountered in service provision and condom use
The authors explored the MSM participants’ views regarding the challenges or barriers confronting them as community members. The challenges they face were identified under Theme 4, comprising six subthemes.
Sub-theme 4.1: Stigma
Stigmatisation is a significant challenge when it comes to MSM. Participants expressed themselves on the stigma attached to purchasing condoms or lubricants from pharmacies and the stigma from the public.
“Sometimes there is self-stigma, especially when you are in a community where you feel shy to walk into a bar or a pharmacy to buy condoms and then also buy lubricant as well because they mean to buy condoms and lubricant, it tells the person you are going to have either anal sex or any other kind of sex”. (MSM A, 28 years old, Gay)
“Some of our community members wouldn’t want to come out for outreach programmes to be identified or something due to fear of stigmatisation, criminalisation, and others. “. (MSM C, 21 years old, Gay)
Sub-theme 4.2: Availability of condoms and/or lubricants
Some of the participants indicated that they do not have problems with finding condoms, even if they need to go to the pharmacy.
“Yeah, I do. And because of the intervention programmes in the MSM communities, we have volunteers that ...eemm share condoms and lubricants at a free space when we attend like outreach programmes, we get condoms free, and then we get lubricants free. It’s not for sale unless you are at a place where you need to get some, but you don’t have any peer educators or any volunteers who work within any of your friendly NGOs who have it; then you would have to buy it”. (MSM A, 28 years old, Gay)
Sub-theme 4.3: Financial difficulties
Financial difficulty is a significant challenge for most MSM. Some of them indicated that they might not necessarily like the condoms being given to them, but they do not have the money to buy lubricant, especially since they are costly at the pharmacy.
“Sometimes people are not used to the brand that is being given out for free, and...eemm, your skin might react to what is being given for free. Sometimes, when you don’t have the funds to afford what is actually good for you, it becomes a challenge”. (MSM A, 28 years old, Gay)
“Like I said, sometimes we don’t have the lubricant, and buying it is also expensive. There are times that I have condoms, but when I call my peer educator, he does his best to get me at least what I will use for that day”. (MSM D, 30 years old, Gay)
Sub-theme 4.4: Lack of awareness
Some MSM have concerns about inadequate awareness among other community members, especially those living far away from the cities and service provision centres.
“Some people are not aware that there are even organisations out there intervening on behalf of we in the community, and also most people don’t know about the benefits of these packages”. (MSM B, 25 years old, Bisexual)
Sub-theme 4.5: Condoms breaking
A typical challenge associated with using condoms during anal sexual intercourse is condom breakage. Some MSM participants mentioned that using condoms without lubricants or the compatible lubricants during anal sex increases the friction and cause condoms to break thus making it a serious challenge.
“A first when I didn’t know about the water-based lube, I used to sometimes experience condom breakage or tear when I was not using lubes, so it some kind of prevent easy entry and some lubricants can also make the condom weak and cause it to break, probably due to the friction, and penetration gets difficult”. (MSM D, 30 years old, Gay)
Sub-theme 4.6: Partner refusing condoms or lubricants
Sometimes, sexual partners’ refusal to use condoms with or without lubricants is another challenge to most MSM, especially for individuals who feel shy to insist on condom use with lubricants or negotiate for safe sex. Some participants express their opinions on their partners’ refusal for protected sex and the actions they have to take to keep themselves from contracting HIV or STIs.
“Well, there are people who say they don’t like the condoms and the lubes. I meet people who say that they don’t use condoms, but it’s not my thing. So, I will insist on using condoms or no sex at all”. (MSM F, 30 years old, Queer)
“I don’t have difficulties in getting condoms because I’m in the city, and it’s easy to get condoms. There are about 5 pharmacies around me, so even if I don’t get it from my peer educators, I’m going to get it there, but the only challenge is that I meet people who are like they want raw sex, in that case, the conversation has to end right there”. (MSM G, 26 years old, Gay)
Theme 5: MSM suggestions for ongoing and improved services
After identifying the major challenges facing the MSM community, the authors also explored their views on addressing the challenges. The suggested solutions were put into four subthemes: education and awareness, making sachet lubricants more affordable, Improved accessibility of condoms and lubricants, and Improved government involvement in services.
Sub-theme 5.1: Education and awareness
The participants indicated that intensifying education on consistent condom use with lubricants by highlighting the risks and benefits of safe sex practices, as well as creating awareness of HIV prevention strategies through social media platforms and service centres, and also sending out HIV prevention messages via SMS, are essential tools to rely on.
“There can be consistent public education to increase awareness among the MSM community members, using peer educators to reach out to members…eemm I’m a benefactor, so I know what I’m talking about. Public awareness can be done through social media platforms like Facebook, Instagram, and Television channels”. (MSM B, 25 years old, Bisexual)
Sub-theme 5.2: Making sachet lubricants more affordable
One of the challenges that emerged was inadequate lubricants from suppliers and the high cost of water-based lubricants at the pharmacies. The participants suggested that condom-compatible lubricants be produced locally in sachet forms to make them readily available and affordable.
“…eemm producing lubes in sachet forms to reduce cost and increase availability. Yeah, that’s by making the sachet lubricants more affordable and available so that the pockets can afford”. (MSM A, 28 years old, Gay)
“The companies should also produce sachet lubricants that are affordable so that we can always buy them. It will be very good if sachet lubricants can flow just like the way condoms are always or mostly available”. (MSM D, 30 years old, Gay)
Sub-theme 5.3: Improved accessibility of condoms and lubricants
Improving access to condoms and lubricants makes it convenient and increases their willingness to use them consistently. The participants pointed out that using the peer educators to distribute condoms and lubricants makes accessibility very easy for them.
“To make the condoms easily accessible to us, there should be a continuous supply to our peer educators so that anytime we need some, we can contact them. Yes, they are close to us and getting it from them is very easy than going out to the public”. (MSM D, 30 years old, Gay)
Sub-theme 5.4: Improved government involvement in services
Since the availability of condom compatible lubricant is a significant challenge for most MSM, and those at the pharmacies also come at exorbitant prices, the participants suggested that there is a need for the government to intervene, making sure that some of the locally manufactured pharmaceutical companies go into the production of quality and affordable sachet lubricants to meet the growing demand.
“Also, the government must set up a company to produce locally produced sachet lubricants that are also affordable to the community members”. (MSM D, 26 years old, Bisexual)
4. Discussion
4.1. Main Findings
This study found five main interventions specifically implemented to promote the consistency of the correct use of condoms with condom-compatible lubricants among the MSM population in Ghana. These are the provision/distribution of free condoms and water-based lubricants, education and risk-reduction counselling, dissemination of HIV preventive information, free HIV testing services, and outreach programmes such as peer-led outreaches, MSM community-based outreach programmes, and online outreach volunteer programmes. The participants stated that while the free distribution of condoms and lubricants removes financial burden from them, it also makes access easier, thus enabling them to use the condoms with the lubricants more consistently. Our findings agree with studies conducted in the Netherlands and Malawi [32,33]. A 2015 joint report by the Joint United Nations Programme on HIV/AIDS (UNAIDS) and the World Health Organisation (WHO) revealed that the distribution of free condoms and lubricants makes accessibility easier and has therefore been shown to significantly reduce the incidence of new HIV and other STIs in both MSM and those involved in sex work. Other studies conducted in India, Zimbabwe, and South Africa also revealed that free distribution of condoms and lubricants to key population groups is linked to a significant reduction in HIV and other STIs [34,35,36,37]. A systematic review done by Carvalho and colleagues (2011) also reported that risk-reduction counselling and peer education promote consistent condom use with lubricant, especially among individuals who know their HIV status [38]. Through outreach programmes and the dissemination of HIV preventive information via SMS and other media platforms, most MSM become enlightened and more aware of the consequences of unsafe sexual practices [39,40]. These interventions also afford them the opportunity to have access to useful educational resources, which empower them to practice safe sex by using condoms with lubricants consistently [41].
Our study identified several challenges confronting both MSM and service providers. Among them are stigmatisation of MSM and service providers, discrimination, criminalisation, and human rights violations. Due to some unfavourable legislative provisions Criminal Offences Act, 1960, MSM in Ghana are criminalised, discriminated against under the current laws, and face stigmatisation by the public. Section 104(1)(b) of the Criminal Offences Act of Ghana 1960 criminalises MSM and same-sex activities. In addition to this law, Ghana again introduced another bill in 2021 called the Promotion of Proper Human Sexual Rights and Ghanaian Family Values Bill, which prescribes serious sanctions against same-sex behaviour [42,43,44]. Under this bill, service providers who are providing services to the MSM communities are even classified as allies, and for that matter, they are also criminalised in the bill. While this makes it challenging for service providers to effectively deliver services, it also sends the MSM community into hiding and therefore unable to access these HIV prevention interventions. Our findings are consistent with a study conducted in Senegal by Dibble and colleagues (2022) and a UNAIDS report, which stated that stigmatisation and criminalisation of MSM affect the availability, access, and uptake of HIV prevention interventions as well as treatment services [45,46].
Another challenge is the inadequate financial provision by the government of Ghana for the procurement of condoms and lubricants to meet the needs of its MSM community. This has increased the reliance of the MSM community on donor organisations like the USAID for HIV prevention interventions such as condoms and lubricants. This, therefore, poses a challenge to the MSM community in Ghana due to the USAID policy shift on financial aid for HIV prevention and treatment programmes. This is confirmed by the findings of a study conducted in 30 SSA countries by Olakunde et al., which reported overdependence on foreign aid by many African countries for a better HIV response [47]. Financial difficulty on the part of most MSM is also a barrier to accessing HIV prevention interventions. Some of the MSM participants mentioned that they sometimes find it difficult to get transport fare to visit the clinic or hospitals where they normally have access to free condoms and lubricants, and PrEP, as well as education and counselling services.
Again, shortages of water-based lubricants and sometimes condoms are a major challenge to most MSM, especially for those who do not have the means to buy them from the pharmacy or feel afraid to access them from public sources. As mentioned above, because of the government’s inability to make provisions in the budget to ensure a continuous supply of condoms and lubricants to the MSM community, any slight delay in the supply chain processes from donor organisations or countries usually leads to a shortage of condoms and lubricants [48]. The service providers further indicated that they usually have an inadequate supply of lubricants, even from donor organisations, which makes it difficult for most MSM to use condoms with lubricants consistently. This might also lead to condomless anal sex among those who are not financially capable of purchasing them.
Additionally, MSM non-compliance with service providers in terms of not disclosing HIV/STIs status to sexual partners and being available for continuous counselling and education is a major challenge. Most healthcare service providers revealed that counselling and education on HIV prevention are very powerful tools in ensuring consistency and correct usage of condoms with lubricants; however, some of the MSM community members refuse to avail themselves to receive HIV education and risk-reduction counselling. Several studies have also reported that MSM who know their partners’ HIV and STIs status are more likely to use condoms with lubricant consistently [49,50]; however, most MSM do not voluntarily disclose their HIV/STIs status to their partners. This agrees with a study conducted in Asia by Wei et al., which reported that over 65% of MSM had not disclosed their HIV/STIs status to their sexual partners [51]
Lastly, partners’ refusal to use condoms consistently, with or without lubricants, undermines HIV prevention efforts. Most of the MSM participants reported that some sexual partners prefer to have unprotected anal sex. This is particularly a major barrier to consistent condom use with lubricants and a challenge for younger MSM who are not empowered enough to be able to negotiate for safe or protected sex. Our finding is in agreement with a study conducted in Kenya by Ngure and colleagues, which reported partners’ unwillingness to use condoms with or without lubricants, irrespective of their HIV/STI status, as a significant barrier to fighting against further HIV spread [52].
The suggested solutions by both service providers and MSM for improving ongoing and future services include legislative amendments and policy reforms to target the needs of MSM. In order to address the stigma and discrimination, human rights abuses and violations, there is a need for legislative and policy reforms. While policy reforms must be made to target the specific HIV prevention needs of MSM, the legislative reforms also must include the amendment of existing laws that criminalise the activities of MSM and other communities that have been targeted under these laws; otherwise, any other policy that is implemented may be in vain. This aligns with studies conducted by Operario et al. (2022) and Thapa et al. (2024), which reported that decriminalisation of same-sex practices reduces structural barriers such as stigma and discrimination and also enhances the uptake of HIV prevention interventions [53,54]. There should also be a continuous provision of free condoms and lubricants by increasing state funding for the procurement of adequate condoms and lubricants for the MSM community. Stakeholders in HIV prevention need to intensify education, counselling, and awareness creation at healthcare facilities and during outreach programmes. The government should incentivise local pharmaceutical companies to go into the production of quality and affordable condoms and sachet lubricants to increase availability and accessibility. Making condoms and lubricants easily accessible by using effective and convenient distribution strategies, such as peer educators, mobile vans, condom vending machines, and drop-in centres.
4.2. Strengths and Limitations
This study contributes to knowledge by identifying interventions implemented to promote consistent use of condoms with lubricant among MSM. It also gives a broader understanding of the challenges that service providers face in the course of their service delivery and within the key population programme implementation space. The study has also highlighted the major barriers that hinder the uptake of HIV prevention interventions among the MSM community. The major strength of this study also includes the interviews of both service providers and MSM and suggestions from both parties on how best their challenges could be addressed. Despite the strengths mentioned above, the study findings may not be generalizable to other key population groups. Again, only service providers who worked within HIV-focused governmental and non-governmental organisations and public healthcare specialists were interviewed.
5. Conclusions
This study provides insights into interventions that exist to promote consistent and correct use of condoms with condom-compatible lubricants among the MSM population in Ghana. The study further identified the challenges confronting both service providers and MSM. Suggested solutions by both service providers and MSM for improving ongoing and future service delivery include legislative amendments to provide a legally friendly environment for MSM, make policy reforms to target the needs of MSM, use efficient and convenient condom and lubricant distribution channels, consider the production of locally manufactured condoms and sachet lubricants to ensure continuous availability and accessibility as well as intensifying education and risk-reduction counseling. The above proposed solutions should therefore inform the development of an evidence-based model, with the goal of improving the consistency of the correct use of condoms with condom-compatible lubricants among MSM in Ghana.
Author Contributions
Conceptualization, R.A (Ratif Abdulai); EP.; and R.N.P.M.; Validation, R.A (Ratif Abdulai); R.N.P.M.; and E.P.; Writing the first draft, R.A (Ratif Abdulai); reviewing and editing, R.A (Ratif Abdulai); EP.; K.A.; R.A (Rita Afriyie); and R.N.P.M.; supervision, R.N.P.M.; K.A.; and E.P.; project administration, R.A (Ratif Abdulai); funding acquisition, R.A (Ratif Abdulai); and R.N.P.M. and EP. All authors have read and agreed to the submission of the manuscript.
Funding
The work reported herein is made possible through funding by the South African Medical Research Council (SAMRC) project Code #57035 (SAMRC File Reference No: HDID8528/KR/202) through its Division of Research Capacity Development under the Mid-Career Scientist Programme using funding received from the South African National Treasury. The first author, Ratif Abdulai, is also supported by the Global Excellence Stature, Fourth Industrial Revolution (GES 4.0) Scholarship. This work is conducted under the auspices of the SAMRC/UJ PACER Extramural Unit. The content hereof is the authors’ sole responsibility and does not represent the official views of the SAMRC or UJ.
Institutional Review Board Statement
The study was conducted following the Declaration of Helsinki and approved by the Research and Ethics Committee of the University of Johannesburg (REC-2742-2024; date of approval: 10 May 2024) and the Ghana Health Service Ethics Review Committee (GHS-ERC:007/01/25; date of approval: 26 March 2025).
Informed Consent Statement
All the participants gave their consent to participate in the study and to be audio-taped during the interviews.
Data Availability Statement
To protect the service providers and the MSM participants from stigmatisation and criminalisation of same-sex sexual behaviour, the data have not been made publicly available. The data are available from the corresponding author upon reasonable request.
Acknowledgments
We sincerely appreciate the support and contributions of the University of Johannesburg, South African Medical Research Council, Pan African Centre for Epidemics Research Extramural Unit, and the Ghana AIDS Commission. We sincerely appreciate all the study participants for taking part in this study. We also appreciate the support of the professional coder, Dr. Peter Schultz.
Conflicts of Interest
The authors declare no conflicts of interest.
Appendix A
Appendix A is the University of Johannesburg Research and Ethics Approval Letter.
Appendix B
Appendix B is the Ghana Health Service Ethics Review Committee Approval Letter.
References
- Ghana AIDS Commission. Ghana Aids Commission Ghana Men’s Study II. 2017; Available from: https://www.ghanaids.gov.gh/mcadmin/Uploads/Ghana Men%27s Study Report(2).pdf.
- Baggaley RF, White RG, Boily MC. HIV transmission risk through anal intercourse: systematic review, meta-analysis and implications for HIV prevention. Int J Epidemiol [Internet]. 2010 Apr 20 [cited 2025 Jun 18];39(4):1048. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC2929353/.
- Mayer KH, Wheeler DP, Bekker LG, Grinsztejn B, Remien RH, Sandfort TGM, et al. Overcoming biological, behavioral, and structural vulnerabilities: New directions in research to decrease HIV transmission in men who have sex with men. J Acquir Immune Defic Syndr [Internet]. 2013 Jul 1 [cited 2025 Jun 18];63(SUPPL. 2). Available from: https://journals.lww.com/jaids/fulltext/2013/07012/overcoming_biological,_behavioral,_and_structural.10.aspx.
- Jin F, Jansson J, Law M, Prestage GP, Zablotska I, Imrie JCG, et al. Per-contact probability of HIV transmission in homosexual men in Sydney in the era of HAART. AIDS [Internet]. 2010 Mar [cited 2025 Jun 18];24(6):907–13. Available from: https://journals.lww.com/aidsonline/fulltext/2010/03270/per_contact_probability_of_hiv_transmission_in.14.aspx.
- UNAIDS. Key Populations Atlas [Internet]. 2025 [cited 2025 May 18]. Available from: https://kpatlas.unaids.org/dashboard.
- Wiyeh AB, Mome RKB, Mahasha PW, Kongnyuy EJ, Wiysonge CS. Effectiveness of the female condom in preventing HIV and sexually transmitted infections: A systematic review and meta-analysis. BMC Public Health. 2020;20(1):1–17.
- Giannou FK, Tsiara CG, Nikolopoulos GK, Talias M, Benetou V, Kantzanou M, et al. Condom effectiveness in reducing heterosexual HIV transmission: a systematic review and meta-analysis of studies on HIV serodiscordant couples. Expert Rev Pharmacoecon Outcomes Res [Internet]. 2016 Jul 3 [cited 2024 Oct 20];16(4):489–99. Available from: https://pubmed.ncbi.nlm.nih.gov/26488070/.
- USAID. Condom fact sheet. Usaid [Internet]. 2015;26(April):1–2. Available from: https://www.globalhealthlearning.org/sites/default/files/reference-files/condomfactsheet.pdf.
- Barcavage Shaun Haun. How well do condoms protect gay men from HIV? San Fr AIDS Found [Internet]. 2016;1–8. Available from: https://www.sfaf.org/collections/beta/how-well-do-condoms-protect-gay-men-from-hiv/.
- Ghana. Plans, Strategies & Reports - National Strategic Plans & Reports [Internet]. 2018 [cited 2025 May 19]. Available from: https://www.ccmghana.net/index.php/strategic-plans-reports.
- Nelson LRE, Wilton L, Agyarko-Poku T, Zhang N, Zou Y, Aluoch M, et al. Predictors of condom use among peer social networks of men who have sex with men in Ghana, West Africa. PLoS One [Internet]. 2015 Jan 30 [cited 2025 May 19];10(1). Available from: https://pubmed.ncbi.nlm.nih.gov/25635774/.
- Abdulai R, Phalane E, Atuahene K, Kwao ID, Afriyie R, Shiferaw YA, et al. Consistency of Condom Use with Lubricants and Associated Factors Among Men Who Have Sex with Men in Ghana: Evidence from Integrated Bio-Behavioral Surveillance Survey. Int J Environ Res Public Health [Internet]. 2025 Apr 1 [cited 2025 May 19];22(4):599. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC12026881/.
- CDC. Preventing HIV with Condoms [Internet]. 2024 [cited 2025 May 18]. Available from: https://www.cdc.gov/hiv/prevention/condoms.html.
- World Health Organization. Condoms Key facts [Internet]. 2025 [cited 2025 May 18]. Available from: https://www.who.int/news-room/fact-sheets/detail/condoms.
- Stover J, Teng Y. The impact of condom use on the HIV epidemic. Gates Open Res. 2022;5.
- UNAIDS. Condom and lubricant programming in high HIV prevalence countries [Internet]. 2015 [cited 2025 May 18]. Available from: https://www.unaids.org/en/resources/documents/2015/Condomlubricantprogramming.
- Ghana AIDS Commission. National HIV & AIDS STRATEGIC PLAN 2021-2025. Angew Chemie Int Ed 6(11), 951–952. 2021;2013–5.
- Kushwaha S, Lalani Y, Maina G, Ogunbajo A, Wilton L, Agyarko-Poku T, et al. “But the moment they find out that you are MSM…”: a qualitative investigation of HIV prevention experiences among men who have sex with men (MSM) in Ghana’s health care system. BMC Public Health [Internet]. 2017 Oct 3 [cited 2025 Feb 26];17(1). Available from: https://pubmed.ncbi.nlm.nih.gov/28974257/.
- Beyrer C. Global prevention of HIV infection for neglected populations: men who have sex with men. Clin Infect Dis [Internet]. 2010 May 15 [cited 2024 Oct 20];50 Suppl 3(SUPPL. 3). Available from: https://pubmed.ncbi.nlm.nih.gov/20397938/.
- Fay H, Baral SD, Trapence G, Motimedi F, Umar E, Iipinge S, et al. Stigma, health care access, and HIV knowledge among men who have sex with men in Malawi, Namibia, and Botswana. AIDS Behav [Internet]. 2011 Aug [cited 2024 Oct 20];15(6):1088–97. Available from: https://pubmed.ncbi.nlm.nih.gov/21153432/.
- Rebe K, Semugoma P, McIntyre J. New HIV prevention technologies and their relevance to MARPS in African epidemics. Sahara J [Internet]. 2012 [cited 2024 Oct 20];9(3):164–6. Available from: https://www.tandfonline.com/doi/abs/10.1080/17290376.2012.744168.
- Osse L. Ghanaians are united and hospitable but intolerant toward same-sex relationships. 2021;(Afrobarometer Dispatch Dispatch No. 461):1–9.
- Ghana. Human Dignity Trust [Internet]. 2025 [cited 2025 May 18]. Available from: https://www.humandignitytrust.org/country-profile/ghana/.
- Persson A, Ellard J, Newman C, Holt M, De Wit J. Human rights and universal access for men who have sex with men and people who inject drugs: A qualitative analysis of the 2010 UNGASS narrative country progress reports. Soc Sci Med [Internet]. 2011 Aug 1 [cited 2025 May 18];73(3):467–74. Available from: https://www.sciencedirect.com/science/article/abs/pii/S0277953611003376?via%3Dihub.
- Williamson R, Wondergem P, J. RAH& HR, 2014 U. Using a reporting system to protect the human rights of people living with HIV and key populations: a conceptual framework. 2014 [cited 2025 May 18]; Available from: https://www.hhrjournal.org/2014/07/01/using-a-reporting-system-to-protect-the-human-rights-of-people-living-with-hiv-and-key-populations-a-conceptual-framework/.
- Ayala G, Makofane K, Santos GM, Beck J, Do TD, Hebert P, et al. Access to Basic HIV-Related Services and PrEP Acceptability among Men Who Have sex with Men Worldwide: Barriers, Facilitators, and Implications for Combination Prevention. J Sex Transm Dis [Internet]. 2013 Jul 8 [cited 2025 May 18];2013:953123. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC4437423/.
- Poteat T, Diouf D, Drame FM, Ndaw M, Traore C, Dhaliwal M, et al. HIV Risk among MSM in Senegal: A Qualitative Rapid Assessment of the Impact of Enforcing Laws That Criminalize Same Sex Practices. PLoS One [Internet]. 2011 Dec 14 [cited 2025 May 18];6(12):e28760. Available from: https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0028760.
- Abdulai R, Phalane E, Atuahene K, Phaswana-Mafuya RN. Consistent and Correct Use of Condoms With Lubricants and Associated Factors Among Men Who Have Sex With Men from the Ghana Men’s Study II: Protocol for a Mixed Methods Study. JMIR Res Protoc [Internet]. 2024 Dec 3 [cited 2024 Dec 26];13(1):e63276. Available from: http://www.ncbi.nlm.nih.gov/pubmed/39626229.
- Abdulai R, Phalane E, Atuahene K, Phaswana-Mafuya RN. Consistent Condom and Lubricant Use and Associated Factors Amongst Men Who Have Sex with Men in Sub-Saharan Africa: A Systematic Review. Sexes 2024, Vol 5, Pages 796-813 [Internet]. 2024 Dec 23 [cited 2024 Dec 26];5(4):796–813. Available from: https://www.mdpi.com/2411-5118/5/4/51/htm.
- Colorafi KJ, Evans B. Qualitative Descriptive Methods in Health Science Research. Heal Environ Res Des J [Internet]. 2016 Jul 1 [cited 2025 May 19];9(4):16–25. Available from: https://pubmed.ncbi.nlm.nih.gov/26791375/.
- Ghana. Republic of Ghana: Key facts. 2025 [cited 2025 Jun 30].African Commission on Human and Peoples’ Rights. Available from: https://achpr.au.int/en/member-states/ghana.
- Rosenberg NE, Graybill LA, Wesevich A, McGrath N, Golin CE, Maman S, et al. The Impact of Couple HIV Testing and Counseling on Consistent Condom Use among Pregnant Women and their Male Partners: An Observational Study. J Acquir Immune Defic Syndr [Internet]. 2017 Aug 1 [cited 2025 Jun 14];75(4):417. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC5493523/.
- Bom RJM, Van Der Linden K, Matser A, Poulin N, Schim Van Der Loeff MF, Bakker BHW, et al. The effects of free condom distribution on HIV and other sexually transmitted infections in men who have sex with men. BMC Infect Dis [Internet]. 2019 Mar 4 [cited 2025 Jun 14];19(1):1–10. Available from: https://bmcinfectdis.biomedcentral.com/articles/10.1186/s12879-019-3839-0.
- Boily MC, Pickles M, Lowndes CM, Ramesh BM, Washington R, Moses S, et al. Positive impact of a large-scale HIV prevention programme among female sex workers and clients in South India. AIDS [Internet]. 2013 Jun 1 [cited 2025 Jun 14];27(9):1449. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3678895/.
- Rachakulla HK, Kodavalla V, Rajkumar H, Prasad SPV, Kallam S, Goswami P, et al. Condom use and prevalence of syphilis and HIV among female sex workers in Andhra Pradesh, India – following a large-scale HIV prevention intervention. BMC Public Health [Internet]. 2011 [cited 2025 Jun 14];11(Suppl 6):S1. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3287547/.
- Halperin DT, Mugurungi O, Hallett TB, Muchini B, Campbell B, Magure T, et al. A Surprising Prevention Success: Why Did the HIV Epidemic Decline in Zimbabwe? PLoS Med [Internet]. 2011 Feb [cited 2025 Jun 14];8(2):e1000414. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3035617/.
- Johnson LF, Hallett TB, Rehle TM, Dorrington RE. The effect of changes in condom usage and antiretroviral treatment coverage on human immunodeficiency virus incidence in South Africa: a model-based analysis. J R Soc Interface [Internet]. 2012 Jul 7 [cited 2025 Jun 14];9(72):1544. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3367823/.
- Carvalho FT, Gonçalves TR, Faria ER, Shoveller JA, Piccinini CA, Ramos MC, et al. Behavioral interventions to promote condom use among women living with HIV. Cochrane Database Syst Rev. 2011 Sep 7;2012(2).
- Jommaroeng R, Richter KA, Chamratrithirong A, Soonthorndhada A. The effectiveness of national HIV prevention education program on behavioral changes for men who have sex with men and transgender women in Thailand. J Heal Res. 2020 Jan 14;34(1):2–12.
- Sabin LL, Semrau K, Desilva M, Le LTT, Beard JJ, Hamer DH, et al. Effectiveness of community outreach HIV prevention programs in Vietnam: A mixed methods evaluation. BMC Public Health [Internet]. 2019 Aug 16 [cited 2025 Jun 14];19(1):1–17. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-019-7418-5.
- Johansson K, Persson KI, Deogan C, El-Khatib Z. Factors associated with condom use and HIV testing among young men who have sex with men: a cross-sectional survey in a random online sample in Sweden. Sex Transm Infect [Internet]. 2018 Sep 1 [cited 2023 Dec 17];94(6):427–33. Available from: https://sti.bmj.com/content/94/6/427.
- Ako EY. Same-sex relationships and recriminalisation of homosexuality in Ghana. Socioling Stud [Internet]. 2023 Nov 4 [cited 2025 Jun 3];17(1–3):45–65. Available from: /doi/pdf/10.1558/sols.24077?download=true.
- Fiaveh DY. LGBQ+ in Ghana: Analysing local and Western discourses. Socioling Stud. 2023 Aug 7;17(1–3):21–43.
- Coleman TE, Ako EY, Kyeremateng JG. A human rights critique of Ghana’s Anti-LGBTIQ+ Bill of 2021. African Hum Rights Law J [Internet]. 2023 [cited 2025 Jun 3];23(1):96–125. Available from: http://www.scielo.org.za/scielo.php?script=sci_arttext&pid=S1996-20962023000100006&lng=en&nrm=iso&tlng=en.
- Dibble KE, Baral SD, Beymer MR, Stahlman S, Lyons CE, Olawore O, et al. Stigma and healthcare access among men who have sex with men and transgender women who have sex with men in Senegal. SAGE Open Med [Internet]. 2022 [cited 2025 Jun 15];10:20503121211069276. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9066634/.
- UNAIDS. Criminalising Homosexuality and Public Health: Adverse Impacts on the Prevention and Treatment of HIV and AIDS 3 2. 2014 [cited 2025 Jun 15]; Available from: http://www.unaids.org/sites/default/files/media_asset/UNAIDS_Gap_report_en.pdf.
- Olakunde BO, Adeyinka DA, Ozigbu CE, Ogundipe T, Menson WNA, Olawepo JO, et al. Revisiting aid dependency for HIV programs in Sub-Saharan Africa. Public Health [Internet]. 2019 May 1 [cited 2025 Jun 15];170:57–60. Available from: https://www.sciencedirect.com/science/article/abs/pii/S0033350619300526.
- UNAIDS. Condoms and lubricants in the time of COVID-19 — Sustaining supplies and people-centred approaches to meet the need in low- and middle-income countries — A short brief on actions, April 2020. 2020;(April):1–3. Available from: https://www.unfpa.org/sites/default/files/resource-pdf/condoms-lubricants-covid19_en.pdf.
- Madiba S, Letsoalo B, Madiba S, Letsoalo B. Disclosure, Multiple Sex Partners, and Consistent Condom Use among HIV Positive Adults on Antiretroviral Therapy in Johannesburg, South Africa. World J AIDS [Internet]. 2014 Feb 26 [cited 2025 Jun 18];4(1):62–73. Available from: https://www.scirp.org/journal/paperinformation?paperid=43584.
- Ajayi AI, Ismail KO, Akpan W. Factors associated with consistent condom use: a cross-sectional survey of two Nigerian universities. BMC Public Health [Internet]. 2019 Sep 2 [cited 2025 Jun 18];19(1):1207. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6719351/.
- Wei C, Lim SH, Guadamuz TE, Koe S. HIV Disclosure and Sexual Transmission Behaviors among an Internet Sample of HIV-positive Men Who Have Sex with Men in Asia: Implications for Prevention with Positives. AIDS Behav [Internet]. 2012 Oct [cited 2025 Jun 15];16(7):1970. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3340458/.
- Ngure K, Mugo N, Celum C, Baeten JM, Morris M, Olungah O, et al. A Qualitative Study of Barriers to Consistent Condom Use among HIV-1 Serodiscordant Couples in Kenya. AIDS Care [Internet]. 2011 Apr 1 [cited 2025 Jun 15];24(4):509. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC3932299/.
- Thapa S, Ogunleye TT, Shrestha R, Joshi R, Hannes K. Increased Stigma, and Physical and Sexual Violence Against Men Who Have Sex with Men and Transgender Women in Sub-Saharan Africa: A Qualitative Evidence Synthesis Analyzing Social and Structural Barriers to HIV Testing and Coping Behaviors. J Homosex [Internet]. 2024 Jan 28 [cited 2025 Jun 15]; Available from: https://www.tandfonline.com/doi/pdf/10.1080/00918369.2024.2320237.
- Operario D, Sun S, Bermudez AN, Masa R, Shangani S, van der Elst E, et al. Integrating HIV and mental health interventions to address a global syndemic among men who have sex with men. lancet HIV [Internet]. 2022 Aug 1 [cited 2025 Jun 15];9(8):e574. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC7613577/.
Figure 1.
Service providers’ responses to interventions for consistent and correct use of condoms with condom-compatible lubricants among MSM in Ghana.
Figure 1.
Service providers’ responses to interventions for consistent and correct use of condoms with condom-compatible lubricants among MSM in Ghana.
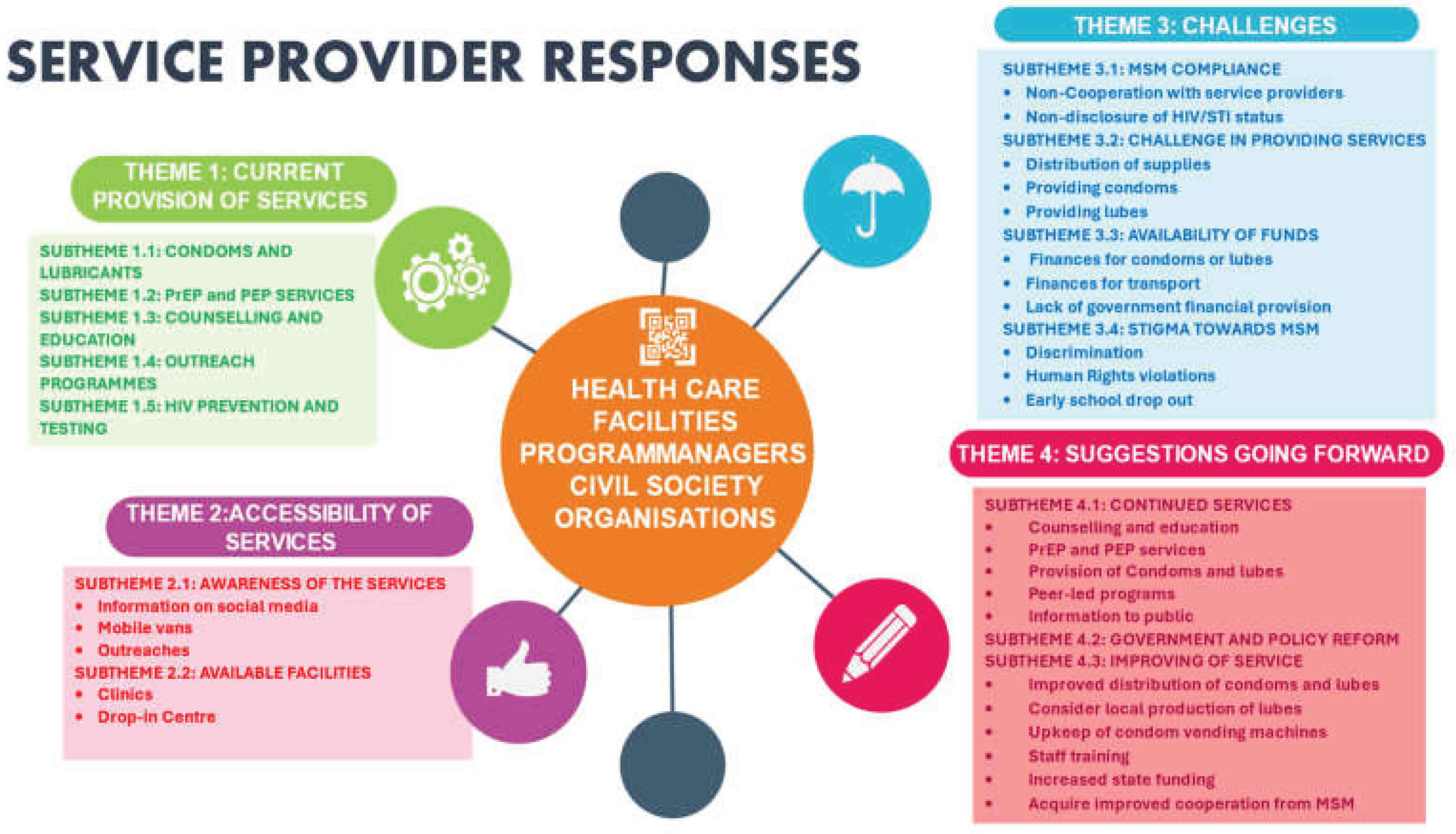
Figure 2.
The MSM responses to interventions/programmes for consistent and correct use of condoms with condom-compatible lubricants.
Figure 2.
The MSM responses to interventions/programmes for consistent and correct use of condoms with condom-compatible lubricants.
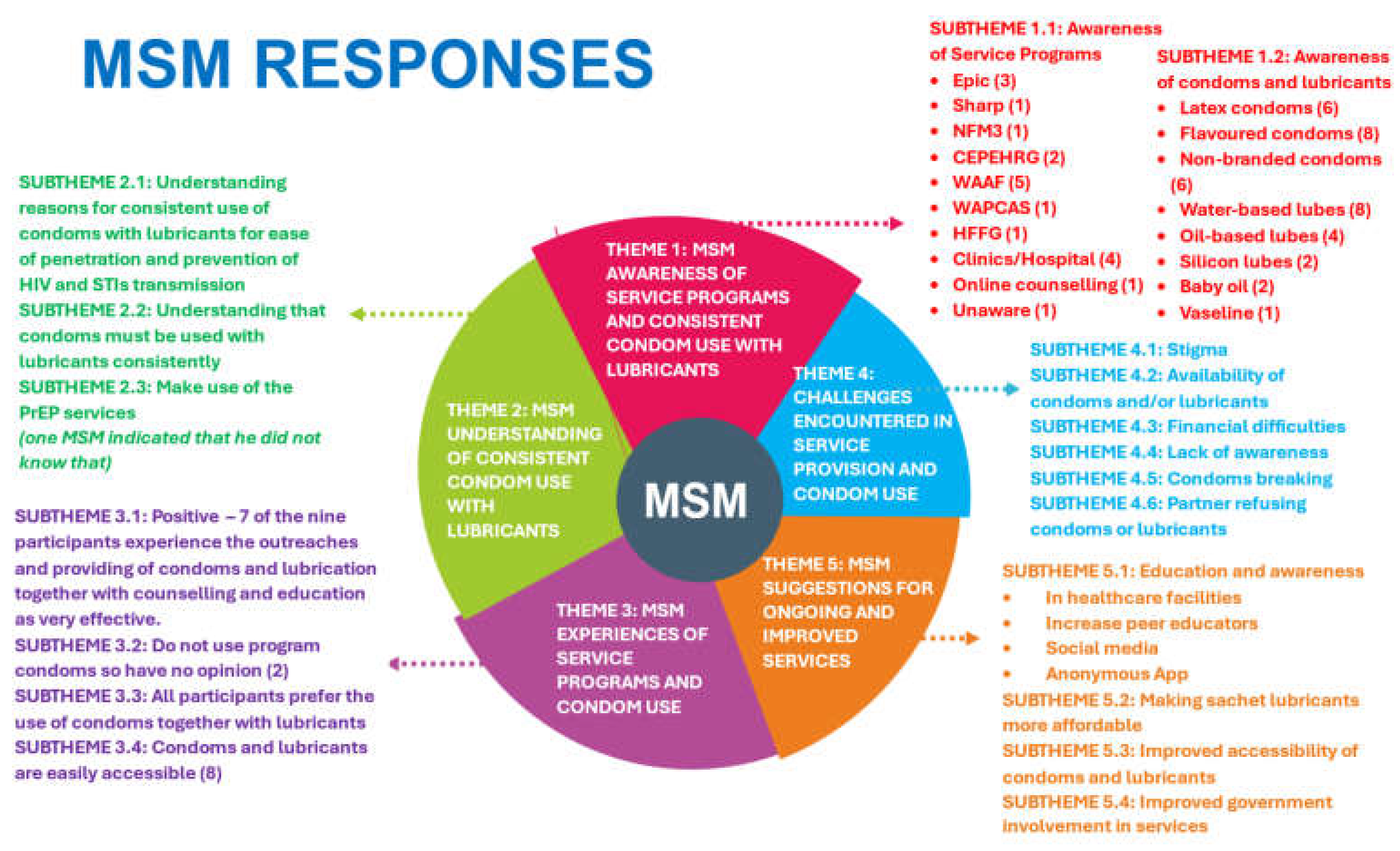

Table 1.
Criteria for inclusion and exclusion of the study participants.
| Participants | • MSM, HIV healthcare service providers, programme or technical coordinators, and programme managers from HIV-focused CSOs who provide MSM with interventions to ensure consistent and correct use of condoms with lubricants. |
| Inclusion criteria | • Healthcare workers, programme or technical coordinators, programme managers in HIV prevention, and aged eighteen years and above. • Individuals who provided informed consent to participate in the study. • Those working in the area of HIV prevention and care among Key populations for at least 1 year. • Those who could speak English or at least one local dialect. |
| Exclusion criteria | • Individuals who were below eighteen years old. • Individuals who did not give their consent to participate in the study. • Service providers with less than a year of experience in HIV control and prevention among key populations. • Individuals who could not speak English or at least one local dialect. |
Table 2.
Study Characteristics of the men who have sex with men and Service Providers.
| Service Providers and MSM respondents | Age | Gender/sexual orientation | Employment | Role |
| A | 28 | Gay | Self-employed | Buys and sells electrical appliances |
| B | 25 | Bisexual | National Service personnel | Internship |
| C | 21 | Gay | Unemployed | None |
| D | 30 | Gay | Employed | Insurance agent |
| E | 28 | Bisexual | Self-employed | Hairstylist |
| F | 30 | Queer | Employed | Operations manager |
| G | 26 | Gay | Employed | Event organiser on Social Media Marketer |
| H | 56 | Female | Employed | Data manager at the ART unit and a Counsellor. |
| I | 45 | Female | Employed | Public Health Nurse |
| J | 48 | Female | Employed | Clinical and Public Health Nurse |
| K | 50 | Female | Employed | Regional Technical Coordinator at the Technical Support Unit, Ghana AIDS Commission, Accra. |
| L | 52 | Female | Employed | Public Health Nurse |
| M | 39 | Male | Employed | Programme Manager |
| N | 31 | Female | Employed | Clinical Nurse |
| O | 29 | Female | Employed | Monitoring and Evaluation |
| P | 47 | Male | Employed | Regional Technical Coordinator, Ghana AIDS Commission, Accra. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



