
Submitted:
27 August 2025
Posted:
28 August 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
In individuals recently hospitalized with COVID-19, global estimates show a 17.9% prevalence of neuropsychiatric disorders. Cognitive behavioral therapy (CBT) is a viable alternative to reduce the harmful effects of the COVID-19 pandemic on mental health. This study aimed to verify the effect of CBT on anxiety, depression, post-traumatic stress disorder (PTSD), and quality of life (QOL) in hospitalized post-COVID-19 patients. This was a prospective clinical trial involving individuals with neuropsychiatric symptoms. Clinical data were collected, and the Hospital Anxiety and Depression Scale, Event Impact Scale (IES-6), and Short-Form Health Survey were administered. Fifteen patients (mean age 53.4 years), seven hospitalized in the COVID-19 ward and eight in the intensive care unit, underwent CBT sessions once a week for 50 min for a period of six weeks. The groups showed similar anxiety and depression scores (p>0.05) before and after CBT. However, there were significant intragroup differences in anxiety (p=0.01), depression (p=0.01), and PTSD (p=0.01) scores before and after CBT. Thus, CBT effectively reduced anxiety, depression, and PTSD, and improved QOL in post-COVID-19 patients.
Keywords:
post-traumatic stress disorder
; anxiety
; depression
; post-COVID-19
; psychotherapy
1. Introduction
In May 2021, the World Health Organization (WHO) declared the coronavirus disease 2019 (COVID-19) a pandemic as the number of confirmed cases worldwide reached 160 million [1]. According to the WHO (2022), of the 376,478,335 COVID-19 cases recorded by January 31, 2022, there were 5,666,064 lethal cases [2]. The pandemic has caused profound behavioral and economic changes in the society in different countries [3]. Generally, post-COVID-19 patients experience clinical, cognitive, emotional, and behavioral symptoms. Since the official report of the first COVID-19 outbreak in December 2019, several research groups have analyzed the neuropsychological impact of the disease [4,5].
Considering the individuals who were recently hospitalized with the coronavirus disease 2019 (COVID-19), global estimates show a 17.9% prevalence of neuropsychiatric disorders, with rates similar to those observed in survivors of Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS). The prevalent psychiatric disorders persisted for up to 12 months [3,6,7,8].
A recent study by Duru et al. (2023), involving individuals over 18 years of age who lived in Turkey during the COVID-19 pandemic period, showed a 31.9%, 45.3%, and 51.3% prevalence of post-traumatic stress disorder (PTSD), anxiety, and depression, respectively [9]. Furthermore, research has shown a 29.7% prevalence of anxiety and 68% of depression resulting from COVID-19 in Brazil [10], with higher prevalence among young women, individuals with lower educational levels, and those with pre-existing comorbidities, anxiety, and depressive disorders [11].
In a cross-sectional study with Brazilian patients, Hammerle et al. (2023) analyzed cognitive impairment, including anxiety and depression, associated with long-term COVID-19. The authors evaluated 127 post-COVID-19 patients; 53% of them reported subjective complaints of cognitive deficits, including anxiety and depression [12].
Some epidemiological data have shown that individuals hospitalized for extended periods due to COVID-19 are, the most affected by post-traumatic stress disorder (PTSD), anxiety, and depression [13,14]. According to the literature, sociodemographic characteristics, history of chronic disease (mental or physical), previous psychiatric morbidity, and type and intensity of trauma exposure are the main factors associated with triggering PTSD in post-COVID-19 patients [15,16].
The direct and/or indirect mechanisms underlying the psychiatric sequelae associated with COVID-19 are based on psychological stressors, inflammatory immune response to viral infection, and subsequent neuroinflammation induced by SARS-CoV-2 infection [17]. These findings suggest that peripheral changes, such as an increase in pro-inflammatory stimuli, can affect the central nervous system through humoral, neural, and cellular pathways, triggering mood disorders. Brain and glial cells also express angiotensin-converting enzyme 2 (ACE2) receptors, making them a potential target for viral infection via hematogenous or retrograde neuronal pathways [18].
Neuroplastic alterations, invasive medical procedures, limited ability to communicate, high drug consumption, and long hospital stays can exacerbate or consolidate symptoms associated with PTSD [19]. According to Rogers et al. (2020), 32.2% of critically ill patients who survived COVID-19 reported symptoms of PTSD, and 14.9% reported anxiety and depression [20]. In a cohort of 1276 individuals hospitalized with COVID-19, a significant increase in mood disorders was reported during the one-year follow-up, which negatively affected functional capacity [21].
In this context, cognitive-behavioral interventions can be viable alternatives to reduce or eliminate the harmful effects of the COVID-19 pandemic on mental health. Cognitive-behavioral therapy (CBT) consists of a brief and focused treatment that aims to modify dysfunctional responses, altering an individual's thoughts and behaviors, generally effective in the treatment of anxiety, depression, and PTSD associated with COVID-19 [22]. In line with the global pandemic scenario, this study aimed to verify the effects of brief therapy on PTSD, anxiety, depression, and QoL in patients after hospitalization for COVID-19.
2. Materials and Methods
2.1. Study Design and Participants
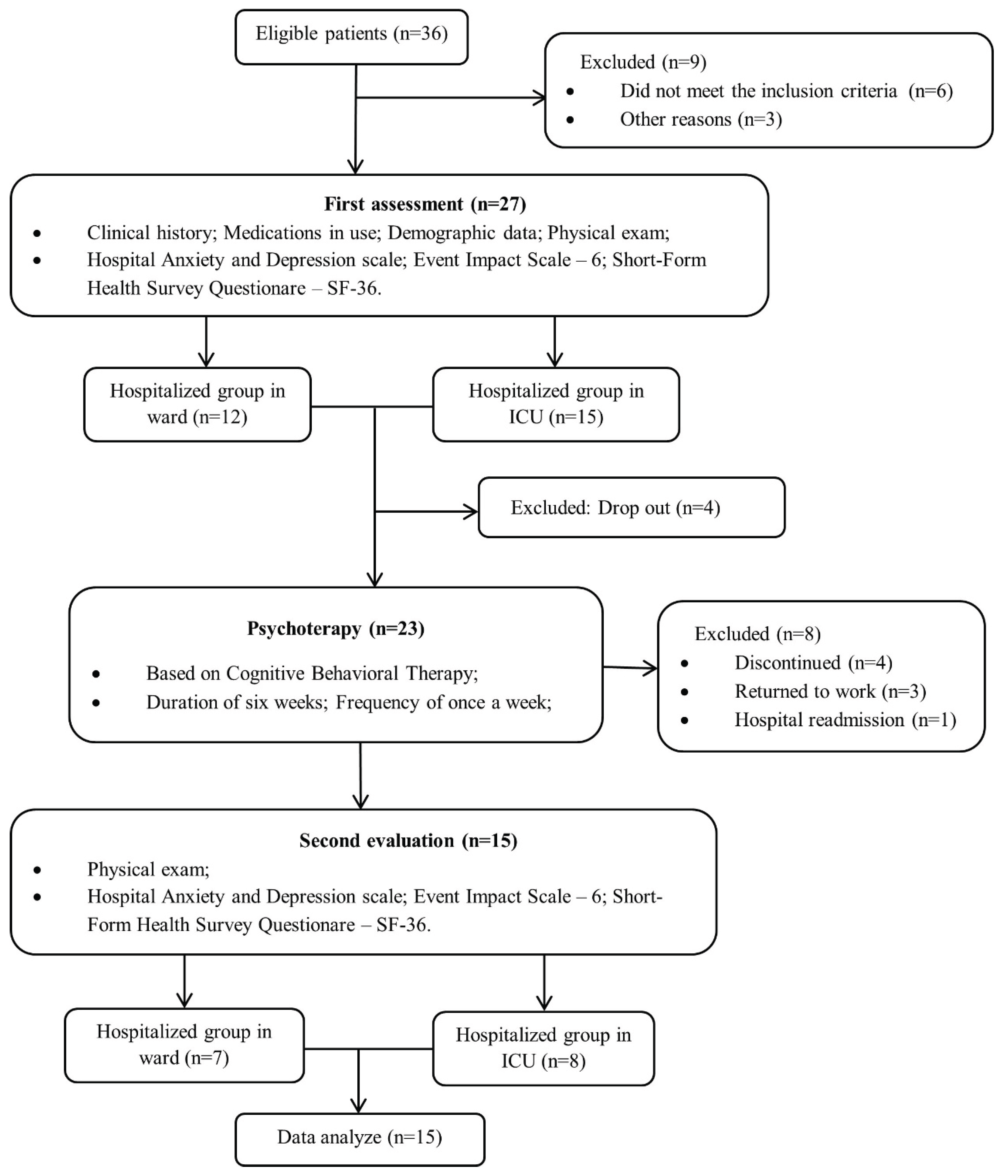
This was a clinical, prospective, and consecutive study carried out in a single center involving individuals affected by COVID-19 who were hospitalized. The study followed recommendations of the Transparent Reporting of Evaluations with Nonrandomized Designs (TREND), according to the flowchart shown in Fig. 1 [23]. Participants were recruited from May 2nd to December 2nd, 2021 through digital media, folders and posters distributed in reference hospitals for the treatment of COVID-19. All patients involved in the study had a clinical laboratory diagnosis of COVID-19 confirmed by polymerase chain reaction tests, according to the guidelines of the World Health Organization. In this study, the sample included both male and female individuals, aged between 18 and 75 years, clinically stable after clinical hospitalization for COVID-19 confirmed by clinical and laboratory diagnosis in a non-acute phase, and who had neuropsychiatric symptoms resulting from hospitalization. Patients who had prior psychiatric, neurological, or mood disorders were excluded from the present psychotherapy study. Due to the fact that there is no longer any demand for post-COVID-19 patients for psychological care in this service, the clinical trial was closed in February 2022.
2.2. Ethical Aspects
The study protocol was approved by the Research Ethics Committee of Universidade Evangelia de Goiás (process number 4,296,707) and was registered at Clinical Trials.org (NCT04982042). All participants who agreed to participate in the research gave written informed consent, after explaining all study procedures in a private environment.
2.3. Data Collection
This study was conducted at the Pulmonary Rehabilitation Laboratory of the Evangelical University of Goiás, located in the city of Anápolis (GO), Brazil. A clinical evaluation was performed prior to starting the psychotherapy sessions to collect sociodemographic data, pre-existing comorbidities, time and place of hospitalization, presence of symptoms of anxiety, depression, PTSD, and assessment of QoL. All data were collected on standardized forms for each outcome and stored in a database for further analysis. The following is a brief description of the data collection instruments used:
2.3.1. Hospital Anxiety and Depression Scale (HADS)
The HADS is an instrument used for assessing anxiety and depression in the scientific literature. It consists of 14 multiple-choice questions, comprising two subscales for anxiety and depression with seven items each. Each item is scored from zero (low) to three (high), totaling a score from 0 to 21. The severity of anxiety and depression can be classified as “normal” (0–7), mild (8–10), moderate (11–15), or severe (16–21).
The total score can also be used as a clinical indicator as long as it is analyzed as an index of emotional disturbance or stress [24].
Figure 1.
Study flowchart.
2.3.2. Event Impact Scale – IES-6
To assess PTSD, the Impact of Events Scale – 6 (IES-6) was used. This is an abbreviated version of the IES-R, a PTSD symptom screening tool with established validity and reliability for multiple types of trauma across multiple cultures. Despite containing only six items, the scale preserves the symptoms of the three sub-dimensions focused on in the original scale (intrusive, avoidance/blunting, and hypervigilance symptoms). The participants answered questions based on the previous seven days. In this study, to detect the presence of PTSD symptoms, a mean score of 1.09 or more was used as the cut-off score for significant stress [25].
2.3.3. Short-Form Health Survey – SF-36
QoL was assessed using the self-administered Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36). It is an instrument that is easy to apply and understand and is composed of 36 questions related to eight domains, four of which relate to the physical component of the QoL (functional capacity, physical aspects, pain, and general health status) and four related to the mental component (vitality, social aspects, emotional aspects, and mental health). Scores in each of these domains range from 0 to 100, with higher scores representing better QoL within the domain in question [26].
2.4. Psychological Intervention
CBT is recognized as a non-pharmacological treatment supported by strong evidence of its effectiveness in mitigating mental health problems. Therapy is based on the cognitive model, which supports the hypothesis that emotions, behaviors, and physiology are influenced by individuals' perceptions of events [27].
In this study, a specialist psychologist applied CBT once a week for the duration of six weeks in 50-minute sessions. The cognitive-behavioral interventions used were psychoeducation, identification of automatic thoughts and emotions, identification of central and intermediate beliefs, cognitive restructuring, problem-solving, and process evaluation. These interventions aimed to help patients detect and react to dysfunctional thoughts, promote a better emotional state and adaptive behavior to their environment, seek to strengthen resilience, and improve satisfaction and general well-being [27].
All sessions were structured following the standard CBT model with individualized treatment plans, goals, and action plans [28]. Upon completing the six weeks of therapy, the patients were reassessed and then oriented and/or released.
2.5. Statistical Analysis and Sample Size
For continuous variables, the mean and standard deviation of the mean or median and interquartile range (IQR) were used in the descriptive analysis. Data normality was verified using the Shapiro-Wilk test. For ordinal variables with no normal distribution, the Mann–Whitney U test or Wilcoxon test was used, and for those with normal data distribution, the Student’s t-test was used. Descriptive analyses were performed for categorical variables presented in absolute and relative frequencies. Comparisons were performed using the chi-squared test or Fisher's exact test. To compare the frequencies of the same population for two points in time, the McNemar test was performed. The significance level adopted for all tests was 5%. STATA ® software (version 17.0) was used for the statistical analysis. As for the sample size calculation, due to not finding a similar previously published study, the criterion of convenience sampling was adopted according to the principle “intention-to-treat.” In this study, the researchers involved in data analysis were blind to the composition of the different patient groups.
3. Results
From an initial sample consisting of 21 subjects with a confirmed diagnosis of COVID-19, this study included seven patients who were hospitalized in the ward (WG) and eight in the intensive care unit (ICUG), totaling 15 patients involved in the final analysis. The mean age of the patients was 53.4 years (WG = 54.9 and ICUG = 51.7). No significant differences were observed between the groups in terms of age, sex, self-reported race, educational status, comorbidities, length of hospitalization, anxiety, or depression (Table 1).
Before the intervention, four ICUG patients had a possible diagnosis of depression, and two had anxiety. No significant differences were observed in symptoms of anxiety, depression, and PTSD before and after the psychotherapeutic intervention, as well as differences between the pre- and post-intervention groups (Table 2).
Before and after the psychotherapeutic intervention, the anxiety and depression scores were similar between the groups (p>0.05). However, there were significant intragroup differences in anxiety (p=0.01), depression (p=0.01), and PTSD (p=0.01) scores before and after the psychotherapeutic intervention (Table 3).
According to Table 4, in the QOL assessment, it can be observed that after the psychotherapeutic intervention, ICUG patients showed significant improvement in their functional capacity, physical aspects, vitality, emotional aspects, and mental health domains. Similarly, individuals who were hospitalized in the ward showed improvements in their general and mental health constructs. No significant difference was observed between the groups in terms of variations in post-intervention scores.
4. Discussion
In this study, no significant differences were found between the groups in terms of age, sex, self-reported race, comorbidities, and length of hospitalization. The results showed a similarity between WG and ICUG patients, where approximately half of the sample presented symptoms of anxiety, depression, and PTSD. This rate was higher than that reported in a recent meta-analysis involving 31 studies, in which the prevalence of anxiety and depression symptoms among post-COVID-19 patients was 47% and 45%, respectively [29]. A retrospective study of 402 COVID-19 survivors showed that 56% of patients had at least one psychiatric disorder (Mazza et al., 2020) [30], which corresponds with the findings of a review that demonstrated a high prevalence of PTSD, anxiety, and depression in this population [31]. A 6-month follow-up study also reported that 57.3% of patients without previous psychiatric history developed a mental disorder after hospitalization for COVID-19 [32].
In the study conducted by Vlake et al. (2021), 294 patients (average age of 64 years, 36% female) post-COVID-19 were evaluated after one and three months of hospital discharge. Of these, 16% and 13% reported positive symptoms for PTSD, 29% and 20% for anxiety and 32% and 24% for depression symptoms, respectively in the first and second assessment. Patients who required ICU admission reported symptoms of depression less frequently, however, no significant differences were observed in relation to PTSD, anxiety and/or general HRQoL [33].
The discrepancy in the prevalence of neuropsychiatric symptoms in COVID-19 survivors is partially due to the study design, heterogeneity of the population involved, variety of instruments, and cut-off points used in the assessment [29].
A study conducted by Li et al. (2021) showed that patients aged between 46 and 60 years had a higher proportion of symptoms of anxiety and depression assessed by the HADS during hospitalization for COVID-19. It was also observed that patients hospitalized for more than 14 days had a higher risk of depressive symptoms than those hospitalized for less than seven days. Another interesting finding was the verification of a significant positive correlation between HADS scores, indicating that in post-COVID-19 patients, symptoms of anxiety and depression were interconnected [34].
A case-control study by Azizi et al. (2022) reported similar results. The authors reported that COVID-19 survivors had higher levels of anxiety and depression (HADS-A = 12.84; HADS-D = 10.91) than the control group (HADS-A = 9.90; HADS-D = 8.27), proving that a longer hospital stay and the severity and duration of COVID-19 symptoms were among the most important predictors of worsening mental health [4].
On the other hand, in the study by Olgun et al. (2023) 283 patients were involved, divided into a post-COVID-19 group (n=144) and a control group (n=139). The post-COVID-19 group was evaluated approximately one month after infection and of these, 89 (61.8%) of the 144 were hospitalized. When analyzing the results of the HADS questionnaire, the average score was 13 in post-COVID-19 cases and nine in the control group (p<0.001), values considered lower than those found in the present study. When analyzing the anxiety and depression subgroups, both results were significant in post-COVID patients when compared to the control group (p<0.001 and p=0.022, respectively). When comparing the hospitalization status of patients with COVID-19, no significant difference was observed in the aspect of anxiety (p=0.23), however depression (p<0.024) was more prevalent in hospitalized patients [35].
The study by Khatun and Farhana (2023) only evaluated signs of depression in 325 patients recovered from COVID-19. The authors observed that the largest proportion of the sample was aged between 46 and 55 years (23.1%), with 61.5% being male. Of the patients evaluated, 31% showed signs of depression, 26.7% being mildly depressed, 2.5% extremely depressed and 1.2% severely depressed. The level of depression in patients involved in the study was significant when associated with diabetes mellitus, duration of hospitalization, social distancing, social media posts about COVID-19, job loss, family financial losses and fear of reinfection [36]. Potential risk factors described in the literature also include female sex, a high prevalence of symptoms, presence of comorbidities, age, prolonged hospitalization, administration of sedatives, functional changes and patients from low-income countries [37,38].
In addition, unique pandemic elements can affect survival outcomes, including rampant circulation of misinformation, bed shortages, ICU stays, use of mechanical ventilation, treatment-related neglect in health facilities, lack of family presence in the hospital, limited post-acute care rehabilitation, and widespread economic recession, as well as uncertainty about disease prognosis and adverse outcomes [39].
Regarding the triggering of PTSD in post-COVID-19 patients, the main associated factors consist of sociodemographic characteristics, previous psychiatric morbidity, and type and intensity of trauma exposure [15]. According to the Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5), experiencing repeated or extreme exposure to aversive details of traumatic events can be potentially aggravating, such as the COVID-19 pandemic outbreak, owing to its acute and chronic implications for both individual and community [40].
A recent systematic review identified that PTSD symptoms usually persist for more than three months after the disease has resolved. According to the study, in 36.4% of patients, symptoms were present within two months of hospitalization, and 5.9% within three to four months of hospitalization. Severe PTSD symptoms were consistent in 5.9% of survivors, 11.3% exhibited moderate symptoms, and 25.6% exhibited mild symptoms [41,42]. The cause of these symptoms correlates with infection through direct and indirect mechanisms; however, the underlying etiology seems more complex and multifactorial, involving environmental, psychological, and biological factors [42].
Another systematic review also showed that trauma-focused therapies are more effective than pharmacological interventions for the treatment of PTSD [43]. This result is supported by other researchers, who detected more significant improvements among individuals treated with a psychotherapeutic approach than those treated with pharmacological therapy [44].
Regarding QoL, which refers to the level of well-being perceived by the individual in the different domains of their life and their impact on general health, a review study demonstrated the effects of hospitalization as a potential agent for the decline of QoL [45]. Theref ore, the data from this study showed that individuals who were hospitalized in the ward and the ICU showed a significant improvement in the mental health domain after the psychological intervention. These findings indicate that regardless of the severity of the disease, levels of anxiety and stress can be reduced gradually over time with the use of psychotherapy [13].
An interesting study by Hu et al. (2021) involving 90 hospitalized patients diagnosed with COVID-19 at the General Hospital in Wuhan, China, assessed HRQoL, anxiety, depression, and physical activity levels. The authors concluded that after hospital discharge, patients with COVID-19 had negative emotional symptoms, such as anxiety and/or depression, as well as HRQoL impairments, primarily in female patients, compared with the control group. Based on their observations, the authors suggested that patients hospitalized for COVID-19 should be referred to mental health and physical rehabilitation programs to improve their psychological state and functional capacity, and, consequently, their HRQoL [46].
Gutiérrez-Canales et al. (2022) performed a cross-sectional study evaluating HRQoL, using the SF-36, in a sample of 206 Latin American patients hospitalized for COVID-19. Most of the patients (73.3%) had persistent symptoms such as fatigue (36.9%), anxiety (26.2%), and headache (24.8%) [47]. In addition, a large cross-sectional study including 422 patients aged 30–75+ found high prevalence and severity of depressive and anxiety symptoms, reinforcing the need for targeted mental health interventions in COVID-19 survivors [48]. As in the study by Hu et al. (2021), female sex was associated with an increased risk of persistent symptoms (OR=2.95, 95%CI 1.56–5.57). The authors concluded that a high percentage of patients hospitalized for COVID-19 had persistent anxiety and depression symptoms and impaired HRQoL. Based on these results, it is important consider referring these patients to psychological therapy and physical rehabilitation to improve their quality of life, while finding a better way to treat “long COVID” [46].
Similar results were reported by Munoz-Corona et al. (2022), who evaluated COVID-19 symptoms and HRQoL in 141 post-SARS-CoV-2 patients 90 days after hospital discharge. Most of the patients (75.9%) reported persistent fatigue and arthralgia and had low HRQoL scores, as assessed by the SF-36, compared with patients who did not have symptoms [49]. Koullias et al. (2022) also evaluated HRQoL six months after hospital discharge in a sample of 151 Greek patients hospitalized for COVID-19. They found that hospitalized patients had significant HRQoL impairments compared with patients with mild COVID-19 and healthy controls. According to the authors, physical impairment and psychological stress caused by severe COVID-19 symptoms represented considerable health impairment, especially for women and people aged 41 to 60 years, even six months after hospitalization for COVID-19 [50].
HRQoL assessed by the SF-36 was also significantly reduced in post-COVID patients assessed approximately seven months after hospital discharge [51]. Poudel et al. (2021) also observed that the impact of COVID-19 on HRQoL was considered relevant both in patients with acute Covid and in patients with Long Covid [38]. The study by Bolgeo et al. (2023) included 199 patients evaluated approximately 4 months after hospital discharge. Of these, 145 were followed up for 8 months after the infection and it was observed that the patients' quality of life worsened over time, especially in terms of mobility (27.6%) and pain (31%). The authors also found a positive correlation between COVID-19 symptoms and comorbidities present at admission, in addition to an inadequate perception of quality of life, thus reinforcing the need for these patients to be included in a physical and psychological rehabilitation program, in accordance with the improvement results observed in the present study [52].
In a prospective cohort study, Wiertz et al. (2022) evaluated the recovery of 67 post-COVID-19 patients (mean age: 62 years; 78% male) during the first year after intensive care unit (ICU) discharge. In addition to checking for different physical and functional functions, the authors also assessed the levels of depression, anxiety, and post-traumatic stress (Global Psychotrauma Screen-Post-Traumatic Stress Disorder), and changes in cognitive functioning after admission to the ICU. The results showed that, at a one-year follow-up, 50% of the patients had not resumed their work activities, and showed restrictions in the practice of physical activities (51%), housework (46%), and leisure activities (29%). The authors pointed out that self-reported complaints of shortness of breath and fatigue, perceived limitations in activities of daily living, a less proactive coping style, and the presence of anxiety/depression were associated with slower recovery [53]. Similar findings were observed in a 12-month ICU follow-up study, which associated psychosomatic, respiratory, and neurocognitive sequelae with persistent depression, anxiety, fatigue, and sleep disturbances [54].
Mazurek et al. (2022) drew attention to the fact that the COVID-19 pandemic had spread rapidly worldwide, generating considerable significant negative economic and psychosocial consequences and contributing to mental health impairment. Although COVID-19 primarily compromises physical health, it is important to consider its secondary effects on patients’ mental health [55].
According to Koullias et al. (2022), the COVID-19 pandemic caused a secondary epidemic among survivors, which needs to be addressed using a multidisciplinary approach before it entails a high cost for public health systems in different countries. These patients should be screened for physical rehabilitation programs and psychological treatment for complete physical, functional, and HRQoL recovery [50].
The effect of the psychological impact caused by outbreaks of pandemic diseases demonstrates the relevance of evidence-based psychological intervention in coping, understanding that these demands tend to change over the course of the disease or the occurrence of related factors. Regarding psychological support, this study found that CBT resulted in a reduction in anxiety and depression scores and improved QoL in WG and ICUG patients.
The results of this study revealed that individuals who had been hospitalized in the COVID-19 ward and ICU showed significant improvement in the mental health domain after receiving psychological intervention. The significant improvement presented in the patients was possibly due to the orientation of identifying and reorganizing events that could interfere with their mood and daily behaviors, as well as creating coping strategies to deal with the sequelae resulting from COVID-19. These findings correspond with those reported in a cohort of Chinese patients whose therapeutic effect was associated with a significant reduction in behavioral changes [56]. Asimakos et al. (2023) also investigated the effects of an 8-week rehabilitation program and observed that patients significantly improved anxiety, depression and PTSD symptomatology, which is similar to the results of the present study, while patients in usual care remained without showing significant improvements [57].
These psychotherapeutic approach strategies were developed through planning new daily activities, which not only promoted an improvement in mood but were also compatible with the physical condition of the patients. The functional capacity, vitality, and mental health dimensions evaluated using the SF-36 questionnaire showed significant improvement between the groups. These results suggest that the control of neuropsychiatric symptoms is a predictor of functional abilities and physical symptoms [22].
When analyzed together, these factors point to the relevance of psychological interventions aligned with emerging needs in the current pandemic context. Consequently, cognitive restructuring of CBT applied to dysfunctional symptoms can help in the treatment of patients hospitalized with COVID-19. Song et al. (2021) found a significant reduction in levels of anxiety, depression, and stress in patients who tested positive for COVID-19 and who underwent a CBT protocol compared with the group of patients who only underwent routine treatment following the guidelines for disease management [22].
Psychotherapy allows post-COVID-19 patients to reframe their life experiences and trauma, resulting in improved relationships, creating new possibilities, increasing emotional stability, and increased valuation of life [58]. In addition, interdisciplinary collaboration between health experts and specialized post-COVID-19 rehabilitation centers should be made available to enhance the management of persistent symptoms, knowing that interventions aimed at improving patients' mental health can play a role in enhancing patients' QoL [59].
It is important to highlight that mental health is a key component of collective and individual ability. Therefore, the promotion, protection, and restoration of mental health are vital to individuals, communities, and societies around the world [60]. Social support is also an important influencing factor that can increase the self-esteem of individuals, alleviate persistent unpleasant or stressful emotions, and make life more meaningful, protecting individuals from psychological distress and promoting positive changes after traumatic events [61].
In line with the findings of this study, the results of a randomized clinical trial demonstrated reduced rates of anxiety, depression, and stress after CBT treatment. The authors highlighted that the psychotherapeutic approach was more effective in patients with chronic diseases who were hospitalized in the ICU [62]. Other studies have also proven the effectiveness of CBT in preventing psychiatric disorders in individuals at risk, such as PTSD, anxiety, and depression [63,64,65].
An interesting study conducted by Garcia-Molina et al. (2022) verified the results of an outpatient neuropsychological intervention program involving 123 post-COVID-19 patients (mean age: 51 years). The patients underwent pre- and post-participation cognitive behavioral assessments in an outpatient post-COVID-19 neurorehabilitation program, including respiratory and motor physiotherapy and neuropsychological rehabilitation. After the initial neuropsychological evaluation, 91 patients (74%) presented with cognitive impairment and underwent psychological intervention. The authors concluded that neuropsychological intervention was an effective tool to treat cognitive-emotional deficits in the post-COVID-19 syndrome. However, they highlighted the fact that not all patients attained their pre-COVID-19 functional levels, six months after the end of treatment [5].
Rutkowski et al. (2022) conducted an in-hospital pulmonary rehabilitation program (PRP) with virtual reality components, involving 32 post-COVID-19 patients in a public hospital in Poland. PRP includes aerobic training, respiratory function, resistance, and relaxation activities. The authors assessed exercise tolerance, anxiety, depression (HADS), and HRQoL (WHOQOL-BRIEF), and concluded that the 3-week in-hospital PRP significantly improved exercise tolerance, reduced anxiety and depressive symptoms, and consequently improved HRQoL. The study highlighted the importance of including relaxation activities and psychotherapy in the therapeutic approach for post-COVID-19 patients [66].
Therefore, early interventions are crucial to combat the growing psychiatric manifestations in post-COVID-19 patients, aiming to improve the functional capacity and QoL of affected people, in addition to reducing the chances of developing neurocognitive deficiencies. It is thus essential to develop strategies for cognitive and behavioral changes in the face of the situation experienced during the period of isolation, treatment in a hospital environment, and/or in the ICU, which can contribute to healing traumas related to fear of death, reducing negative beliefs that may make treatment after hospital discharge difficult, impotence, and irritability in the face of events.
As a limitation of this study, we draw attention to the fact that the study was carried out in a single center, and the sample size was small, which limits the generalizability of the results. However, it is important to highlight that after conducting a few sessions, a considerable number of patients dropped out of the study due to showing significant improvement.
5. Conclusions
According to our data, CBT was effective in reducing levels of anxiety and depression as well as improving the QoL of post-COVID-19 patients. These findings must be considered by future studies involving a greater number of patients and followed-up for a longer period of time, aiming to establish criteria for the diagnosis, assess the severity and frequency of the observed manifestations, and propose intervention strategies for the individual and/or population to alleviate the suffering caused by COVID-19.
Author Contributions
Conceptualization, M.M.C., M.C.O., L.V.F.O and H.N.C.P.; methodology, L.R.A. and J.P.R.A.; software, R.P.V. and R.A.C.A.; validation, H.N.C.P., L.R.A., R.K.P. and I.O.S; formal analysis, R.K.P., R.F.O., D.A.A.P.O., G.C, P.C., and C.H.M.S.; investigation, M.M.C., M.C.O., W.A.O.C and L.R.A.; resources, L.R.A. and L.V.F.O.; data curation, R.P.V. and R.A.C.A.; writing—original draft preparation, L.V.F.O., M.M.C. and M.C.O.; writing—review and editing, , M.M.C., J.P.R.A., L.V.F.O. and M.C.O.; visualization, I.O.S, G.C, P.C., C.H.M.S. W.A.O.C, R.F.O. and D.A.A.P.O.; supervision, L.V.F.O, L.R.A. and R.P.V.; project administration, L.V.F.O.; funding acquisition, M.M.C. and L.V.F.O. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. LVFO received grants from Research Productivity, modality PQII; process no. 310241/2022-7 of Conselho Nacional de Desenvolvimento Cientifico e Tecnologico (local acronym CNPq), Brazil. RPV receive grants Research Productivity, modality PQII; process no. 313299/2018-8 of Conselho Nacional de Desenvolvimento Cientifico e Tecnologico (local acronym CNPq), Brazil. MCO and, JPRA receives a grant from the Fundação de Amparo a Pesquisa do Estado de Goias (FAPEG), (GO), Brazil. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Research Ethics Committee of Universidade Evangelica de Goiás (process number 4,296,707) and was registered at Clinical Trials.org (NCT04982042).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study will be made available upon request to the corresponding author due to ethical restrictions.
Acknowledgments
The authors would like to thank all the patients involved in this study and the Pulmonary Rehabilitation Laboratory at Evangelical University of Goiás - UniEVANGELICA and Fundação de Amparo a Pesquisa do Estado de Goiás - FAPEG who allowed this study to be conducted.
Conflicts of Interest
The authors declare that they have no conflict of interest.
References
- World Health Organization. WHO coronavirus (COVID-19) dashboard. 2021. Available online: https://covid19.who.int (accessed on 20 Oct 2024).
- World Health Organization. Diagnostic testing for SARS-CoV-2: Interim guidance. COVID-19: Laboratory and diagnosis. 2022. Available online: https://www.who.int/publi cations/i/item/diagnostic-testing-for-sars-cov-2 (accessed on 20 Oct 2024).
- Jung G, Ha JS, Seong M, Song JH. The Effects of Depression and Fear in Dual-Income Parents on Work-Family Conflict During the COVID-19 Pandemic. Sage Open. 2023, 13, 21582440231157662. [CrossRef]
- Azizi A, Achak D, Saad E, Hilali A, Youlyouz-Marfak I, Marfak A. Post-COVID-19 mental health and its associated factors at 3-months after discharge: A case-control study. Clin Epidemiol Glob Health. 2022, 17, 101141. [CrossRef]
- García-Molina A, García-Carmona S, Espiña-Bou M, Rodríguez-Rajo P, Sánchez-Carrión R, Enseñat-Cantallops A. Neuropsychological rehabilitation for post-COVID-19 syndrome: results of a clinical programme and six-month follow up. Neurologia (Engl Ed). 2022, 39, 592-603. [CrossRef]
- Lee AM, Wong JG, McAlonan GM, Cheung V, Cheung C, Sham PC, et al. Stress and psychological distress among SARS survivors 1 year after the outbreak. Can J Psychiatry. 2007, 52, 233-40. [CrossRef]
- Lee SH, Shin HS, Park HY, Kim JL, Lee JJ, Lee H, et al. Depression as a Mediator of Chronic Fatigue and Post-Traumatic Stress Symptoms in Middle East Respiratory Syndrome Survivors. Psychiatry Investig. 2019, 16, 59-64. [CrossRef]
- Zeng N, Zhao YM, Yan W, Li C, Lu QD, Liu L, et al. A systematic review and meta-analysis of long term physical and mental sequelae of COVID-19 pandemic: call for research priority and action. Mol Psychiatry. 2023, 28, 423-433. [CrossRef]
- Altundal Duru H, Yılmaz S, Yaman Z, Boğahan M, Yılmaz M. Individuals' Coping Styles and Levels of Depression, Anxiety, and Stress During the COVID-19 Pandemic in Turkey: A Web-Based Cross-Sectional Study. Sage Open. 2023, 13, 21582440221148628. [CrossRef]
- Filgueiras A, Stults-Kolehmainen M. Risk Factors for Potential Mental Illness Among Brazilians in Quarantine Due To COVID-19. Psychol Rep. 2022, 125, 723-741.
- Bellan M, Soddu D, Balbo PE, Baricich A, Zeppegno P, Avanzi GC, et al. Respiratory and Psychophysical Sequelae Among Patients With COVID-19 Four Months After Hospital Discharge. JAMA Netw Open. 2021, 4, e2036142. [CrossRef]
- Hammerle MB, Sales DS, Pinheiro PG, Gouvea EG, de Almeida PIFM, de Araujo Davico C, et al. Cognitive Complaints Assessment and Neuropsychiatric Disorders After Mild COVID-19 Infection. Arch Clin Neuropsychol. 2023, 38, 196-204. [CrossRef]
- Huang L, Li X, Gu X, Zhang H, Ren L, Guo L, et al. Health outcomes in people 2 years after surviving hospitalisation with COVID-19: a longitudinal cohort study. Lancet Respir Med. 2022, 10, 863-876. [CrossRef]
- Taquet M, Geddes JR, Husain M, Luciano S, Harrison PJ. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: a retrospective cohort study using electronic health records. Lancet Psychiatry. 2021, 8, 416-427. [CrossRef]
- Al-Jassas HK, Al-Hakeim HK, Maes M. Intersections between pneumonia, lowered oxygen saturation percentage and immune activation mediate depression, anxiety, and chronic fatigue syndrome-like symptoms due to COVID-19: A nomothetic network approach. J Affect Disord. 2022, 297, 233-245. [CrossRef]
- Akova İ, Kiliç E, Özdemir ME. Prevalence of Burnout, Depression, Anxiety, Stress, and Hopelessness Among Healthcare Workers in COVID-19 Pandemic in Turkey. Inquiry. 2022, 59, 469580221079684. [CrossRef]
- Bortolato B, Carvalho AF, Soczynska JK, Perini GI, McIntyre RS. The Involvement of TNF-α in Cognitive Dysfunction Associated with Major Depressive Disorder: An Opportunity for Domain Specific Treatments. Curr Neuropharmacol. 2015, 13, 558-76. [CrossRef]
- Ou X, Liu Y, Lei X, Li P, Mi D, Ren L, et al. Characterization of spike glycoprotein of SARS-CoV-2 on virus entry and its immune cross-reactivity with SARS-CoV. Nat Commun. 2020, 11, 1620. [CrossRef]
- Badenoch J, Cross B, Hafeez D, Song J, Watson C, Butler M, et al. Post-traumatic symptoms after COVID-19 may (or may not) reflect disease severity. Psychol Med. 2023, 53, 295-296. [CrossRef]
- Rogers JP, Chesney E, Oliver D, Pollak TA, McGuire P, Fusar-Poli P, et al. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry. 2020, 7, 611-627. [CrossRef]
- Huang L, Yao Q, Gu X, Wang Q, Ren L, Wang Y, et al. 1-year outcomes in hospital survivors with COVID-19: a longitudinal cohort study. Lancet. 2021, 398, 747-758. [CrossRef]
- Song J, Jiang R, Chen N, Qu W, Liu D, Zhang M, et al. Self-help cognitive behavioral therapy application for COVID-19-related mental health problems: A longitudinal trial. Asian J Psychiatr. 2021, 60, 102656. [CrossRef]
- Des Jarlais DC, Lyles C, Crepaz N; TREND Group. Improving the reporting quality of nonrandomized evaluations of behavioral and public health interventions: the TREND statement. Am J Public Health. 2004, 94, 361-6. PMID: 14998794; PMCID: PMC1448256. [CrossRef]
- Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983, 67, 361-70. [CrossRef]
- Hosey MM, Leoutsakos JS, Li X, Dinglas VD, Bienvenu OJ, Parker AM, et al. Screening for posttraumatic stress disorder in ARDS survivors: validation of the Impact of Event Scale-6 (IES-6). Crit Care. 2019, 23, 276. [CrossRef]
- Ware JE Jr, Sherbourne CD. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992, 30, 473-83.
- Beck JS. Terapia cognitivo-comportamental: Teoria e prática. Porto Alegre: Artmed. 2013.
- Beck JS, Knapp P. Terapia cognitivo-comportamental: Teoria e prática. 3ª ed. Porto Alegre: Artmed. 2021.
- Deng J, Zhou F, Hou W, Silver Z, Wong CY, Chang O, et al. The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: a meta-analysis. Ann N Y Acad Sci. 2021, 1486, 90-111. [CrossRef]
- Mazza MG, De Lorenzo R, Conte C, Poletti S, Vai B, Bollettini I, et al. Anxiety and depression in COVID-19 survivors: Role of inflammatory and clinical predictors. Brain Behav Immun. 2020, 89, 594-600. [CrossRef]
- Carrijo M, Oliveira MC, Oliveira AC, Lino MEM, Souza SKA, Afonso JPR, et al. Post-traumatic stress disorder, anxiety and depression in post-COVID19 patients: integrative review. Mtprehabjournal. 2022, 20, 1–10. [CrossRef]
- Chamorro-Delmo J, Portillo De-Antonio P, Porras-Segovia A, de León-Martínez S, Figuero Oltra M, del Pozo-Herce P, Sánchez-Escribano Martínez A, Abejón Pérez I, Vera-Varela C, Postolache TT, et al. Onset of mental disorders following hospitalization for COVID-19: a 6-month follow-up study. COVID. 2023, 3, 218-225. [CrossRef]
- Vlake JH, Wesselius S, van Genderen ME, van Bommel J, Boxma-de Klerk B, Wils EJ. Psychological distress and health-related quality of life in patients after hospitalization during the COVID-19 pandemic: A single-center, observational study. PLoS One. 2021, 16, e0255774. [CrossRef]
- Li X, Tian J, Xu Q. The Associated Factors of Anxiety and Depressive Symptoms in COVID-19 Patients Hospitalized in Wuhan, China. Psychiatr Q. 2021, 92, 879-887. [CrossRef]
- Olgun Yıldızeli S, Kocakaya D, Saylan YH, Tastekin G, Yıldız S, Akbal Ş, et al. Anxiety, Depression, and Sleep Disorders After COVID-19 Infection. Cureus. 2023, 15, e42637. [CrossRef]
- Khatun K, Farhana N. Assessment of Level of Depression and Associated Factors among COVID-19-Recovered Patients: a Cross-Sectional Study. Microbiol Spectr. 2023, 11, e0465122. [CrossRef]
- Grasselli G, Zangrillo A, Zanella A, Antonelli M, Cabrini L, Castelli A, et al. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020, 323, 1574-1581. [CrossRef]
- Poudel AN, Zhu S, Cooper N, Roderick P, Alwan N, Tarrant C, et al. Impact of Covid-19 on health-related quality of life of patients: A structured review. PLoS One. 2021, 16, e0259164. [CrossRef]
- Xiang YT, Yang Y, Li W, Zhang L, Zhang Q, Cheung T, et al. Timely mental health care for the 2019 novel coronavirus outbreak is urgently needed. Lancet Psychiatry. 2020, 7, 228-229. [CrossRef]
- First MB. Diagnostic and statistical manual of mental disorders, 5th edition, and clinical utility. J Nerv Ment Dis. 2013, 201, 727-9. [CrossRef]
- Bonazza F, Borghi L, di San Marco EC, Piscopo K, Bai F, Monforte AD, et al. Psychological outcomes after hospitalization for COVID-19: data from a multidisciplinary follow-up screening program for recovered patients. Res Psychother. 2021, 23, 491. [CrossRef]
- Shanbehzadeh S, Tavahomi M, Zanjari N, Ebrahimi-Takamjani I, Amiri-Arimi S. Physical and mental health complications post-COVID-19: Scoping review. J Psychosom Res. 2021, 147, 110525. [CrossRef]
- Coventry PA, Meader N, Melton H, Temple M, Dale H, Wright K, et al. Psychological and pharmacological interventions for posttraumatic stress disorder and comorbid mental health problems following complex traumatic events: Systematic review and component network meta-analysis. PLoS Med. 2020, 17, e1003262. [CrossRef]
- Merz J, Schwarzer G, Gerger H. Comparative Efficacy and Acceptability of Pharmacological, Psychotherapeutic, and Combination Treatments in Adults With Posttraumatic Stress Disorder: A Network Meta-analysis. JAMA Psychiatry. 2019, 76, 904-913. [CrossRef]
- Oliveira MC, Carrijo MM, Afonso JPR, Moura RS, Oliveira LFRJ, Fonseca AL, et al. Effects of hospitalization on functional status and health-related quality of life of patients with COVID-19 complications: a literature review. Mtprehabjournal. 2022, 20. [CrossRef]
- Hu J, Zhang Y, Xue Q, Song Y, Li F, Lei R, et al. Early Mental Health and Quality of Life in Discharged Patients With COVID-19. Front Public Health. 2021, 9, 725505. [CrossRef]
- Gutiérrez-Canales LG, Muñoz-Corona C, Barrera-Chávez I, Viloria-Álvarez C, Macías AE, Guaní-Guerra E. Quality of Life and Persistence of Symptoms in Outpatients after Recovery from COVID-19. Medicina (Kaunas). 2022, 58, 1795. [CrossRef]
- Germann N, Amozova D, Göhl-Freyn K, Fischer T, Frischknecht M, Kleger G-R, Pietsch U, Filipovic M, Brutsche MH, Frauenfelder T, et al. Evaluation of psychosomatic, respiratory, and neurocognitive health in COVID-19 survivors 12 months after ICU discharge. COVID. 2024, 4, 1172-1185. [CrossRef]
- Muñoz-Corona C, Gutiérrez-Canales LG, Ortiz-Ledesma C, Martínez-Navarro LJ, Macías AE, Scavo-Montes DA, et al. Quality of life and persistence of COVID-19 symptoms 90 days after hospital discharge. J Int Med Res. 2022, 50, 3000605221110492. [CrossRef]
- Koullias E, Fragkiadakis G, Papavdi M, Manousopoulou G, Karamani T, Avgoustou H, et al. Long-Term Effect on Health-Related Quality of Life in Patients With COVID-19 Requiring Hospitalization Compared to Non-hospitalized COVID-19 Patients and Healthy Controls. Cureus. 2022, 14, e31342. [CrossRef]
- da Silveira AD, Scolari FL, Saadi MP, Brahmbhatt DH, Milani M, Milani JGPO, et al. Long-term reduced functional capacity and quality of life in hospitalized COVID-19 patients. Frontiers in Medicine. 2024, 10, 1289454. [CrossRef]
- Bolgeo T, Di Matteo R, Gatti D, Cassinari A, Damico V, Ruta F, et al. Impact of COVID-19 on Quality of Life After Hospital Discharge in Patients Treated With Noninvasive Ventilation/Continuous Positive Airway Pressure: An Observational, Prospective Multicenter Study. Dimensions of Critical Care Nursing. 2024, 43, 3–12.
- Wiertz CMH, Hemmen B, Sep SJS, van Santen S, van Horn YY, van Kuijk SMJ, et al. Life after COVID-19: the road from intensive care back to living - a prospective cohort study. BMJ Open. 2022, 12, e062332. [CrossRef]
- Rizanaj N, Gavazaj F. Effects of depressive and anxiety-related behaviors in patients aged 30–75+ who have experienced COVID-19. COVID. 2024, 4, 1041-1060. [CrossRef]
- Mazurek J, Cieślik B, Szary P, Rutkowski S, Szczegielniak J, Szczepańska-Gieracha J, et al. Association of Acute Headache of COVID-19 and Anxiety/Depression Symptoms in Adults Undergoing Post-COVID-19 Rehabilitation. J Clin Med. 2022, 11, 5002. [CrossRef]
- Liu Z, Qiao D, Xu Y, Zhao W, Yang Y, Wen D, et al. The Efficacy of Computerized Cognitive Behavioral Therapy for Depressive and Anxiety Symptoms in Patients With COVID-19: Randomized Controlled Trial. J Med Internet Res. 2021, 23, e26883. [CrossRef]
- Asimakos A, Spetsioti S, Mavronasou A, Gounopoulos P, Siousioura D, Dima E, et al. Additive benefit of rehabilitation on physical status, symptoms and mental health after hospitalisation for severe COVID-19 pneumonia. BMJ Open Respir Res. 2023, 10, e001377. [CrossRef]
- Jin Y, Xu J, Liu D. The relationship between post traumatic stress disorder and post traumatic growth: gender differences in PTG and PTSD subgroups. Soc Psychiatry Psychiatr Epidemiol. 2014, 49, 1903-10. [CrossRef]
- Mahmoudi H, Saffari M, Movahedi M, Sanaeinasab H, Rashidi-Jahan H, Pourgholami M, et al. A mediating role for mental health in associations between COVID-19-related self-stigma, PTSD, quality of life, and insomnia among patients recovered from COVID-19. Brain Behav. 2021, 11, e02138. [CrossRef]
- Khan S, Siddique R, Li H, Ali A, Shereen MA, Bashir N, et al. Impact of coronavirus outbreak on psychological health. J Glob Health. 2020, 10, 010331. [CrossRef]
- Zysberg L, Zisberg A. Days of worry: Emotional intelligence and social support mediate worry in the COVID-19 pandemic. J Health Psychol. 2022, 27, 268-277. [CrossRef]
- Li J, Li X, Jiang J, Xu X, Wu J, Xu Y, et al. The Effect of Cognitive Behavioral Therapy on Depression, Anxiety, and Stress in Patients With COVID-19: A Randomized Controlled Trial. Front Psychiatry. 2020, 11, 580827. [CrossRef]
- Cheng P, Kalmbach DA, Tallent G, Joseph CL, Espie CA, Drake CL. Depression prevention via digital cognitive behavioral therapy for insomnia: a randomized controlled trial. Sleep. 2019, 42, zsz150. [CrossRef]
- Kong X, Kong F, Zheng K, Tang M, Chen Y, Zhou J, et al. Effect of Psychological-Behavioral Intervention on the Depression and Anxiety of COVID-19 Patients. Front Psychiatry. 2020, 11, 586355. [CrossRef]
- Vink M, Vink-Niese A. Could Cognitive Behavioural Therapy Be an Effective Treatment for Long COVID and Post COVID-19 Fatigue Syndrome? Lessons from the Qure Study for Q-Fever Fatigue Syndrome. Healthcare (Basel). 2020, 8, 552. [CrossRef]
- Rutkowski S, Bogacz K, Czech O, Rutkowska A, Szczegielniak J. Effectiveness of an Inpatient Virtual Reality-Based Pulmonary Rehabilitation Program among COVID-19 Patients on Symptoms of Anxiety, Depression and Quality of Life: Preliminary Results from a Randomized Controlled Trial. Int J Environ Res Public Health. 2022, 19, 16980. [CrossRef]

Table 1.
Clinical and sociodemographic characterization of the two groups of patients.
| Variables | Total (n=15) | WG (n=7) | ICUG (n=8) | p |
|---|---|---|---|---|
| Idade, média (dp) | 53,4 (14,1) | 51,7 (17,4) | 54,9 (11,4) | 0,68¹ |
| Sex, n (%) | 0,28² | |||
| Female | 10 (66,7) | 6(85,7) | 5(50) | |
| Male | 5(33,3) | 1(14,3) | 4(50) | |
| Self-reported race, n (%) | 0,5² | |||
| White | 2(13,4) | 0 | 2(25,0) | |
| Brown | 8(53,3) | 5(71,4) | 3(37,5) | |
| Black | 5(33,3) | 2(28,6) | 3(37,5) | |
| Educational status, n (%) | 1² | |||
| Incomplete elementar school | 2(13,3) | 1(14,3) | 1(12,5) | |
| Complete primary school | 3(20,0) | 1(14,3) | 2(25,0) | |
| High school | 7(46,7) | 3(42,9) | 4(50,0) | |
| University education | 3(20,0) | 2(28,6) | 1(12,5) | |
| Comorbidities, n (%) | ||||
| DM | 4 (26,7) | 1(14,3) | 3(37,5) | 0,56² |
| SAH | 6(40,0) | 2(28,6) | 4(50,0) | 0,6² |
| Respiratory diseases | 0 | 0 | 0 | - |
| Hepatic steatosis | 2(13,3) | 0 | 2(25,0) | 0,46² |
| Obesity | 3(20,0) | 0 | 3(37,5) | 0,2² |
| Dyslipidemia | 1(6,7) | 0 | 1(12,5) | 1² |
| Anxiety, n (%) | 8(53,3) | 2(28,6) | 6(75,0) | 0,13¹ |
| Depression, n (%) | 3(20,0) | 2(28,6) | 1(12,5) | 0,56¹ |
| Hospitalization time, n (%) | 11,3 (10,1) | 6,4 (6,5) | 15,5 (11,2) | 0,08¹ |
Note: DM: diabetes Mellitus; WG: ward group; ICUG: intensive care unit group; SAH: systemic arterial hypertension; Values in mean and standard deviation (sd) or absolute (n) and relative (%) frequencies. 1 t-Student test ² Fisher's exact test.
Table 2.
Anxiety, depression and post-traumatic stress disorder.
| Pre-intervention | Post-intervention | p WG pre x post² |
p ICUG pre x post² |
|||||
|---|---|---|---|---|---|---|---|---|
| WG (n=7) | ICUG (n=8) | p | WG (n=7) | ICUG (n=8) | p | |||
| IES | 0,2 | 1 | 1 | 1 | ||||
| <10 | 0 | 2(28,6) | 7(87,5) | 6(85,7) | ||||
| ≥ 10 | 8(100,0) | 5(71,4) | 1(12,5) | 1(14,3) | ||||
| TEPT | 1 | --- | 0,38 | 0,34 | ||||
| <1.09 | 4(50,0) | 4(57,1) | 8(100,0) | 7(100,0) | ||||
| ≥1.09 | 4(50,0) | 3(42,9) | 0 | 0 | ||||
| Depression (HADS-D) | 0,53 | 0,56 | --- | --- | ||||
| Unlikely diagnosis | 2(25,0) | 1(14,3) | 5(62,5) | 6(85,7) | ||||
| Possible diagnosis | 2(25,0) | 4(57,1) | 3(37,5) | 1(14,3) | ||||
| Probable diagnosis | 4(50,0) | 2(28,6) | ||||||
| Anxiety (HADS-A) | 1 | 0,56 | --- | --- | ||||
| Unlikely diagnosis | 1(12,5) | 1(14,3) | 7(87,5) | 5(71,4) | ||||
| Possible diagnosis | 4(50,0) | 4(57,1) | 1(12,5) | 2(28,6) | ||||
| Probable diagnosis | 3(37,5) | 2(28,6) | ||||||
Note: WG: ward group; ICUG: intensive care unit group; HADS: hospital anxiety and depression scale; HEI: scale of event impact; PTSD: post-traumatic stress disorder.
Table 3.
Anxiety, depression and post-traumatic stress disorder before and after psychotherapy.
| Pre-intervention | Post-intervention | p ICUG | p WG | |||||
|---|---|---|---|---|---|---|---|---|
| WG | ICUG | p¹ | WG | ICUG | p¹ | pré x pós | pré x pós | |
| TEPT average (sd) | 0,8(0,3) | 1,0(0,2) | 0,1¹ | 0,4(0,2) | 0,8(0,3) | 0,86¹ | 0,001² | 0,004² |
| Depression (HADS) (IQ) | 10(8-12) | 10(7,5-13,5) | 0,86³ | 4(3-7) | 5(2,5-8) | 0,72³ | 0,014 | 0,014 |
| Anxiety (HADS) (IQ) | 10(9-12) | 10(9,5-12,5) | 0,51³ | 6(2-8) | 5,5(2-6,5) | 0,48³ | 0,014 | 0,014 |
Note: WG: ward group; ICUG: intensive care unit group; HADS: hospital anxiety and depression scale; IQ: interquartile; PTSD: post-traumatic stress disorder. Values presented as mean, median and interquartile ranges. 1,2 Student t-test; 3 Mann-Whitney test; 4 Wilcoxon test. SD: standard deviation.
Table 4.
Quality of life befor’'e and after psychotherapy.
| Pre-intervention | Post-intervention | p ICUG pre x pós² |
p WG pre x pós² |
Δ ICUG |
Δ WG |
p Δ¹ |
|||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SF-36 | ICUG | WG | p¹ | ICUG | WG | p¹ | |||||
| Functional capacity | 28,7(19,3) | 50,7(30,6) | 0,11 | 56,2(25,6) | 62,1(24,5) | 0,65 | 0,01 | 0,17 | 27,5(25,2) | 11,4(19,5) | 0,19 |
| Physical aspects | 0 | 42,8(42,6) | 0,0062 | 28,1(33,9) | 46,4(36,6) | 0,33 | 0,04 | 0,79 | 28,1(33,9) | 3,6(62,0) | 0,35 |
| Pain | 55,5(30,0) | 58,6(27,2) | 0,84 | 71,2(27,7) | 64,6(24,9) | 0,63 | 0,13 | 0,41 | 15,7(26,0) | 6,0(18,0) | 0,42 |
| General health status | 48,6(15,1) | 50,3(19,2) | 0,85 | 55,5(11,6) | 64,6(16,9) | 0,24 | 0,18 | 0,01 | 6,9(13,2) | 14,3(11,1) | 0,26 |
| Vitality | 49,4(18,0) | 50,7(7,3) | 0,55* | 63,1(18,7) | 62,1(20,8) | 0,92 | 0,01 | 0,12 | 13,7(16,8) | 11,4(16,5) | 0,79 |
| Social aspects | 48,4(25,4) | 55,3(25,9) | 0,61 | 65,6(23,8) | 67,8(27,8) | 0,87 | 0,12 | 0,15 | 17,2(28,3) | 12,5(20,4) | 0,72 |
| Emotional aspects | 25(23,8) | 61,9(35,6) | 0,01 | 58,3(38,8) | 57,1(16,2) | 0,94 | 0,01 | 0,8 | 33,3(30,9) | -4,8(48,9) | 0,08 |
| Mental Health | 52,7(22,3) | 52,6(14,7) | 0,98 | 66,5(21,8) | 66,8(17,5) | 0,97 | 0,02 | 0,01 | 13,7(13,7) | 14,3(10,5) | 0,93 |
Note: WG: ward group; ICUG: intensive care unit group. Values presented as mean (standard deviation). ¹Student t-test; 2 Mann-Whitney test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



