
Submitted:
17 August 2025
Posted:
18 August 2025
You are already at the latest version
Abstract
Introduction: The prognosis for patients admitted to emergency departments (ED) after drowning or diving accidents is often uncertain. In this study, we evaluated a range of clinical and laboratory parameters as potential predictors of survival. Many of these markers have previously been investigated in the context of survival prediction in both trauma-related and non-trauma-related clinical scenarios. Methods: We conducted a retrospective analysis of 25 patients aged >17 years who were admitted to the ED of the University Hospital Leipzig after drowning or diving accidents between 2012 and 2024. Clinical and laboratory parameters were compared between survivors and nonsurvivors, with survival defined as discharge from the hospital. Results: Of all cases analyzed—comprising 19 drowning and six diving incidents—10 patients (40%) survived, while 15 (60%) did not. Age, sex, or etiology of the accident were not statistically associated with survival. Compared to survivors, nonsurvivors were significantly more likely to have received prehospital cardiopulmonary resuscitation (CPR; 20% vs. 86.7%) and to have exhibited lower Glasgow Coma Scale scores and lower pH values (7.4 vs. 6.7). They were also more likely to have shown increased levels of lactate (4.3 mmol/l vs. 14.8 mmol/l), CK-MB quotient (9.7% vs. 51.8%), myoglobin (188.9 µg/l vs. 1930.9 µg/l), and blood sugar (6.6 mmol/l vs. 14.3 mmol/l). Conclusions: The need for CPR appears to be the most significant risk factor for not surviving a drowning or diving accident. Furthermore, selected laboratory parameters, such as pH and lactate, may serve as tools for predicting survival in these patients. Early decision-making regarding the continuation of CPR remains a critical and routine challenge for ED teams. Our findings offer a rationale for future prospective studies, aiming to incorporate additional clinical and biochemical markers and potentially develop new prognostic scoring systems for patients following drowning or diving accidents.
Keywords:
drowning
; diving accidents
; mortality
; survival
; emergency department
; survival prediction
; prognostic markers
1. Introduction
In 2024, the German Lifesaving Society reported 411 drowning-related deaths in Germany [1]. Worldwide, more than 500,000 deaths are caused by unintentional drowning each year [2]. Currently, there is no similar central registry for diving accidents in Germany [3]. However, the German Association of Sports Divers reported 62 diving accidents in Germany in the year 2018 [4]. Other European studies have also reported relatively low numbers of diving accidents; for example, a study from Spain recorded only 25 cases over a 10-year period [5]. According to the German Resuscitation Registry (GRR), 0.4% (approximately 42 cases) of all out-of-hospital reanimations in 2023 were related to drowning accidents [6]. Unfortunately, most patients with clinically diagnosed decompression sickness (DCS) are not monitored further, rendering data on the long-term outcomes of diving accidents sparse and unreliable [3,7,8]. The lack of a consistent database representing both fatal and nonfatal drowning incidents has been a central point of criticism [9].
The prognosis for these patients at hospital admission is often unclear and depends on several factors. Diving accidents often result in DCS, which is caused by the formation of free inert gas bubbles (e.g., nitrogen) during rapid ascent to the surface. The S2k guidelines categorize DCS according to symptoms: mild cases present with symptoms such as skin irritation and fatigue, while severe cases present with pain and neurological or/and cardiocirculatory symptoms [7,10]. Additionally, barotrauma of the lungs and arterial gas embolism can develop, both of which can be fatal [7,11]. While several predisposing factors may lead to diving accidents and a generally different pathology, the most common forensic cause of death assigned to fatal diving accidents is drowning – as shown in numerous other studies [11,12,13,14] – which is why we decided to statistically group and evaluate the two entities as one.
According to the current S2k guideline from March 2023 [10], the most important therapeutic measure in diving accidents is the immediate administration of 100% oxygen, or hyperbaric oxygen therapy (HBOT) in severe cases. The objective of emergency treatment for drowning- and diving-related accidents is the rapid management of hypoxia to prevent permanent neurological damage and loss of function [15]. Airway management, fluid resuscitation, and cardiopulmonary resuscitation (CPR) according to the most recent guidelines may be necessary [7,10].
Upon admission to the emergency department (ED) at a hospital, the prognosis for patients who have had drowning or diving accidents depends on the accident itself or the submersion time in the case of drowning. Laboratory markers such as pH and lactate values, blood sugar, and heart enzymes (troponin, myoglobin, and CK-MB quotient) may be important in predicting survival and for clinical outcome. For example, blood sugar changes in trauma patients have been used to predict ED mortality [16], which might also be applicable for evaluating outcomes in cases of drowning and diving accidents. Similarly, the dynamics of lactate acidosis have been investigated as a potential predictor of 30-day mortality in nontrauma patients following CPR [17]. Lactate acidosis itself is associated with poor clinical outcomes, whether measured as a single value or as sustained hyperlactatemia [18]. Heart enzymes such as troponin, CK-MB, and myoglobin are standard laboratory markers used to diagnose acute myocardial infarction and ischemia, despite their clinical relevance being continuously questioned and critically reviewed [19,20]. Many factors surrounding drowning and diving, such as hypothermia, the diving reflex, and respiratory failure, can lead to bradycardia, myocardial ischemia, and death by cardiac arrest [21].
In our study, we evaluated clinical and laboratory parameters that could be significant in quantifying survival outcomes after drowning or diving accidents. Previous studies have examined similar parameters, particularly lactate values, as prognostic markers for survival in both trauma and nontrauma patients [17,18,22]. The primary objective of this study was to evaluate whether these parameters were also associated with survival status after the incident in patients presenting with drowning- or diving-related accidents in EDs.
2. Methods
2.1. Study Design
In a retrospective study, we evaluated patients aged over 17 years who had been involved in drowning or diving accidents and were admitted to the ED of the University Hospital of Leipzig between 01.01.2012 and 31.12.2024.
2.2. Data Source and Variables
Patient data were retrieved from the electronic patient management system IS-H (Industry Solutions Healthcare by SAP, version 618) using the relevant ICD-10 codes (International Statistical Classification of Diseases and Related Health Problems, 10th Revision) for drowning: T75.1; decompression sickness: T70.3; and diving accident: W16.
We obtained information on patients’ age, sex, the type of accident they were involved in, and their clinical and laboratory parameters (see Table 1 for an overview of these parameters). Patients were classified as survivors or nonsurvivors based on their hospital discharge status, with survival defined as discharge from the hospital and nonsurvival as in-hospital death.
We also evaluated cause of death in the nonsurvivor group.
2.3. Statistical Analyses
All statistical analyses were carried out using IBM SPSS Statistics 29 (Armonk, NY, USA) with a two-sided α level of .05. For descriptive statistics, missing values in single variables were considered by presenting absolute values, range, and frequencies as % (n/invalid). Continuous variables were presented as mean (M) ± standard deviation (SD).
Differences between categorical variables were analyzed using Fisher’s exact tests. We specifically analyzed differences between survivors and nonsurvivors in the following categorial variables: “case” (drowning, diving), “sex” (male, female), “CPR received” (yes, no), and “GCS” (GCS ≤ 8, GCS 9-12, GCS ≥ 13).
Group differences in normally distributed continuous variables were analyzed using univariate analyses of variance (ANOVAs). We specifically analyzed differences between survivors and nonsurvivors in the following normally distributed continuous variables: “age”, “body temperature”, “CK-MB quotient”, “pH”, “lactate”, and “blood sugar”.
Group differences in non-normally distributed continuous variables were analyzed using Mann-Whitney U-tests. We specifically analyzed differences between survivors and nonsurvivors in the following non-normally distributed continuous variables: “GCS”, “troponin”, and “myoglobin”.
3. Results
3.1. Patient Characteristics
During the study period, 25 patients were admitted to the ED and included in the analysis [sex: 17 (68%) male, 8 (32%) female, mean age: 49.3 ± 20.5 years]. Of these patients, 19 (76%) had experienced a drowning accident, while 6 (24%) had been involved in a diving accident. The location of the drowning or diving accident was a lake in 19 cases (76%), other freshwater sources in 4 cases (16%), a pool in one case (4%), and a bathtub in one case (4%).
In total, 15 patients (60%) did not survive the accident. Following drowning incidents, six patients (31.6%) survived, while 13 did not (68.4%). Following diving accidents, four patients (66.7%) survived and two did not (33.3%). Age, sex, or etiology of the accident were not statistically associated with survival. The detailed characteristics of survivors and nonsurvivors can be found in Table 2.
3.2. Clinical Findings in Survivors and Nonsurvivors
In the group of nonsurvivors, CPR was more commonly administered (86.7%) than in the group of survivors (20%). A total of 15 patients (60%) received CPR, of whom two (13.3%) survived and 13 (86.7%) did not. There was a significant association between receiving CPR and survival rate (p = 0.002; Figure 1). Of the four patients in whom CPR was performed for a maximum time of 10 min, two survived. In contrast, none of the 11 patients who received CPR for more than 10 min survived. When the no-flow time exceeded 5 min (in eight patients receiving CPR, 53.3%) none survived, whereas among the six patients (40%) with a no-flow time of less than 5 min, two (33.3%) survived.
In our sample, the GCS values ranged from 3 to 15, with 18 patients showing severe brain injury (GCS ≤ 8) and seven patients showing minor neurological impairment (GCS ≥ 13). No patients showed moderate neurological impairment (GCS 9-12). All patients in the nonsurvivor group exhibited a GCS score of 3, which differed significantly from the scores of survivors (p < 0.001).
The mean body temperature across all clinical cases was 34.6 ± 2.9°C (range 28.0-37.0°C). In nonsurvivors, body temperature was lower (33.5°C) than in survivors (36.1°C); however, this difference was not statistically significant (p = 0.100). A detailed description of the clinical parameters for survivors and nonsurvivors can be found in Table 2.
Of the 15 nonsurvivors, forensic autopsy revealed that hypoxic brain injury was the leading cause of death in seven cases (46.7%), followed by heart failure and multi-organ failure in four cases each (26.7%).
3.3. Laboratory Findings in Survivors and Nonsurvivors
The mean lactate value across all clinical cases was 10.5 ± 8.5 mmol/l (range 0.9-28.0), with values of 4.3 mmol/l in survivors and 14.8 mmol/l in nonsurvivors (p =0.002; Figure 2).
The mean pH value across all clinical cases was 7.0 ± 0.4 (range 6.3-7.5). Consistent with the lactate levels, there was a significant difference in pH between survivors (pH = 7.4) and nonsurvivors (pH = 6.7; p < 0.001).
The mean blood sugar level across all clinical cases was 11.6 ± 5.0 mmol/l (range 4.9-20.7), with blood sugar levels of 6.6 mmol/l in survivors and 14.3 mmol/l in nonsurvivors (p < 0.001).
The mean values for the heart enzymes across all clinical cases were 49.2 ± 60.2 pg/ml for troponin (range 4.6-211.0), 1,253.5 ± 1,754.0 µg/l for myoglobin (range 25.0-7,010.0), and 35.5 ± 26.4% for CK-MB quotient (range 4.6-86.9). Among survivors versus nonsurvivors, the respective values were 19.2 pg/ml versus 67.7 pg/ml (p = 0.076) for troponin, 188.9 µg/l versus 1,930.9 µg/l (p < 0.001) for myoglobin, and 9.7% versus 51.8% (p < 0.001) for the CK-MB quotient. A detailed description of the laboratory parameters for survivors and nonsurvivors can be found in Table 2.
4. Discussion
The results of this study indicate that markers associated with not surviving a drowning or diving accident include receiving out-of-hospital CPR and having a low GCS score, decreased pH levels, and increased levels of lactate, CK-MB-quotient, myoglobin, and blood sugar. There was no significant association in our sample between survival and sex, age, body temperature, troponin, or whether the incident was drowning or diving.
Our study found that there is a significant association between receiving out-of-hospital CPR and not surviving, indicating that patients who require CPR after a drowning or diving accident are more likely to have a fatal outcome than those who do not undergo CPR. This finding aligns with established clinical understanding, as even brief periods of cardiac and pulmonary dysfunction are known to adversely affect survival and neurological outcomes, regardless of the cause of OHCA [26]. The necessity and duration of CPR comprise two of the most critical factors affecting survival in preclinical settings [24]. Parameters such as no-flow time, CPR duration, and the occurrence of return of spontaneous circulation (ROSC) have been proposed as predictors of survival in OHCA. This also includes the quality of CPR and preclinical medical care provided by healthcare professionals and laypersons [6,24,26]. However, the results of other studies indicate that the duration of CPR may not significantly impact long-term survival [27], and the value of CPR duration as a direct prognostic marker for survival remains unclear [19].
Given the pathophysiology of drowning – which inevitably leads to terminal apnea followed by cardiac arrest – the strong association between receiving CPR and survival is coherent. Furthermore, it is noteworthy that, among OHCA patients in 2023, the GRR reported that only 41.4% achieved ROSC, and 24-h survival was below 20% [6].
Due to the small number of cases in our study, we could not test for a statistical association between CPR duration and survival, as only two of the 15 patients who received CPR survived. Importantly, these two patients were in the group in which CPR duration was less than 10 min, whereas all 11 patients receiving CPR for more than 10 min died. This observation aligns with findings from a 2022 study on OHCA, which reported the lowest survival rates in patients with prolonged CPR durations (>20 min) and the highest survival rates in those with shorter durations (<10 min) [27]. Moreover, we could not test for a statistical association between survival and no-flow time. However, as with CPR duration, all survivors presented a no-flow time of less than 5 min. In the nonsurvivor group, no-flow time was more than 5 min in eight patients. It can be assumed that, specifically in diving accidents, rescue from the water takes longer and therefore no-flow times are longer. Other studies have found that no-flow time can be a reliable prognostic marker for survival and neurological outcome in patients with OHCA of endogenous origin [29].
The leading clinical cause of death in the nonsurvivor group was hypoxic brain injury. Previous studies often related neurological outcomes to the duration of CPR, the timing of intervention, and the management of hypothermia [30]. For drowning and diving accidents, all of these parameters are difficult to determine, as rescue from the water may be prolonged and hypothermia is more likely [31]. This circumstance may be one reason why hypoxic brain injury was the leading cause of death, and it is an important factor to consider when treating patients who have suffered a drowning or diving accident.
Body temperature constitutes an ambivalent factor in both clinical and preclinical care. Hypothermia is considered to be part of the triad of death, alongside coagulopathy and acidosis [32]. However, hypothermia can also have neuroprotective properties and is used in clinical settings to preserve neurological function and prevent brain damage caused by hypoxia [15]. In our study, no significant relationship was found between body temperature and survival; however, body temperature was below physiological levels in those patients who did not survive. Other studies have described a correlation between low rectal temperature and a worse clinical outcome in both drowning- and non-drowning-related cases [33,34]. Specifically in drowning cases, a low rectal temperature was associated with a longer period of submersion and a lower water temperature [21,31]. However, as most studies conducted on this topic focused on pediatric patients, the results may not be applicable to adults.
The GCS is primarily used in preclinical settings to assess state of consciousness after traumatic brain injury [35]. All patients in the nonsurvivor group were found to have a GCS of ≤8, whereas the majority of patients in the survivor group exhibited a GCS of ≥13. Given that loss of consciousness due to hypoxia is a key feature of the pathophysiology of drowning, particularly in severe cases, it is reasonable to expect a significant relationship between survival and GCS score, which serves as a quantitative measure of consciousness and neurological impairment [35]. This correlation has also been demonstrated in other studies, particularly those investigating survival following OHCA or survival in trauma patients [24,36].
With respect to laboratory parameters, we found that pathological values in several markers were associated with survival outcomes in drowning and diving accidents. Many of these parameters are also established prognostic indicators in other clinical conditions, such as trauma and myocardial infarction [5]. One of the primary objectives of the present study was to evaluate whether these laboratory parameters could also serve as predictors of survival in drowning and diving accidents. Indeed, our findings are consistent with those of the OBSERvE-Lactate study, which examined lactate levels as a prognostic indicator for survival in trauma patients [17]. In our cohort, lactate concentrations were markedly elevated in fatal cases, whereas survivors exhibited values close to physiological levels, although still slightly elevated. Similar findings were reported in another study that assessed lactate as an early predictor for survival and clinical outcomes in patients undergoing resuscitative care [35]. In that same study, a correlation between survival and pH value was also identified, with pH being reported as an independent predictor of survival in several other studies [37]. Given the well-established inverse relationship between lactate and pH—where elevated lactate levels contribute to metabolic acidosis and thus lower pH values [18]—this result was anticipated, particularly in light of the observed association between lactate levels and survival in our study.
Concerning heart enzymes, both the CK-MB quotient and myoglobin levels were found to be associated with survival in the present study. However, these parameters are usually used in diagnosing myocardial infarction and can also be elevated in cases of noncardiac skeletal muscle injury (e.g., rhabdomyolysis) or renal failure [19]. Given that drowning leads to cardiac arrest and hypoxia-induced muscular stress and ischemia, an increase in the CK-MB ratio and myoglobin is not unexpected. Importantly, CPR itself may contribute to elevating the CK-MB ratio, as chest compressions exert direct mechanical pressure on the heart, potentially increasing cardiac creatine kinase release. Therefore, these observed associations may not be specific to drowning pathophysiology, and the CK-MB ratio might not serve as a reliable predictor of survival in drowning or diving accidents. This interpretation is supported by findings from another study investigating differences between in- and out-of-hospital cardiac arrests and resuscitations. In that study, an elevated CK-MB ratio was observed, with no significant differences between groups [37], suggesting that an increase in the CK-MB-quotient is probably a CPR effect. Additionally, the prognostic value of myoglobin remains uncertain, with some authors even recommending that routine measurement be discontinued due to the limited clinical utility of that parameter [20].
We also observed a significant association between blood sugar level and survival. Although research on this specific association in drowning and diving accidents is limited, some studies examining blood glucose as a prognostic marker for neurological outcomes and survival in trauma patients support our findings [16]. However, our study did not assess whether elevated blood sugar levels were present prior to the incident or were a physiological response to the drowning or diving event.
Overall, predicting survival in drowning and diving accidents is quite similar to that for other clinical conditions, including both trauma-related and nontraumatic fatalities [17,25]. While the severity and pathophysiological expression of certain parameters may differ in drowning compared to other causes of hospitalization, their implications for survival and the urgency of appropriate medical intervention are likely comparable. However, drowning and diving incidents present distinct challenges, such as prolonged rescue times, environmental factors such as water temperature, and extended submersion or no-flow times. These unique circumstances underscore the critical importance of rapidly assessing the situation and initiating appropriate interventions, including CPR, thermoregulation, HBOT, and other clinical treatments.
This study has several limitations. It is a monocentric, retrospective analysis based on a small sample size (n = 25), which limits the generalizability of the findings. As a cross-sectional study, no follow-up was conducted on surviving patients, and neurological outcomes were not assessed. Additionally, evolving clinical treatment protocols over the study period (2012–2024), along with incomplete data for some variables, further constrain the robustness of the results.
5. Conclusions
This study could serve as a foundation for optimizing the clinical management of adult patients involved in drowning and diving accidents, potentially enabling earlier and more informed decision-making based on laboratory and preclinical parameters. Based on our findings, we propose several recommendations to improve outcomes in such cases: establish a centralized national registry for diving accidents, develop extended emergency and rescue protocols specific to immersion-related incidents, and implement structured post-hospital follow-up documentation for survivors of drowning and diving accidents.
Author Contributions
Conceptualization AP, JD, AG; methodology AP, JD, AS, AG; formal analysis AP, AS; data curation AP, AS; writing of the original draft preparation AP, AG; writing—review and editing JD, AS; visualization, AS; supervision, AG; All authors have read and agreed to the published version of the manuscript.
Funding
No funding was received for conducting this study.
Institutional Review Board Statement
The study was carried out in accordance with the Declaration of Helsinki and the study protocol was approved by the research ethics committee of the Leipzig University (reference number 224/24-ek). The study complies with the current laws in Germany and with institutional regulations. As the present study included the retrospective analysis of clinical data and medical records, the need for informed consent was waived.
Data Availability Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Acknowledgments
We thank Dr. med. Julia Schlote and Katharina Fasold-Beuth for their support. For proofreading we thank Sherryl Sundell.
Conflicts of Interest
The authors have no competing interests to declare.
References
- DLRG:Statistik Ertrinken. 2024. Available online: https://www.dlrg.de (accessed on 13 March 2025).
- Szpilman, D.; Bierens, J.J.; Handley, A.J.; Orlowski, J.P. Drowning. New Engl. J. Med. 2012, 366, 2102–2110. [Google Scholar] [CrossRef] [PubMed]
- Eichhorn, L.; Leyk, D. Diving Medicine in Clinical Practice. Dtsch. Aerzteblatt Online 2015, 112, 147–158. [Google Scholar] [CrossRef] [PubMed]
- VDST: Unfallanalyse. 2018. Available online: https://www.vdst.de (accessed on 12 March 2025).
- Ceglarek, U.; Schellong, P.; Rosolowski, M.; Scholz, M.; Willenberg, A.; Kratzsch, J.; Zeymer, U.; Fuernau, G.; de Waha-Thiele, S.; Büttner, P.; et al. The novel cystatin C, lactate, interleukin-6, and N-terminal pro-B-type natriuretic peptide (CLIP)-based mortality risk score in cardiogenic shock after acute myocardial infarction. Eur. Hear. J. 2021, 42, 2344–2352. [Google Scholar] [CrossRef]
- Fischer, M; et al. Öffentlicher Jahresbericht 2023 des Deutschen Reanimationsregisters: Außerklinische Reanimation 2023. 10 May 2024. Available online: www.reanimationsregister.de/berichte.html (accessed on 10 May 2025).
- Böttcher, F; et al. Tödlicher Tauchunfall. In Der Anaesthesist; Springer: Berlin, 2012. [Google Scholar]
- Guillén-Pino, F.; Morera-Fumero, A.; Henry-Benítez, M.; Alonso-Lasheras, E.; Abreu-González, P.; Medina-Arana, V. Descriptive study of diving injuries in the Canary Islands from 2008 to 2017. Diving Hyperb. Med. J. 2019, 49, 204–208. [Google Scholar] [CrossRef]
- Hasenjäger M, Burchert H Statistische Erfassung von Ertrinkungsnotfällen in Deutschland. Präv Gesundheitsf. 2014, 9, 305–311. [CrossRef]
- Jüttner, B.; Wölfel, C.; Camponovo, C.; Schöppenthau, H.; Meyne, J.; Wohlrab, C.; Werr, H.; Klein, T.; Schmeißer, G.; Theiß, K.; et al. S2K guideline for diving accidents. Ger. Med. Sci. 2023, 21. [Google Scholar] [CrossRef]
- Tarozzi, I.; Franceschetti, L.; Simonini, G.; Raddi, S.; Machado, D.; Bugelli, V. Black box of diving accidents: Contribution of forensic underwater experts to three fatal cases. Forensic Sci. Int. 2023, 346, 111642. [Google Scholar] [CrossRef] [PubMed]
- Buzzacott, P.L. The epidemiology of injury in scuba diving. Med Sport Sci. 2012, 58, 57–79. [Google Scholar] [CrossRef]
- Casadesús, J.M.; Aguirre, F.; Carrera, A.; Boadas-Vaello, P.; Serrando, M.T.; Reina, F. Diving-related fatalities: multidisciplinary, experience-based investigation. Forensic Sci. Med. Pathol. 2019, 15, 224–232. [Google Scholar] [CrossRef]
- Petzold, A.; Schlote, J.; Gries, A.; Dreßler, J. Fatal Diving Accidents in East Germany. J Forensic Sci & Criminal Inves. 2024, 18, 555989. [Google Scholar]
- Gries, A. Notfallmanagement bei Beinahe-Ertrinken und akzidenteller Hypothermie. Der Anaesthesist 2001, 50, 887–901. [Google Scholar] [CrossRef] [PubMed]
- Torabi, M.; Abadi, F.M.S.; Baneshi, M.R. Blood sugar changes and hospital mortality in multiple trauma. Am. J. Emerg. Med. 2018, 36, 816–819. [Google Scholar] [CrossRef]
- Kramer, A.; Urban, N.; Döll, S.; Hartwig, T.; Yahiaoui-Doktor, M.; Burkhardt, R.; Petros, S.; Gries, A.; Bernhard, M. Early Lactate Dynamics in Critically Ill Non-Traumatic Patients in a Resuscitation Room of a German Emergency Department (OBSERvE-Lactate-Study). J. Emerg. Med. 2019, 56, 135–144. [Google Scholar] [CrossRef]
- Kraut, J.A.; Madias, N.E.; Ingelfinger, J.R. Lactic Acidosis. New Engl. J. Med. 2014, 371, 2309–2319. [Google Scholar] [CrossRef]
- Saenger, A.K.; Jaffe, A.S. Requiem for a heavyweight: the demise of creatine kinase-MB. Circulation 2008, 118, 2200–2206. [Google Scholar] [CrossRef]
- Servonnet, A; et al. Y a-t-il un intérêt au dosage de la myoglobine en 2017? [Myoglobin: still a useful biomarker in 2017?]. Ann Biol Clin. 2018, 76, 137–141. [Google Scholar]
- Golden, F.S.; Tipton, M.J.; Scott, R.C. Immersion, near-drowning and drowning. Br. J. Anaesth. 1997, 79, 214–225. [Google Scholar] [CrossRef]
- Vincent, J.-L.; e Silva, A.Q.; Couto, L.; Taccone, F.S. The value of blood lactate kinetics in critically ill patients: a systematic review. Crit. Care 2016, 20, 1–14. [Google Scholar] [CrossRef]
- American Board of Internal Medicine: ABIM Laboratory Test Reference Ranges. 14 April. Available online: https://www.abim.org (accessed on 14 April 2025).
- Guy, A.; Kawano, T.; Besserer, F.; Scheuermeyer, F.; Kanji, H.D.; Christenson, J.; Grunau, B. The relationship between no-flow interval and survival with favourable neurological outcome in out-of-hospital cardiac arrest: Implications for outcomes and ECPR eligibility. Resuscitation 2020, 155, 219–225. [Google Scholar] [CrossRef]
- Thevathasan, T.; Gregers, E.; Mørk, S.R.; Degbeon, S.; Linde, L.; Andreasen, J.B.; Smerup, M.; Møller, J.E.; Hassager, C.; Laugesen, H.; et al. Lactate and lactate clearance as predictors of one-year survival in extracorporeal cardiopulmonary resuscitation – An international, multicentre cohort study. Resuscitation 2024, 198, 110149. [Google Scholar] [CrossRef] [PubMed]
- Myat, A.; Song, K.-J.; Rea, T. Out-of-hospital cardiac arrest: current concepts. Lancet 2018, 391, 970–979. [Google Scholar] [CrossRef]
- Goto, Y. No association of CPR duration with long-term survival. Resuscitation 2022, 182, 109677. [Google Scholar] [CrossRef]
- Rohlin, O.; Taeri, T.; Netzereab, S.; Ullemark, E.; Djärv, T. Duration of CPR and impact on 30-day survival after ROSC for in-hospital cardiac arrest—A Swedish cohort study. Resuscitation 2018, 132, 1–5. [Google Scholar] [CrossRef]
- Murakami, N.; Kokubu, N.; Nagano, N.; Nishida, J.; Nishikawa, R.; Nakata, J.; Suzuki, Y.; Tsuchihashi, K.; Narimatsu, E.; Miura, T. Prognostic Impact of No-Flow Time on 30-Day Neurological Outcomes in Patients With Out-of-Hospital Cardiac Arrest Who Received Extracorporeal Cardiopulmonary Resuscitation. Circ. J. 2020, 84, 1097–1104. [Google Scholar] [CrossRef]
- Perkins, G.D.; Callaway, C.W.; Haywood, K.; Neumar, R.W.; Lilja, G.; Rowland, M.J.; Sawyer, K.N.; Skrifvars, M.B.; Nolan, J.P. Brain injury after cardiac arrest. Lancet 2021, 398, 1269–1278. [Google Scholar] [CrossRef]
- Suominen, P.K.; E Korpela, R.; Silfvast, T.G.; Olkkola, K.T. Does water temperature affect outcome of nearly drowned children. Resuscitation 1997, 35, 111–115. [Google Scholar] [CrossRef]
- Mikhail, J. The trauma triad of death: hypothermia, acidosis, and coagulopathy. AACN Clin Issues 1999, 10, 85–94. [Google Scholar] [CrossRef]
- Kyriacou, D.N.; Arcinue, E.L.; Peek, C.; Kraus, J.F. Effect of Immediate Resuscitation on Children with Submersion Injury. Pediatrics 1994, 94, 137–142. [Google Scholar] [CrossRef]
- Quan, L.; Wentz, K.R.; Gore, E.J.; Copass, M.K. Outcome and Predictors of Outcome in Pediatric Submersion Victims Receiving Prehospital Care in King County, Washington. Pediatrics 1990, 86, 586–593. [Google Scholar] [CrossRef]
- Teasdale, G.; Jennett, B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974, 2, 81–84. [Google Scholar] [CrossRef]
- Khan, A.J.; Liao, C.J.; Kabir, C.; Hallak, O.; Samee, M.; Potts, S.; Klein, L.W. Etiology and Determinants of In-Hospital Survival in Patients Resuscitated After Out-of-Hospital Cardiac Arrest in an Urban Medical Center. Am. J. Cardiol. 2020, 130, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Yıldırım, S.; Varışlı, B. The effects of cardiopulmonary resuscitation (CPR) performed out-of-hospital and in-hospital with manual or automatic device methods and laboratory parameters on survival of patients with cardiac arrest. Ir. J. Med Sci. (1971-) 2023, 192, 2365–2371. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Stacked bar plots of cardiopulmonary resuscitation (CPR) performed in survivors and nonsurvivors.
Figure 1.
Stacked bar plots of cardiopulmonary resuscitation (CPR) performed in survivors and nonsurvivors.
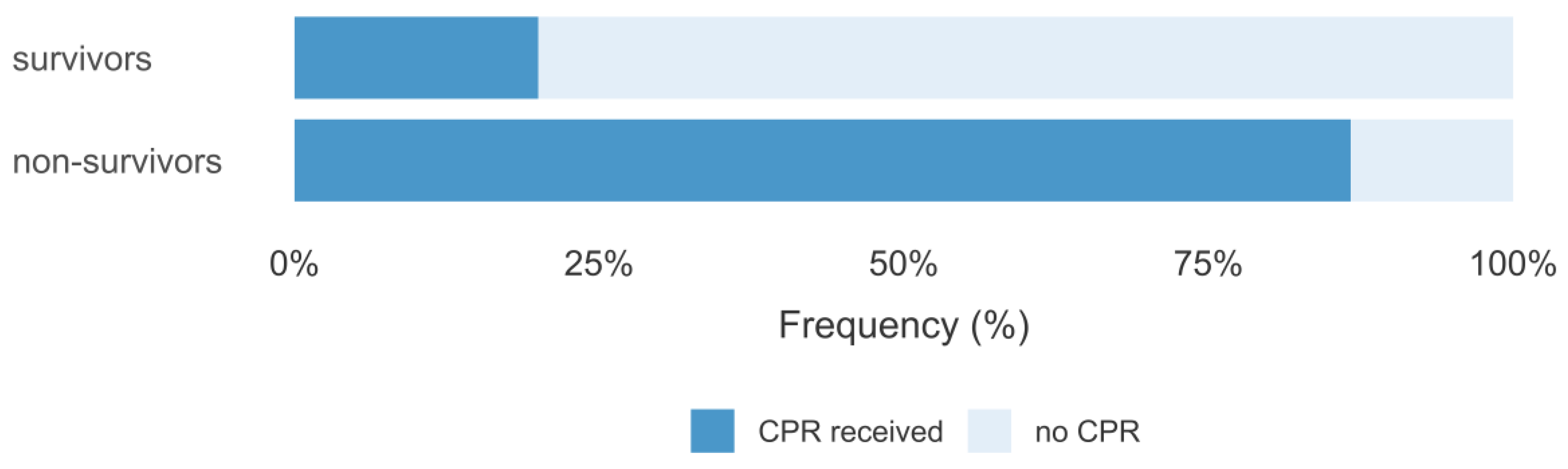
Figure 2.
Violin plots of lactate values in survivors and nonsurvivors.
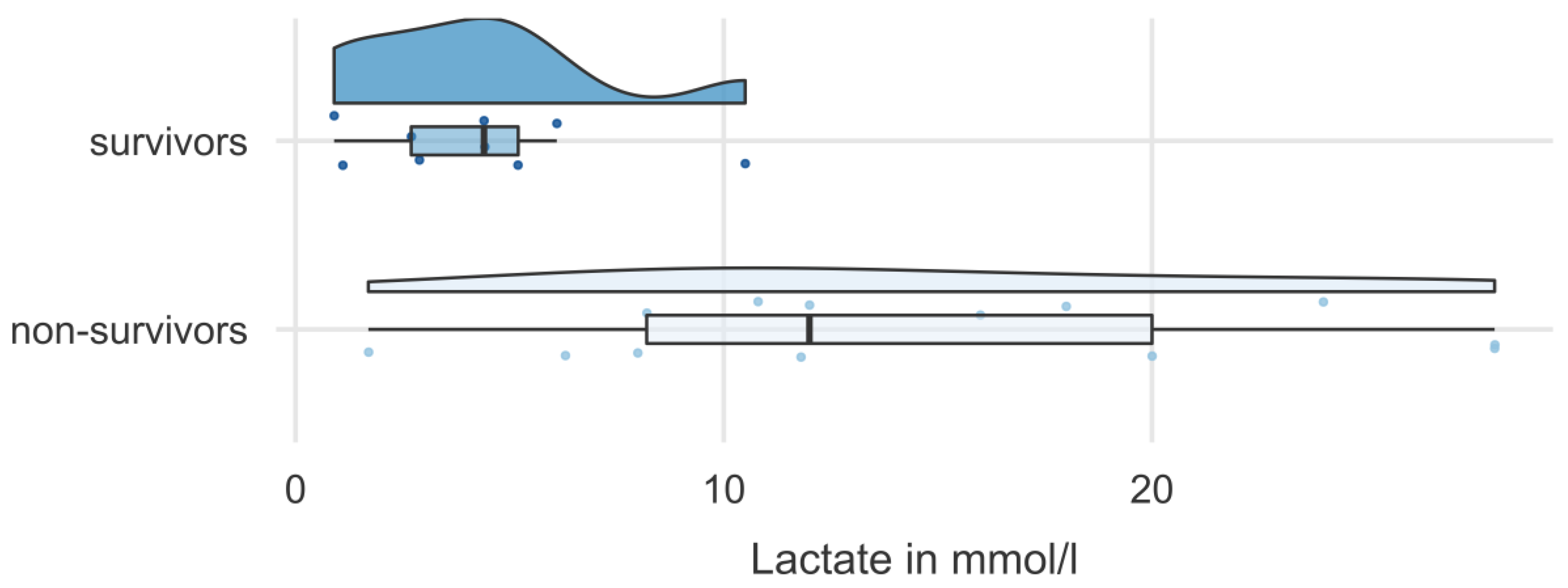

Table 1.
Clinical and laboratory parameters recorded in patients with drowning/diving accidents in the emergency department.
Table 1.
Clinical and laboratory parameters recorded in patients with drowning/diving accidents in the emergency department.
| Patient characteristics | Age [yrs] | Sex [m/f] | Survival [yes/no] | Drowning / Diving accident |
|---|---|---|---|---|
| Clinical parameters on admission | Initial body temperature [°C] (36 - 37)1 |
CPR2 duration [≤ 10 min / >10 min] | No-flow time3 [≤ 5 min / >5 min] | Glasgow Coma Scale (GCS)4 (3-15) |
| Laboratory parameters on admission | Lactate [mmol/l] (0.5 - 2.2) |
pH value (7.36 - 7.44) |
Blood sugar [mmol/l] (4.0 - 7.8) |
Heart enzymes [troponin in pg/ml (<14), CK-MB quotient in % (<6), myoglobin in µg/l (28 – 72)] |
Note. 1values in parentheses () represent the physiological range [23]. 2CPR = cardiopulmonary resuscitation. 3No-flow time is defined as time interval between onset of out-of-hospital cardiac arrest and start of cardiopulmonary resuscitation [24]. 4While the GCS was originally developed for assessing consciousness levels in traumatic brain injury [25], application of GCS in this study reflects its utility in evaluating neurological function irrespective of underlying etiology.
Table 2.
Clinical and laboratory parameters in groups of survivors and nonsurvivors after drowning or diving accidents.
Table 2.
Clinical and laboratory parameters in groups of survivors and nonsurvivors after drowning or diving accidents.
| Parameter | Survivor | Nonsurvivor | p |
|---|---|---|---|
| N | 10 | 15 | |
| Patient characteristics | |||
| Case [drowning/diving] | 6/4 | 13/2 | 0.175 |
| Sex [m/f] | 7/3 | 10/5 | 1.000 |
| Age [yrs] | 51.6±22.2 | 47.8±20.0 | 0.660 |
| Clinical findings | |||
|
CPR [yes/no] If yes: CPR duration [≤10 min, >10 min] No-flow time [≤5 min, >5 min] |
2/8 2/0 2/0 |
13/2 2/11 4/8 |
0.002 n.a. n.a. |
| Body temperature [°C] | 36.1±1.0 | 33.5±3.4 | 0.100 |
|
GCS GCS ≤ 8 GCS 9-12 GCS ≥ 13 |
3 0 7 |
15 0 0 |
<0.001 |
| Laboratory findings | |||
| Lactate [mmol/l] | 4.3±2.9 | 14.8±8.4 | 0.002 |
| pH | 7.4±0.1 | 6.7±0.3 | <0.001 |
| CK-MB quotient [%] | 9.7±4.5 | 51.8±20.5 | <0.001 |
| Myoglobin [µg/l] | 188.9±190.4 | 1930.9±1977.4 | <0.001 |
| Troponin [pg/ml] | 19.2±12.9 | 67.7±70.6 | 0.076 |
| Blood sugar [mmol/l] | 6.6±1.4 | 14.3±4.1 | <0.001 |
Note. Values represent n, mean, and standard deviation. Bold values indicate a significant difference of p < .05. n.a. = p value not applicable due to low sample size in the survivor group. CP = cardiopulmonary resuscitation; GCS = Glasgow Coma Scale.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



