
Submitted:
10 June 2025
Posted:
10 June 2025
You are already at the latest version
Abstract
Children with Congenital Zika Virus Syndrome (CZVS) experience severe neurological and nutritional impairments. Although immediate clinical consequences are well-documented, long-term anthropometric and nutritional outcomes remain poorly understood. This study assessed longitudinal anthropometric and nutritional outcomes in children affected by CZVS. A cohort of 38 children aged ≥5 years diagnosed with CZVS was followed at a reference center in Northeast Brazil. Anthropometric measures (weight, height, BMI, head circumference) were collected using standardized methods, including digital scales and anthropometric tape measures. Growth was analyzed using WHO Anthro and WHO Anthro Plus software. Dietary intake was evaluated through two 24-hour recalls and analyzed with NutWIN 2.5 software. Nutritional status was classified using WHO growth standards, and associations between dietary intake and BMI were statistically examined. Children showed significant linear growth improvement (p=0.007) without corresponding weight gain, leading to worsening BMI classifications (p=0.017). Dietary evaluations revealed limited dietary diversity, frequent intake of ultra-processed foods, inadequate fruit consumption, and widespread insufficiencies in caloric and micronutrient intake (zinc, calcium, iron, vitamin D). Low carbohydrate intake was significantly associated with inadequate BMI (p=0.030). Multidisciplinary nutritional interventions addressing medical, dietary, educational, and socioeconomic factors are essential for improving health outcomes in children with CZVS.
Keywords:
Zika virus Infection
; congenital Zika syndrome
; growth and development
; nutritional status
1. Introduction
Congenital Zika Virus Syndrome (CZVS) is a complex neurological disorder resulting from prenatal exposure to Zika Virus (ZIKV). While microcephaly is the hallmark manifestation, CZVS includes a broad spectrum of clinical features such as subcortical calcifications, ocular abnormalities, early-onset hypertonia, and arthrogryposis. These manifestations collectively impair neuropsychomotor development, communication skills, cognitive functions, and motor abilities [1,2,3,4,5].
Beyond neurological impairments, CZVS affects gastrointestinal function, causing recurrent vomiting, gastric dysmotility, and food intolerance. These symptoms, attributed to dysfunctions in the enteric and autonomic nervous systems, significantly compromise nutritional intake and overall health [6]. Additionally, motor limitations inherent to CZVS worsen feeding difficulties, adversely impacting mealtime posture during and swallowing mechanics. These challenges impose additional burdens on caregivers and frequently result in dietary practices that rely excessively on soft or pureed foods, often high in sugars and ultra-processed components [7,8,9,10,11].
Although immediate clinical and nutritional impacts of CZVS are well-documented, its long-term consequences on anthropometric development and nutritional status remain understudied. The scarcity of longitudinal research limits our understanding of these enduring challenges, restricting the development of targeted interventions. This study aimed to investigate the long-term anthropometric and nutritional outcomes in children affected by CZVS, providing evidence to inform nutritional guidelines and improve clinical care practices.
2. Materials and Methods
2.1. Study Design and Setting
This longitudinal cohort study included children diagnosed with CZVS, followed at the University Hospital of Sergipe (HU-UFS), located in Aracaju, Sergipe State, Northeast Brazil. The hospital serves as a regional reference center for medium and high-complexity care within Brazil’s Unified Health System (Sistema Único de Saúde [SUS], in portuguese) and has provided specialized clinical monitoring for CZVS since 2015. Ethical approval was granted by the Research Ethics Committee of the Federal University of Sergipe (approval no. 5.287.146), and written informed consent was obtained from all participants.
2.2. Eligibility Criteria
Participants included children aged ≥5 years with a confirmed CZVS diagnosis undergoing routine follow-up at HU-UFS outpatient clinics. Inclusion criteria required documented neonatal anthropometric measurements (height, weight, and head circumference) recorded in the official Child Health Booklet (CHB). CZVS diagnosis was confirmed at birth according to Brazilian Ministry of Health criteria: head circumference below two standard deviations from the mean for gestational age and sex, with laboratory-confirmed maternal or neonatal ZIKV exposure [12]. Exclusion criteria included maternal absence during data collection or primary caregivers other than the mother.
2.3. Study Size
Of 51 children monitored at HU-UFS, 38 fulfilled inclusion criteria with complete neonatal anthropometric documentation.
2.4. Outcomes and Measures
Structured interviews with mothers collected sociodemographic information (age, residence, marital status, socioeconomic status, employment, government benefits), obstetric history (pregnancy planning, prenatal care, delivery type), neonatal data (sex, Apgar scores, birth anthropometry, hospitalizations, complications related to CZVS), and current school attendance.
2.4.1. Anthropometric Assessment
Neonatal anthropometric data were obtained from CHB and clinically verified by a specialized maternal-child nurse following Brazilian Ministry of Health protocols. Body weight was measured using a calibrated digital scale (G-Tech®, 150 kg capacity). Children unable to stand independently due to motor impairments were weighed in the caregiver’s arms, with their weight calculated by subtracting caregiver’s weight. Height was estimated from arm length (acromion to radius head), measured using a standardized anthropometric tape, applying Stevenson’s formula: height = (4.35 × arm length) + 21.8 [13]. Head circumference was similarly measured around the occipital bone and supraorbital arch. Severe microcephaly classification followed WHO guidelines, defined as head circumference at birth below three standard deviations for gestational age and sex [14]. Growth was analyzed using WHO Anthro (0–60 months) and WHO Anthro Plus (5–19 years) software, classifying nutritional status according to Brazilian guidelines [15] (Table 1).
2.4.2. Dietary Assessment
Dietary intake was evaluated using two 24-hour dietary recalls, which documented food consumption from the previous day as reported by caregivers [16]. Dietary analyses were conducted using NutWIN 2.5 software (Federal University of São Paulo), based on the Brazilian Food Composition Table (Tabela Brasileira de Composição de Alimentos, in portuguese). Total energy intake, macronutrients (proteins, carbohydrates, lipids), and selected micronutrients (zinc, calcium, iron, vitamin D) were calculated. Energy requirements were assessed by the Culley formula [17], considering intakes within 90%–110% of recommendations adequate [8]. Macronutrient adequacy was assessed using the Acceptable Macronutrient Distribution Range (AMDR): proteins (10–30%), carbohydrates (45–65%), lipids (25–35%) [18]. Micronutrient intake was evaluated based on the Recommended Dietary Allowance (RDA): calcium (1,000 mg/day), iron (10 mg/day), zinc (5 mg/day), vitamin D (15 µg/day) [19].
2.5. Statistical Analysis
Data analyses employed R software (version 3.5.3; R Foundation for Statistical Computing). Changes in anthropometric status from birth to early childhood were analyzed using the McNemar test. Dietary intake comparisons between adequate and inadequate BMI groups utilized the Mann-Whitney test for continuous variables and Fisher’s exact test for categorical variables. A 5% significance level was adopted.
3. Results
3.1. General Characteristics of the Participants
3.1.1. Maternal Characteristics
The median age of mothers was 31 years. Most resided in urban areas (60.5%), were in stable relationships (78.9%), and unemployed (78.9%). Government financial assistance was common (92.1%), and nearly all families (94.7%) had a monthly income ranging between 1 to 3 minimum wages. Prenatal care attendance was universal, with 55.3% of mothers undergoing vaginal delivery (Table 2).
3.1.2. Child Characteristics
At birth, children had a median head circumference of 29 cm. Severe microcephaly was prevalent in 81.6% of cases. Slightly over half the children were male (52.6%), and the median age at assessment was 6 years, with a median head circumference of 44.5 cm. Frequent complications included seizures (76.3%), arthrogryposis (42.1%), and hypertonia (42.1%). Most children (80%) did not attend school (Table 3).
3.2. Anthropometric Outcomes
Longitudinal analysis demonstrated significant linear growth improvement from birth through early childhood, with an increased proportion of children reaching appropriate stature for age (p=0.007). Conversely, weight gain was stable, with no significant change (p=0.238). Particularly, BMI deteriorated significantly over time (p=0.017), with 77.3% of children classified as underweight and 22.7% as overweight or obese by the end of early childhood (Table 4). Growth trajectories relative to WHO standards are visually represented in Figure 1a–c.
3.3. Dietary Intake and Association with BMI
The median daily meal frequency was 5, primarily administered orally (80%) with mushy food consistency (57.8%). Median cereal intake was 22.5%, and fruit intake was 25%. Consumption of ultra-processed foods was frequent (58%), while only 34.2% of children achieved minimum dietary diversity. No significant differences in dietary patterns were identified between children with adequate or inadequate BMI (Table 5).
Macronutrient analysis showed a significant association between inadequate carbohydrate intake and inadequate BMI (p=0.030). No associations were observed between protein or lipid intake and BMI. Caloric intake was inadequate for 85% of the children, and more than 90% presented low intake of essential micronutrients, including zinc, calcium, iron, and vitamin D, without significant associations with BMI status (Table 6).
4. Discussion
Authors should discuss the results and how they can be interpreted from the perspective of previous studies and of the working hypotheses. The findings and their implications should be discussed in the broadest context possible. Future research directions may also be highlighted.
The long-term consequences of CZVS on child growth and nutrition remain insufficiently characterized, despite the well-established neurological impairments associated with the condition. In this cohort, a distinct anthropometric pattern was observed—characterized by significant gains in height over time without proportional increases in weight or BMI. This disproportion suggests underlying compensatory biological mechanisms, potentially involving endocrine or metabolic adaptations commonly seen in chronic conditions or in contexts of sustained nutritional inadequacy [20]. Such findings highlight the complexity of growth trajectories in children with CZVS and raise concerns about the adequacy of their overall nutritional status, even when linear growth appears preserved.
The discrepancy between improved linear growth and stagnation in weight underscores important limitations in the scope and effectiveness of current multidisciplinary care. While stature gains may be attributed to sustained medical follow-up and rehabilitation, the persistence of suboptimal weight and BMI values suggests that nutritional components of care are either insufficiently addressed or inadequately tailored to the specific needs of this population. Moreover, structural socioeconomic constraints—including poverty, unemployment, food insecurity, and restricted access to specialized nutritional resources—likely contribute to persistent dietary inadequacies. These factors not only influence food availability and quality but also shape feeding practices and caregiver decision-making, thereby compounding the biological and developmental vulnerabilities associated with CZVS [8,21,22].
Dietary assessments revealed marked nutritional inadequacies, including limited dietary diversity, high consumption of ultra-processed foods, and low fruit intake. These patterns are consistent with food insecurity and structural poverty, which have been previously associated with adverse nutritional and developmental outcomes in children with neurodevelopmental disorders. In the context of CZVS, these conditions are further exacerbated by the chronic demands of caregiving and restricted autonomy of affected children during feeding [7]. Evidence from similar populations supports the effectiveness of multifaceted interventions that combine caregiver education, nutritional counseling, food supplementation, and psychosocial support in improving dietary quality and functional outcomes [23]. Implementing such strategies in the routine care of children with CZVS may mitigate both biological and social determinants of nutritional risk.
Neurological impairments in CZVS frequently result in dysphagia and oromotor dysfunctions, which complicate nutritional management and require individualized interventions, including texture modifications, alternative feeding techniques, and continuous support from speech-language pathologists. These adaptations are essential not only to ensure adequate caloric and nutrient intake but also to prevent respiratory complications such as aspiration pneumonia [24,25]. Furthermore, the chronic use of anticonvulsants—fundamental in seizure control—has been associated with anorexia, changes in taste perception, and gastrointestinal side effects, all of which can disrupt feeding routines and further compromise nutritional status [26,27]. In parallel, limited caregiver knowledge about age-appropriate dietary practices, combined with socioeconomic challenges, may result in suboptimal feeding behaviors. These findings reinforce the importance of caregiver-centered educational initiatives aimed at building capacity for safe, effective, and developmentally appropriate nutritional care [28].
This study has some limitations. Its single-center design may limit external validity, as the sample may not capture the heterogeneity of children with CZVS across diverse sociocultural and geographic contexts. In addition, the use of only two 24-hour dietary recalls may not fully reflect habitual intake, increasing the possibility of misclassification or recall bias. Future research should prioritize multicenter longitudinal studies that encompass broader demographic variability, allowing for more generalizable conclusions. Moreover, integrating more comprehensive dietary assessment tools, such as repeated recalls or food diaries, would yield more accurate estimates of intake patterns. Evaluating the long-term impact of targeted nutritional interventions—particularly those addressing social vulnerability and feeding-related impairments—will be critical to inform policy and clinical strategies aimed at improving health trajectories in this highly vulnerable population.
5. Conclusions
This study demonstrated that children with CZVS present persistent nutritional inadequacies and suboptimal anthropometric development, evidenced by insufficient weight gain despite improvements in stature. Dietary profiles were characterized by excessive intake of ultra-processed foods and limited diversity, reflecting both neurological impairments and socioeconomic adversity. These findings underscore the need for comprehensive public health strategies that integrate medical, nutritional, educational, and social support. Interventions tailored to the complex needs of this population are essential to reduce nutritional deficits, promote healthy growth, and improve long-term health and quality of life.
Author Contributions
Conceptualization, C.S.S.T., R.S.M., M.C.S.R., and P.R.M.F.; methodology, C.S.S.T., R.S.M., J.S.F.; M.B.B.O., M.C.S.R., and P.R.M.F.; investigation, C.S.S.T., and R.S.M; formal analysis, C.S.S.T., C.S.S.T., J.S.F., M.B.B.O., and P.R.M.F.; supervision, M.C.S.R., and P.R.M.F.; writing—original draft preparation, C.S.S.T., and R.S.M; writing—review and editing, C.S.S.T., R.S.M., J.S.F.; M.B.B.O., M.C.S.R., and P.R.M.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of Federal University of Sergipe (approval no. 5.287.146).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to privacy and ethical restrictions but are available from the corresponding author upon reasonable request.
Acknowledgments
P.R.M.F. is a productivity fellow at the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq). C.S.S.T. and R.S.M. thank the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES) for their scholarship. J.S.F. thanks the Fundação de Apoio à Pesquisa e à Inovação Tecnológica do Estado de Sergipe (Fapitec/SE) for her scholarship.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CZVS | Congenital Zika Virus Syndrome |
| ZIKV | Zika Virus |
| HU-UFS | University Hospital of Sergipe |
| SUS | Sistema Único de Saúde |
| CHB | Child Health Booklet |
| WHO | World Health Organization |
| AMDR | Acceptable Macronutrient Distribution Range |
| RDA | Recommended Dietary Allowance |
| BMI | Body Mass Index |
| IQR | Interquartile Range |
References
- Costa, F.; Sarno, M.; Khouri, R.; de Paula Freitas, B.; Siqueira, I.; Ribeiro, G.S.; Ribeiro, H.C.; Campos, G.S.; Alcântara, L.C.; Reis, M.G.; et al. Emergence of Congenital Zika Syndrome: Viewpoint From the Front Lines. Ann. Intern. Med. 2016, 164, 689. [Google Scholar] [CrossRef] [PubMed]
- Moore, C.A.; Staples, J.E.; Dobyns, W.B.; Pessoa, A.; Ventura, C. V.; Fonseca, E.B. da; Ribeiro, E.M.; Ventura, L.O.; Neto, N.N.; Arena, J.F.; et al. Characterizing the Pattern of Anomalies in Congenital Zika Syndrome for Pediatric Clinicians. JAMA Pediatr. 2017, 171, 288. [Google Scholar] [CrossRef] [PubMed]
- Alves, L. V; Paredes, C.E.; Silva, G.C.; Mello, J.G.; Alves, J.G. Neurodevelopment of 24 Children Born in Brazil with Congenital Zika Syndrome in 2015: A Case Series Study. BMJ Open 2018, 8, e021304. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.; Brites, C.; Mochida, G.; Ventura, P.; Fernandes, A.; Lage, M.L.; Taguchi, T.; Brandi, I.; Silva, A.; Franceschi, G.; et al. Clinical and Neurodevelopmental Features in Children with Cerebral Palsy and Probable Congenital Zika. Brain Dev. 2019, 41, 587–594. [Google Scholar] [CrossRef]
- Vianna, R.A. de O.; Lovero, K.L.; Oliveira, S.A. de; Fernandes, A.R.; Santos, T.C.S. dos; Lima, L.C.S. de S.; Carvalho, F.R.; Quintans, M.D.S.; Bueno, A.C.; Torbey, A.F.M.; et al. Children Born to Mothers with Rash During Zika Virus Epidemic in Brazil: First 18 Months of Life. J. Trop. Pediatr. 2019, 65, 592–602. [Google Scholar] [CrossRef]
- de Paula, G.L.; da Silva, G.A.P.; e Silva, E.J. da C.; Lins, M. das G.M.; Martins, O.S. de S.; Oliveira, D.M. da S.; Ferreira, E. de S.; Antunes, M.M. de C. Vomiting and Gastric Motility in Early Brain Damaged Children With Congenital Zika Syndrome. J. Pediatr. Gastroenterol. Nutr. 2022, 75, 159–165. [Google Scholar] [CrossRef]
- de Oliveira, A.M.M.; de Melo, E.G.M.; Mendes, M.L.T.; dos Santos Oliveira, S.J.G.; Tavares, C.S.S.; Vaez, A.C.; de Vasconcelos, S.J.A.; Santos, H.P.; Santos, V.S.; Martins-Filho, P.R.S. Oral and Maxillofacial Conditions, Dietary Aspects, and Nutritional Status of Children with Congenital Zika Syndrome. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 130, 71–77. [Google Scholar] [CrossRef]
- dos Santos, S.F.M.; Soares, F.V.M.; de Abranches, A.D.; da Costa, A.C.C.; Moreira, M.E.L.; de Matos Fonseca, V. Infants with Microcephaly Due to ZIKA Virus Exposure: Nutritional Status and Food Practices. Nutr. J. 2019, 18, 4. [Google Scholar] [CrossRef]
- França, T.; Medeiros, W.; Souza, N.; Longo, E.; Pereira, S.; França, T.; Sousa, K. Growth and Development of Children with Microcephaly Associated with Congenital Zika Virus Syndrome in Brazil. Int. J. Environ. Res. Public Health 2018, 15, 1990. [Google Scholar] [CrossRef]
- Martinez, S.S.; Pardo-Hernandez, H.; Palacios, C. Feeding Modifications and Additional Primary Caregiver Support for Infants Exposed to Zika Virus or Diagnosed with Congenital Zika Syndrome: A Rapid Review of the Evidence. Trop. Med. Int. Heal. 2020, 25, 1353–1361. [Google Scholar] [CrossRef]
- Oliveira, S.J.G. de; Tavares, C.S.S.; Santos, V.S.; Santos Jr, H.P.; Martins-Filho, P.R. Anxiety, Depression, and Quality of Life in Mothers of Children with Congenital Zika Syndrome: Results of a 5-Year Follow-up Study. Rev. Soc. Bras. Med. Trop. 2022, 55, e06272021. [Google Scholar] [CrossRef] [PubMed]
- Brasil Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Ações Programáticas e Estratégicas. Protocolo de Vigilância e Resposta à Ocorrência de Microcefalia Relacionada à Infecção Pelo Vírus Zika: Plano Nacional de Enfrentamento à Microcefalia; 2015.
- Stevenson, R.D. Use of Segmental Measures to Estimate Stature in Children With Cerebral Palsy. Arch. Pediatr. Adolesc. Med. 1995, 149, 658. [Google Scholar] [CrossRef] [PubMed]
- WHO World Health Organization. Screening, Assessment and Management of Neonates and Infants with Complications Associated with Zika Virus Exposure in Utero; 2016.
- Brasil Ministério da Saúde. Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Coordenação-Geral da Política de Alimentação e Nutrição. Incorporação da Curvas de Crescimento da Organização Mundial da Saúde de 2006 e 2007 no SISVAN; 2007.
- Freudenheim, J.L. A Review of Study Designs and Methods of Dietary Assessment in Nutritional Epidemiology of Chronic Disease. J. Nutr. 1993, 123, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Culley, W.J.; Middleton, T.O. Caloric Requirements of Mentally Retarded Children with and without Motor Dysfunction. J. Pediatr. 1969, 75, 380–384. [Google Scholar] [CrossRef]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; Poos, M. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein and Amino Acids. J. Am. Diet. Assoc. 2002, 102, 1621–1630. [Google Scholar] [CrossRef]
- NRC National Research Council. Recommended Dietary Allowances: 10th Edition; National Academies Press: Washington, D.C., 1989; ISBN 978-0-309-04633-6. [Google Scholar]
- Victora, C.G.; Adair, L.; Fall, C.; Hallal, P.C.; Martorell, R.; Richter, L.; Sachdev, H.S. Maternal and Child Undernutrition: Consequences for Adult Health and Human Capital. Lancet 2008, 371, 340–357. [Google Scholar] [CrossRef]
- Black, R.E.; Victora, C.G.; Walker, S.P.; Bhutta, Z.A.; Christian, P.; de Onis, M.; Ezzati, M.; Grantham-McGregor, S.; Katz, J.; Martorell, R.; et al. Maternal and Child Undernutrition and Overweight in Low-Income and Middle-Income Countries. Lancet 2013, 382, 427–451. [Google Scholar] [CrossRef]
- Penagini, F.; Mameli, C.; Fabiano, V.; Brunetti, D.; Dilillo, D.; Zuccotti, G. Dietary Intakes and Nutritional Issues in Neurologically Impaired Children. Nutrients 2015, 7, 9400–9415. [Google Scholar] [CrossRef]
- Grantham-McGregor, S.; Cheung, Y.B.; Cueto, S.; Glewwe, P.; Richter, L.; Strupp, B. Developmental Potential in the First 5 Years for Children in Developing Countries. Lancet 2007, 369, 60–70. [Google Scholar] [CrossRef]
- Leal, M.C.; van der Linden, V.; Bezerra, T.P.; de Valois, L.; Borges, A.C.G.; Antunes, M.M.C.; Brandt, K.G.; Moura, C.X.; Rodrigues, L.C.; Ximenes, C.R. Characteristics of Dysphagia in Infants with Microcephaly Caused by Congenital Zika Virus Infection, Brazil, 2015. Emerg. Infect. Dis. 2017, 23, 1253–1259. [Google Scholar] [CrossRef]
- Lefton-Greif, M.A.; Arvedson, J.C. Schoolchildren With Dysphagia Associated With Medically Complex Conditions. Lang. Speech. Hear. Serv. Sch. 2008, 39, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Buraniqi, E.; Dabaja, H.; Wirrell, E.C. Impact of Antiseizure Medications on Appetite and Weight in Children. Pediatr. Drugs 2022, 24, 335–363. [Google Scholar] [CrossRef] [PubMed]
- Carvalho-Sauer, R.; Costa, M. da C.N.; Barreto, F.R.; Teixeira, M.G. Congenital Zika Syndrome: Prevalence of Low Birth Weight and Associated Factors. Bahia, 2015–2017. Int. J. Infect. Dis. 2019, 82, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Rabinowitz, D.G. When Failure to Thrive Is About Our Failures: Reflecting on Food Insecurity in Pediatrics. Hosp. Pediatr. 2022, 12, e213–e215. [Google Scholar] [CrossRef]
Figure 1.
Anthropometric curves of children with CZVS from birth to the end of early childhood for height (a), weight (b), and BMI (c).
Figure 1.
Anthropometric curves of children with CZVS from birth to the end of early childhood for height (a), weight (b), and BMI (c).
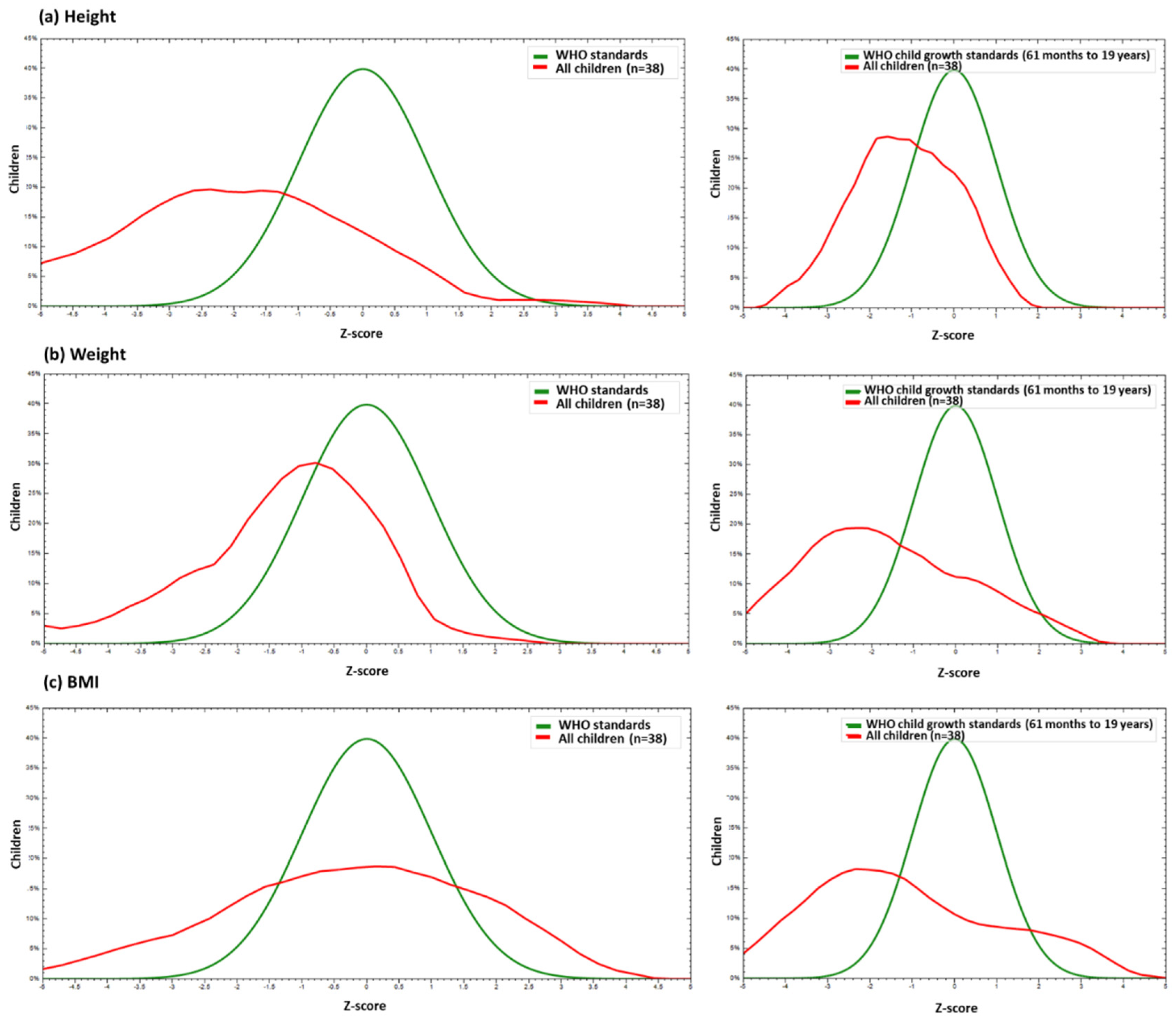

Table 1.
Cutoff points for weight, height, and body mass index.
| Measures | Critical values | Diagnosis |
|---|---|---|
|
Weight |
Percentile > 97/ Z-score > +2 | High weight for age. |
| Percentile > 3 and 97/ Z-score > -2 and +2 | Adequate weight for age. | |
| Percentile > 0.1 and < 3/ Z-score > -3 and < -2 | Low weight for age. | |
| Percentile < 0.1/ Z-score < -3 | Very low weight for age. | |
|
Height |
||
| Percentile > 3/ Z-score > +2 Z-score > -2 and +2 | Adequate height for age. | |
| Percentile > 0.1 and < 3/ Z-score > -3 and < -2 | Short stature for age. | |
| Percentile < 0.1/ Z-score < -3 | Very short stature for age. | |
|
BMI |
Percentile > 99.9/ Z-score > +3 | Obesity. |
| Percentile > 97 and 99.9/ Z-score +2 and +3 | Overweight. | |
| Percentile > 85 and 97/ Z-score > +1 and < +2 | Risk of overweight. | |
| Percentile > 3 and 85/ Z-score > -2 and +1 | Adequate BMI. | |
| Percentile > 0.1 and < 3/ Z-score > -3 and < -2 | Underweight. | |
| Percentile < 0.1/ Z-score < -3 | Severe underweight. |
BMI, body mass index.
Table 2.
Socioeconomic and obstetric characteristics of mothers of children with CZS.
| Variable | % (n) |
|---|---|
|
Age* Area of residence Rural Urban |
31.0 (25.0-37.0) 39.5% (15) 60.5% (23) |
|
Marital status Married/in a stable relationship Divorced/single |
78.9% (30) 21.1% (8) |
| Employed | |
| Yes | 21.1% (8) |
| No | 78.9% (30) |
|
Government benefit Yes No |
92.1% (35) 7.9% (3) |
| Monthly family income | |
| Less than 1 minimum wage | 5.3% (2) |
| From 1 to 3 minimum wages | 94.7% (36) |
| Number of births* | 2.0 (1.5-3.0) |
| Live births* | 2.0 (1.0-3.0) |
| Miscarriages* | 0.0 (0.0-0.0) |
|
Pregnancy wanted Yes No |
42.1% (16) 57.9% (22) |
|
Prenatal Yes Type of delivery Vaginal Cesarean |
100% (38) 55.3% (21) 44.7% (17) |
* Data reported as median (Q1-Q3).
Table 3.
Neonatal history and current data of children with CZVS.
| Variable | % (n) |
|---|---|
| Sex | |
| Male | 52.6% (20) |
| Female | 47.4% (18) |
| Apgar 1º minute* | 9.0 (8.0-9.0) |
| Apgar 5º minute* | 10.0 (9.0-10.0) |
| Head circumference at birth* | 29.0 (27.5-30.0) |
| Severe microcephaly | |
| Yes | 81.6% (31) |
| No | 18.4% (7) |
| Current age | 6.3 (5.9-6.6) |
| Current head circumference* | 44.5 (42.0- 45.9) |
| Complications | |
| Arthrogryposis | 42.1% (16) |
| Seizure | 84.2% (32) |
| Dysphagia | 6.1% (23) |
| Ophthalmological disorders | 42.1% (16) |
| Hearing disorders | 23.7% (9) |
| Hypertonia | 39.5% (15) |
| Hyperreflexia | 7.9% (3) |
| Irritability | 31.6% (12) |
| Neurogenic bladder | 2.6% (1) |
| Need for hospitalization | |
| Yes | 63.2% (24) |
| No | 36.8% (14) |
| Currently attends school | |
| Yes | 21.1% (8) |
| No | 79.9% (30) |
* Data reported as median (Q1-Q3).
Table 4.
Longitudinal analysis of anthropometric measures (height, weight, and BMI) of 38 children with CZVS.
Table 4.
Longitudinal analysis of anthropometric measures (height, weight, and BMI) of 38 children with CZVS.
| Measures | Birth | End of 1st childhood | Diagnostic Evolution | p-value(a) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Median (IQR) |
Adequate parameters for age (%) | Median (IQR) |
Adequate parameters for age (%) |
Remained adequate |
Improved | Remained Inadequate |
Worsened | ||
| Height (cm) | 45.0 (43.0 – 48.0) |
16 (42.1) |
108.8 (106.6 – 117.5) |
29 (76.3) |
12 (31.6) |
17 (44.8) |
5 (13.1) |
4 (10.5) |
0.007* |
|
Weight (Kg) |
2.7 (2.5 – 3.0) |
28 (73.7) |
15.8 (14.3 – 18.7) |
22 (57.9) |
16 (42.1) |
6 (15.8) |
4 (10.5) |
12 (31.6) |
0.238 |
| BMI | 13.0 (11.5 – 14.6) |
28 (73.7) |
13.2 (11.8 – 15.0) |
16 (42.1) |
11 (29.0) |
5 (13.1) |
5 (13.1) |
17 (44.8) |
0.017* |
BMI, body mass index. (a) McNemar test. *p-values less than or equal to 0.05 were considered statistically significant.
Table 5.
General dietary consumption characteristics of children with CZVS.
| Variables | % (n) | Adequate BMI (n = 16) |
Inadequate BMI (n = 22) |
p-value(a) |
|---|---|---|---|---|
| Daily number of meals* | 5.0 (4.5-6.0) | 5.0 (4.6-5.9) | 5.3 (4.4-6.0) | 0.848 |
| Food intake | ||||
| Oral | 80.0% (30) | 68.8% (11) | 86.4% (19) | 0.243 |
| Enteral | 20.0% (8) | 31.2% (5) | 13.6% (3) | |
| Consistency of food | ||||
| Solid | 21.1% (8) | 18.8% (3) | 22.7% (5) | 0.450 |
| Liquid | 21.1% (8) | 31.2% (5) | 13.6% (3) | |
| Mushy | 57.8% (22) | 50.0 (8) | 63.7% (14) | |
| % of meals with cereals* | 22.5% (2.3-37.2) | 15.5% (0.0-30.1) | 26.2% (11.1-37.2) | 0.359 |
| % of meals with fruits* | 25.0% (17.1-36.4) | 25.0% (17.2-37.3) | 26.8% (17.1-35.6) | 0.906 |
| Ultra-processed food consumption | ||||
| Yes | 58.0% (22) | 56.3% (9) | 59.1% (13) | 1.000 |
| No | 42.0% (16) | 43.7% (7) | 40.9% (9) | |
| Minimum dietary diversity | ||||
| Yes | 34.2% (13) | 25.0% (4) | 40.9% (9) | 0.490 |
| No | 65.8% (25) | 75.0% (12) | 59.1% (13) |
* Data reported as median (Q1-Q3). (a) Mann-Whitney or Fisher’s exact test. BMI, body mass index.
Table 6.
Macronutrient and micronutrient intake of children with CZVS.
| Variables | % (N) | Adequate BMI (n = 16) |
Inadequate BMI (n = 22) |
p-value(a) |
|---|---|---|---|---|
| Kcal | ||||
| Adequate | 15.8% (6) | 6.3% (1) | 22.7% (5) | 0.370 |
| Inadequate | 84.2% (32) | 93.7% (15) | 77.3% (17) | |
| Macronutrients | ||||
| Proteins | ||||
| Adequate | 47.4% (18) | 50.0% (8) | 45.5% (10) | 1.000 |
| Inadequate | 52.6% (20) | 50.0% (8) | 54.5% (12) | |
| Carbohydrates | ||||
| Adequate | 84.2% (32) | 100.0% (16) | 72.7% (16) | 0.030¥ |
| Inadequate | 15.8% (6) | 0.0% (0) | 27.3% (6) | |
| Lipids | ||||
| Adequate | 52.6% (20) | 50.0% (8) | 54.5% (12) | 1.000 |
| Inadequate | 47.4% (18) | 50.0% (8) | 45.5% (10) | |
| Micronutrients | ||||
| Zinc | ||||
| Adequate | 10.5% (4) | 6.3% (1) | 13.6% (3) | 0.625 |
| Inadequate | 89.5% (34) | 93.7% (15) | 86.4% (19) | |
| Calcium | ||||
| Adequate | 2.6% (1) | 6.3% (1) | 0.0% (0) | 0.421 |
| Inadequate | 97.4% (37) | 93.7% (15) | 100.0% (22) | |
| Iron | ||||
| Adequate | 10.5% (4) | 6.3% (1) | 13.6% (3) | 0.625 |
| Inadequate | 89.5% (34) | 93.7% (15) | 86.4% (19) | |
| Vitamin D | ||||
| Adequate | 0.0% (0) | 0.0% (0) | 0.0% (0) | 1.000 |
| Inadequate | 100.0% (38) | 100.0% (16) | 100.0% (22) |
(a) Fisher’s exact test. ¥ p-values less than 0.05 were considered statistically significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



