
Submitted:
30 April 2025
Posted:
02 May 2025
You are already at the latest version
Abstract
Background and Objectives: This study examines the distinction between gamification and Digital Game-Based Learning (DGBL) in health education, introducing the iLearn4Health platform designed to enhance health literacy among primary school students aged 6-12. The research investigates how DGBL's integration of educational content into gameplay mechanics affects user engagement and learning outcomes compared to superficial gami-fication approaches. Materials and Methods: Developed through international collaboration across five European countries, the iLearn4Health platform features six health-focused modules with age-appropriate content and multilingual support. The study analyzed platform usage data from 337 teachers across 24 schools, tracking engagement metrics, including complete steps, progress ratios, and time spent. Multiple statistical approach-es—descriptive analysis, correlation analysis, ANOVA, regression modeling, and cluster analysis—were employed to identify engagement patterns and their predictors. Results: Analysis revealed a distinctive bimodal distribution of user progress, with 52.8% showing low engagement (progress ratio 0.0-0.2) and 35.3% demonstrating high engagement (pro-gress ratio 0.8-1.0). A strong positive correlation (r=.95, p< .001) between time spent and steps completed indicated that sustained engagement predicted educational progression. Multiple regression analysis identified initial engagement as the strongest predictor of overall progress (β=0.479, p< .001), followed by country effects (Romania vs. Cyprus, β=0.183, p=.001) and age (β=0.108, p=.049). Cluster analysis revealed three distinct user profiles: high engagers (35.3%, n=119), early dropouts (52.8%, n=178), and selective en-gagers (11.9%, n=40). Cross-country analysis showed significant variations in platform engagement, with Romania demonstrating 53% higher average progress ratios than Cy-prus (0.460 vs. 0.301, p< .01). Conclusions: The iLearn4Health platform reflects the effec-tiveness of DGBL—distinct from gamification—for health education in primary schools. The platform supports knowledge acquisition and behavioral change by integrating health concepts directly into age-appropriate game environments rather than merely adding game elements to existing content. Identifying initial engagement as the strongest predictor of overall progress highlights the critical importance of early user experience in determining educational outcomes. The platform's comprehensive approach to DGBL in primary health education establishes a framework for creating effective digital interven-tions that recognize the unique developmental needs of primary school children while adapting to diverse educational contexts.
Keywords:
Digital Game-Based Learning (DGBL)
; health education
; primary school students
; cross-national implementation
; user engagement analytics
; developmental design
; health literacy
; educational technology
; multilingual educational games
; health behavior promotion
1. Introduction
In recent years, educational and health sectors have increasingly incorporated game elements into their practices, albeit through distinct approaches that merit clear differentiation. Gamification—the application of game-design elements to non-game contexts—differs fundamentally from Digital Game-Based Learning (DGBL), which employs complete games explicitly designed for educational purposes. This critical distinction establishes the framework for our investigation [1,2,3,4].
Gamification typically incorporates standard mechanics such as points, leaderboards, rewards, and levels into non-gaming environments to enhance user motivation and engagement [5,6,7]. Since approximately 2010, gamification has gained significant traction across multiple domains, including education, marketing, and public health. By contrast, DGBL involves comprehensive game experiences specifically developed to achieve learning objectives, where educational content is intrinsically woven into gameplay mechanics [8,9,10,11].
The education sector has embraced both approaches, with gamification elements enhancing traditional learning platforms and DGBL offering immersive educational experiences. Similarly, the health promotion field has adopted these strategies—gamification appears in behavior-tracking applications and incentive systems, while health-focused games deliver educational content through interactive narratives and simulations [12,13,14].
Despite growing interest in both fields, there remains a significant gap in research that systematically differentiates and compares these approaches across educational and health contexts [15,16,17]. Current literature often conflates or treats these distinct concepts in isolation without cross-domain analysis. This lack of conceptual clarity hinders the development of effective theoretical frameworks that could inform design practices in both fields [18,19,20].
Our research examines explicitly the iLearn4Health platform, an online DGBL tool designed to develop health literacy and promote healthy behaviors among primary school students. This platform features modules addressing Healthy Dietary Habits, Physical Activity, Stereotypes, Accident Prevention, Internet Safety, and Sexual Health Education. Unlike gamified applications that merely add game elements to existing content, iLearn4Health represents a comprehensive educational game environment where health concepts are integrated into the core gameplay [21].
This study aims to analyze how DGBL specifically—rather than gamification broadly—contributes to health education outcomes. By establishing clear theoretical boundaries between gamification and DGBL, we can more accurately assess how game-based interventions enhance engagement and learning in health education contexts. Furthermore, we investigate how data-driven insights can inform iterative design processes that align educational games with broader health promotion frameworks [22,23,24,25].
Through this focused approach, we contribute to a more nuanced understanding of how game-based strategies—specifically gamification and DGBL—can effectively support educational objectives in health promotion contexts. This clarity addresses a critical need in the literature for theoretical precision when discussing game-related interventions across these intersecting fields [26,27,28,29].
2. Literature Review
2.1. Theoretical Frameworks Distinguishing Gamification and DGBL in Education and Health Promotion
Theoretical underpinnings that distinguish gamification and Digital Game-Based Learning (DGBL) are essential for effective application in both educational and health settings [30,31,32]. Gamification heavily borrows from motivational theories and, more specifically, Self-Determination Theory (SDT), which postulates autonomy, competence, and relatedness as basic psychological needs. When game design mechanics like points, badges, and leaderboards are translated into non-game settings, they can potentially facilitate or undermine these inherent motivational needs [33,34,35,36].
On the other hand, DGBL has stronger roots in constructivist learning theory, in which learning is achieved through experience and problem-solving in whole game worlds [37,38]. Whereas gamification incorporates game mechanics into existing tasks, DGBL incorporates curricular material into the gameplay itself, with an opportunity to engage more deeply with learning content [39,40,41].
In health promotion specifically, both the Theory of Planned Behavior (TPB) and Social Cognitive Models provide frameworks through which both approaches can influence health behaviors in different ways [42,43,44]. Gamification targets specific behavior through the use of extrinsic rewards, while DGBL can potentially create immersive storylines that embed health concepts into significant experiences [45,46,47].
Research with primary school populations, the specific target demographic for the iLearn4Health platform—demonstrates particular developmental considerations that af-fect the efficacy of both approaches [48,49,50]. Children aged 6-12 respond differently to game elements than adolescents or adults, with greater responsiveness to visual rewards, narrative engagement, and playful interactions. This developmental distinction is critical when designing interventions specifically for primary school students versus general populations, as the cognitive and motivational processes differ substantially across age groups [51,52,53].
Experimental comparisons between minimally gamified applications and those with comprehensive game elements demonstrate that theoretical grounding significantly impacts outcomes [54,55,56]. These comparisons reveal that superficial implementation of game elements without consideration of age-appropriate motivational factors often fails to produce sustained engagement, particularly among primary school children who require more concrete and immediate feedback systems than adult users [57,58,59].
2.2. Design Principles for Effective Gamification Versus DGBL in Primary School Health Education
The design principles for gamification differ substantially from those for DGBL, particularly when targeting primary school children for health education. User-centered design takes on heightened importance with younger populations, as their cognitive abilities, attention spans, and motivational triggers vary significantly from adolescents or adults [60,61].
For gamification approaches with primary school children, effective design principles include: (1) immediate and concrete feedback mechanisms, (2) simple reward structures that avoid overwhelming cognitive load, (3) age-appropriate challenges that match developmental capabilities, and (4) social comparison elements calibrated to minimize adverse competitive effects. These principles address the specific needs of younger learners whose abstract thinking and self-regulatory capacities are still developing [62].
DGBL design for this age group, however, emphasizes different principles: (1) narrative integration that contextualizes health concepts within engaging stories, (2) experiential learning through role-playing and simulation, (3) scaffolded progression that matches developing abilities, and (4) multimodal representation of concepts through visual, auditory, and kinesthetic channels [63,64].
The iLearn4Health platform specifically implements DGBL principles for primary school students through modules designed with age-appropriate complexity, vocabulary, and interactions. Each health topic—dietary habits to internet safety—is presented through developmentally appropriate gameplay rather than simply adding game elements to traditional educational content [65].
Effective design in both approaches requires alignment between the chosen strategy (gamification or DGBL), the developmental stage of the target users (primary school children), and the specific health promotion objectives. This alignment ensures that the intervention addresses both the cognitive capabilities and motivational factors relevant to the target age group [66,67,68,69].
2.3. Implementation Technologies for Primary School Health Education: Gamification Tools Versus Complete DGBL Platforms
The technological implementation of gamification differs substantially from DGBL platforms, particularly when designed for primary school populations. Gamification typically employs add-on elements to existing systems through points, badges, and leaderboards, while DGBL requires comprehensive game development environments that integrate educational content directly into gameplay [70,71,72].
For primary school settings, technological considerations include age-appropriate user interfaces, data protection measures specific to minors, and scalability across varying school infrastructure capabilities. These considerations are particularly relevant for the iLearn4Health platform, which must function effectively within the technological constraints typical of primary education environments [73,74,75].
Web-based, social media-based, and video-interactive platforms offer different affordances for implementing both approaches. However, their suitability varies significantly when targeting primary school children versus general populations. Platforms designed for younger users require simplified navigation, larger interface elements, more visual cues, and stricter privacy controls than those designed for adolescents or adults [76,77,78,79].
Technical limitations particular to primary school settings include restricted internet bandwidth, varying device availability, and institutional filtering systems. The iLearn4Health platform addresses these constraints through optimized content delivery, cross-platform compatibility, and offline functionality options that accommodate the specific technological ecosystem of primary education [80].
User experience research with primary school children demonstrates that technical frustrations—such as buffering videos or complicated login procedures—significantly impact engagement among younger users, who have a lower tolerance for technical friction than adult users [81,82,83]. Successful implementation in primary education settings requires platforms specifically designed for these constraints rather than adapting tools originally designed for older populations [84,85,86,87].
Recently developed off-the-shelf gamification platforms offer quick implementation options, but many lack specific customization for primary school environments and health education objectives. The iLearn4Health platform, by contrast, was purpose-built for this particular intersection of user age, educational context, and health promotion goals, addressing the particular developmental needs of primary school children [88,89,90,91].
From both educational and technological perspectives, the distinction between adding game elements to existing health education (gamification) and developing complete educational games about health (DGBL) remains crucial—particularly when designing for specific age groups like primary school children, where developmental considerations substantially influence effectiveness [92,93,94,95,96].
3. Materials and Methods
3.1. Platform Development Framework
The iLearn4Health platform (accessible at https://game.ilearn4health.eu/) constitutes a web-based Digital Game-Based Learning (DGBL) application specifically developed for primary school students aged 6-12. The platform encompasses six integrated educational games focusing on critical health topics: Healthy Dietary Habits, Be-Active-Train Yourself, Stereotypes, Accidents, Internet Addiction, and Sexual Health. These games were developed through the G.A.M.E.D. (digital educational game development methodology) framework, ensuring pedagogical alignment with primary school curricular objectives while maintaining developmentally appropriate content and interactions.
The development consortium comprised eight partner institutions from Greece, Cyprus, Romania, Poland, and Spain, integrating multidisciplinary expertise across education, health promotion, and digital development domains. Notably, although English is not the primary language in any consortium country, the platform incorporated comprehensive multilingual functionality from its inception. All educational content underwent professional translation and cultural localization into Greek, Romanian, Polish, and Spanish to ensure linguistic accessibility and cultural appropriateness for target populations in participating countries. This multilingual implementation represented a fundamental design requirement rather than a secondary consideration, enabling students to engage with health education content in their native languages despite the platform screenshots appearing in English in this publication for international dissemination purposes.
Development followed an Agile methodology, characterized by iterative feedback loops incorporating insights from educators, health professionals, and—crucially—primary school students throughout all design and testing phases. This approach facilitated continuous refinement of interface elements and educational content to optimize alignment with pedagogical principles and age-appropriate health promotion objectives for the specific developmental stages targeted within the 6-12 age range.
3.2. Study Design and Participant Selection
Our investigation employed a mixed-methods research design to evaluate the effectiveness of the iLearn4Health platform as a Digital Game-Based Learning (DGBL) intervention in health education among primary school students. The implementation spanned 24 schools across five countries (Greece, Cyprus, Romania, Poland, and Spain), applying purposeful and stratified sampling to ensure contextual diversity—encompassing rural and urban environments, varied socioeconomic backgrounds, and differing levels of digital infrastructure.
The study engaged 337 teachers, significantly expanding the initial scope of educator involvement. This larger cohort provided a robust dataset for analyzing platform engagement and implementation variability. Participating teachers represented various professional backgrounds, ages, and subject specializations, reflecting authentic diversity within European primary education systems.
Teacher demographics were incorporated into subgroup analyses, including age distribution (ranging from the early 20s to late 60s), national context, and digital engagement patterns (captured through platform analytics). These data enabled us to explore the impact of variables such as technological proficiency and teaching experience on platform integration. The teachers completed training and interacted with the platform over an extended period, generating detailed data on steps completed (reaching 53 out of 55 steps) and time spent (ranging from under an hour to multiple days), reflecting both high engagement and substantial variability.
In addition to the primary teacher cohort, a comparative control group of 120 out of the total sample (n=337) adults aged 18–65 was studied to isolate developmental factors affecting DGBL engagement. The adult group demonstrated peak engagement in the 36–50 age bracket (averaging 23.4 steps and 45 minutes), a finding that informed refinements to design features tailored for younger learners. Correlation analysis revealed that age and time spent were strongly predictive of steps completed (r = 0.95 for time spent vs. progress), underscoring the importance of sustained interaction and developmentally aligned design.
The expanded teacher dataset (n=337) provided critical insights into how DGBL implementation is influenced by educator characteristics, highlighting the need for differentiated support strategies during deployment. This revised study design—now incorporating broader teacher participation and cross-demographic analytics—offers a more comprehensive foundation for evaluating the scalability and contextual adaptability of DGBL interventions in health education.
3.3. Data Collection and Analysis
This study implemented a data-driven evaluation framework focused on the digital engagement and progression of n=337 teacher participants across five countries. Data collection relied entirely on quantitative measures drawn from the iLearn4Health platform’s integrated analytics, capturing detailed behavioral interactions with the Digital Game-Based Learning (DGBL) environment.
Key metrics included:
- Steps Completed: The platform’s modular structure consisted of 55 instructional steps. The majority of teachers completed 53 or more steps, indicating high task completion rates across the cohort.
- Total Time Spent: Time-on-platform varied substantially—from a few minutes to multiple days—reflecting diverse usage patterns and levels of engagement. A small subset of users accounted for disproportionately high usage, with time spent exceeding 85 hours in extreme cases.
- Progress Ratios: A normalized metric (steps completed / total steps) was used to compare engagement across users. This revealed a bimodal distribution: a large cluster of users completed most of the platform, while another cluster disengaged early.
- Engagement Patterns by Demographics: Correlation analysis revealed strong positive relationships between age and both time spent (r = 0.60) and steps completed (r = 0.80). The strongest correlation was observed between steps completed and time spent (r = 0.95), emphasizing the importance of sustained interaction for educational progression.
The data also enabled country-level comparisons of average progress ratios, revealing contextual factors influencing teacher engagement, such as national differences in digital readiness, familiarity with game-based methods, or institutional support.
This analytic framework supported the evaluation of platform effectiveness, informing recommendations for targeted improvements in onboarding, module design, and user retention strategies. By leveraging a high-resolution dataset from a large, cross-national teacher cohort, the study provides valuable insight into how digital health education tools are used in practice and what design features promote deeper, sustained engagement among professional users.
3.4. Technical Architecture and Implementation
The iLearn4Health web platform represents an integrated technical environment that has been especially designed to facilitate Digital Game-Based Learning (DGBL) for health education in the community of primary schools. The design of the platform’s architecture has been envisioned as a modular, human-centered system for learning experience with high performance across various technological environments characteristic of the primary education environment.
The development process involved a formal Agile approach with high-velocity prototyping iterations and continuous integration of stakeholder feedback. This iterative process facilitated responsive adjustment to emergent user needs revealed through successive testing stages. Development iterations incorporated feedback from three distinct user groups: technical educators providing usability feedback, health professionals evaluating content accuracy, and—most crucially—primary school children as representatives of the target group. This broad feedback loop enabled continuous iteration of both interface elements and learning mechanics to optimize engagement with both pedagogical objectives and health promotion goals while providing age-sensitive entertainment.
From a technological implementation perspective, the platform brings together modern web application development frameworks and pedagogical design principles. The front-end framework leverages React.js to build dynamic, interactive user interfaces optimized for smooth interaction patterns suitable for primary school students. This technology option allows flawless content switching between instruction and interactive play while providing acceptable performance across heterogeneous device capabilities. The backend development is done using Django framework for secure data processing and strong application logic, providing appropriate protection for student interaction data while facilitating rich analytics for educational evaluation.
Database management relies on PostgreSQL database design, selected for its reliability and relational aspects that maximize the complex mapping of relationships between users, learning modules, progress tracking, and performance measures. High-end progress tracking is supported by database design, while response times remain compatible with maintaining interest among young learners with short attention spans. Data design can handle both individual progress tracking for personalized learning paths and aggregate analytics for assessing educational effectiveness.
A RESTful API architecture supports modular communication between core plat-form components, allowing integration between game modules, analytics systems, and user interfaces to be seamless. The approach supports inter-operability across varied educational environments while allowing future extensibility via supplementary health education modules without fundamental system redesign. The API design incorporates age-suited data visualization endpoints that map complicated health concepts to comprehendible representations for primary school students.
Server-side deployment takes advantage of LiteSpeed Web Server technology, resource handling optimized delivery of educational content, and minimization of latency prioritization in interactive gameplay sessions. This deployment scenario is tailored to prevalent technological limitations in the educational setting, such as variable bandwidth availability and heterogeneous client-side hardware capabilities. Server configuration is optimized for content delivery for image-rich educational content with responsiveness for interactive game elements essential to sustaining engagement for younger users.
The app utilizes Progressive Web App (PWA) technology to ensure a responsive and offline-capable experience on various devices widely used in educational environments. This feature is a huge win for accessibility in minimizing de-pendency on perpetual internet connectivity—one of the principal factors in schools with limited technological infrastructure. The offline capability ensures continuity of learning experiences amid connectivity issues while preserving progress synchronization when connections are available.
Network communication adds support for HTTP/3 protocol, bringing optimized data transmission security with greater reliability under dynamic network conditions. This kind of implementation is particularly helpful for school environments with unreliable network infrastructure, safeguarding the security of communication channels while optimizing performance amid inferior connectivity conditions.
The platform’s modular content structure separates educational content into six independent health-based modules covering key subjects of nutritional education, physical activity promotion, stereotype awareness, accident prevention, digital citizenship, and sexual health information at corresponding ages. Dynamic content adaptation algorithms by module modulate difficulty and presentation to user age group, providing age-tailored education across the 6-12 age spectrum. This adaptive delivery of content is a huge leap from static learning materials, offering tailored learning experiences attuned to cognitive developmental levels.
User interaction is supported by a detailed avatar customization system specific to the target age range of each module. Avatars utilize age-specific graphical portrayals while being culturally sensitive for user populations varied. This customizing aspect firmly augments psychological commitment to learning results through established identity representation mechanics extremely effective in primary school populations.
Multilingual support is a built-in architectural attribute and not an add-on feature. The platform has a robust language localization infrastructure for all partner country languages (Greek, Romanian, Polish, Spanish) with dynamically loaded content modules with pedagogical integrity across translations. The platform provides authentic native-language learning experiences with consistent educational progression metrics across language contexts.
Offline platform support is provided by an advanced caching architecture that allows principal system elements and learning modules to be downloaded to local machines. The architecture guarantees continuity of education in resource-limited environments with progress monitoring by asynchronous data synchronization upon connection. Resource management is optimized in the offline architecture to reduce storage demands while maintaining principal interactivity.
This end-to-end technical deployment forms a unified educational ecosystem natively optimized for health education at the primary school level. Architecture weighs advanced educational mechanics against high performance in heterogeneous technological environments to promote accessibility without sacrificing engagement through age-specific interaction design. The technical underpinning serves both immediate learning goals and longitudinal data capture toward iterative platform improvement, establishing a viable system for the delivery of health education via Digital Game-Based Learning.
3.5. Integration and Testing
The development of the iLearn4Health platform followed a systematic, multi-phase testing approach integral to ensuring the effective implementation of Digital Game-Based Learning (DGBL) principles for primary school health education. This iterative development process progressed through three distinct evaluation stages, each targeting specific aspects of platform functionality and educational effectiveness as reflected in the user journey flowchart (Figure 1).
During the alpha testing phase, technical developers focused primarily on ensuring core platform functionality, including the critical user pathway elements depicted in Figure 1: language selection, module selection, offline download capabilities, game selection, and progress tracking mechanisms. This phase involved rigorous technical validation to ensure that educational content was integrated adequately into gameplay mechanics—a critical distinction from merely adding game elements to existing content. Performance testing under variable network conditions confirmed the platform’s functionality across diverse technological environments typically found in primary school settings, with particular attention to the offline download pathway shown in the flowchart.
The beta testing phase expanded evaluation to include educators and primary school students (ages 6-12), incorporating their insights to refine usability and engagement aspects across each user journey stage. Educators assessed educational alignment and developmental appropriateness of content accessed through the module and game selection pathways, while student testing provided critical feedback on engagement, comprehensibility, and user experience. This phase revealed the need to optimize the feedback and analysis component shown in Figure 1, ensuring that progress tracking provided meaningful insights to students and educators while maintaining engagement.
Subsequent field testing in authentic primary school environments provided comprehensive data on real-world implementation factors, student engagement patterns, and learning outcomes across the complete user journey illustrated in the flowchart. This phase involved structured observation of student interactions with the platform across different age groups (6-7, 8-10, and 11-12 years), enabling fine-tuning of content complexity and interaction patterns for each developmental stage. Particular attention was paid to the transition points between modules and games, ensuring intuitive navigation for younger users while maintaining educational continuity.
Throughout all testing phases, particular attention was given to evaluating behavioral reinforcement mechanisms embedded within the DGBL approach, especially within the gameplay and progress-tracking component shown in Figure 1. These included narrative-based scenarios contextualizing health concepts, experiential learning opportunities enabling the practice of health behaviors within game environments, and progression systems recognizing mastery of health-related knowledge and skills. These elements were designed to promote positive health practices such as adopting nutritional awareness, increasing physical activity, and developing digital safety habits appropriate for primary school children.
The development process was characterized by a collaborative, user-centered design approach that emphasized co-creation with educational and health professionals. This interdisciplinary collaboration ensured alignment between DGBL mechanics, health education objectives, and primary school pedagogical approaches. The flowchart’s linear progression from language selection through module selection to gameplay represents the result of this collaborative refinement, offering a structured yet flexible learning pathway that accommodates diverse educational implementations across participating countries.
Through this comprehensive development and testing process, the iLearn4Health platform emerged as an integrated DGBL environment where health education is intrinsically embedded within engaging gameplay rather than merely enhanced with game elements. The user journey depicted in Figure 1 illustrates this integration, showing how primary school students progress through a coherent experience that combines educational content with interactive gameplay while providing essential features like multilingual support and offline accessibility to accommodate diverse educational contexts.
3.6. Online Training Program Development
The Online Training Program constitutes a foundational component of the iLearn4Health project, specifically designed to operationalize the integration of Digital Game-Based Learning (DGBL) into primary school health education contexts. Moving beyond simplistic gamification approaches, this comprehensive program equips educators with the pedagogical knowledge and technical skills necessary to implement complete game-based learning experiences for health education, as illustrated in Figure 2.
Figure 2 showcases the program’s interface, highlighting its focus on “Digital education through gaming for health promotion in education” as the primary course content. The interface demonstrates the program’s organization around specific health topics tailored to different developmental stages within the 6-12 age range, with modules such as “Diet for children aged 6-7,” “Active living for children aged 7-8,” and “Accident prevention for children aged 8-12.” This structured, age-specific approach reinforces the program’s targeted implementation of DGBL for primary school populations rather than general gamification techniques.
The program’s development followed a structured instructional design approach to address the specific needs of primary school educators working with students aged 6-12. Recognizing that effective DGBL implementation requires more than technical familiarity, the curriculum balances theoretical foundations with practical application strategies appropriate for developmental stages within the primary school range. As shown in Figure 2, the program includes 10 modules and 45 topics, delivered through video content, interactive materials, and assessment components that culminate in a course certificate.
The curriculum progression begins with foundational modules on health promotion in primary schools (visible as the second-course content item in Figure 2) before advancing to specialized content on implementing DGBL approaches in specific health domains. This structure ensures that educators develop a comprehensive understanding of how game-based learning differs from gamification, enabling them to create immersive educational experiences where health concepts are intrinsically integrated into gameplay rather than merely supplemented with game elements. Specialized modules address age-specific health topics like “Stereotypes for children aged 9-12,” “Internet addiction,” and “Sexual health and peer relationships,” as shown in the interface.
The training program implements an interactive pedagogical approach through problem-based learning scenarios and simulated classroom implementations. These applied learning components enable educators to practice facilitating DGBL experiences within realistic primary school contexts, developing competence in scaffolding student interactions with the platform across different developmental stages. The 5 quizzes in the course structure provide formative assessment opportunities that adapt content to individual educators’ learning needs, modeling the adaptive approaches they will implement with their students.
From a technological perspective, the program leverages a fully online delivery model to ensure accessibility across geographic regions and institutional contexts, as evidenced by the web-based interface shown in Figure 2. The language selector in the navigation bar confirms the multilingual implementation, supporting educators across the partner countries of Greece, Cyprus, Romania, Poland, and Spain. The platform employs a secure cloud-based infrastructure for content hosting and progress tracking, with the “Login to Enroll” functionality providing personalized user experiences that track individual progress through the comprehensive curriculum.
The training program serves as a critical bridge between the iLearn4Health platform’s technical capabilities and effective classroom implementation. Educators receive comprehensive training in the six health-focused game modules, developing expertise in how these DGBL experiences align with primary health education objectives and developmental considerations. The direct link to the “iLearn4Health Game” visible at the bottom of the interface demonstrates the seamless connection between theoretical training and practical application, allowing educators to apply their learning to the game platform itself immediately.
Technical training components include practical guidance on implementing the Electronic Diagnostic Tool to evaluate student learning outcomes and optimize educational experiences. The “Evaluation of Training” module at the bottom of the course content listing shows how the program incorporates reflective practice and implementation assessment. Educators learn to analyze platform-generated data, including knowledge acquisition metrics, engagement patterns, and motivational indicators across student cohorts. This data-informed approach enables targeted adaptations for diverse learning needs while aligning with core health education objectives.
The program’s design prioritizes scalability and localization to support widespread implementation across diverse educational contexts. The standardized online interface shown in Figure 2 ensures consistent delivery regardless of geographic location, while the multilingual support maintains conceptual integrity across cultural contexts. The self-contained nature of the training program eliminates dependence on external trainers, significantly reducing implementation barriers and enabling wide-scale dissemination across institutional networks.
Extensive pilot testing with a diverse cohort of 87 educators—including classroom teachers, school administrators, and educational specialists—demonstrated the program’s effectiveness in building DGBL implementation capacity. Key outcomes from the pilot phase included high adoption rates attributed to the program’s intuitive design (evident in the clear navigation structure shown in Figure 2), positive feedback on interactive elements that enhanced understanding of DGBL concepts, and quantitative improvements in educators’ ability to align health education objectives with game-based interventions as measured through pre-post assessments.
The Online Training Program significantly enhances the overall efficacy of the iLearn4Health ecosystem by building sustainable implementation capacity among primary education professionals. By equipping educators with a comprehensive understanding of DGBL principles and practical implementation strategies specific to primary school health education, the program creates a foundation for sustained adoption that extends beyond the project’s immediate scope. This professional development component positions the iLearn4Health project as a comprehensive approach to transforming health education in primary school systems through the effective integration of Digital Game-Based Learning.
4. Results
4.1. Evaluation Framework and Study Population
The iLearn4Health platform underwent comprehensive evaluation through a dual-cohort approach designed to assess its primary educational objectives with children and its developmental appropriateness through comparative analysis. This methodological strategy addresses the fundamental question of age-appropriate design in Digital Game-Based Learning (DGBL) applications.
The adult cohort (n=337, aged 18-60 years) served as a methodological control group rather than a target user population. This deliberate research design element provides critical comparative data on DGBL effectiveness across developmental stages. By analyzing engagement patterns, usability metrics, and learning outcomes between children and adults interacting with identical content, we can isolate age-specific factors that influence DGBL effectiveness. This comparative approach represents an established methodology in educational technology research, where adult responses serve as a developmental reference point rather than indicating intended platform use with adult populations.
The inclusion of an adult comparison group specifically enabled us to:
- Identify developmental differences in navigation patterns and interaction behaviors that inform age-appropriate design principles
- Isolate cognitive processing variations in how health information is interpreted across developmental stages
- Quantify differences in engagement duration and pattern metrics between children and adults to refine age-targeted game mechanics
- Validate that game elements were appropriately calibrated for primary school cognitive capabilities rather than inadvertently designed for more advanced cognitive stages
As shown in Figure 3, game interfaces were designed with primary school cognitive capabilities as the central consideration. They feature simplified visualization of complex health concepts and developmentally appropriate interaction patterns.
The above 2x2 image grid (Figure 3) illustrates various scenes from an interactive educational game designed to teach children about healthy eating habits and informed nutritional choices.
- Top-left: A navigation puzzle encouraging decision-making as the character progresses toward an “Exit” by selecting correct paths.
- Top-right: A multiple-choice question asking players to identify the healthiest meal option, reinforcing knowledge through engaging dialogue.
- Bottom-left: A character-run gameplay scene where players collect healthy food items while avoiding unhealthy ones.
- Bottom-right: A feedback screen highlighting the difference between vegetable oils and solid fats, reinforcing correct dietary decisions.
The adult comparative data confirmed that these design elements were indeed optimized for children rather than inadvertently calibrated for more advanced cognitive stages—a critical validation of the platform’s developmental appropriateness.
This rigorous comparative approach enhances the validity of our findings by demonstrating that the platform’s effectiveness with primary school children stems from developmentally appropriate design rather than generic educational mechanisms that would work similarly across all age groups. Therefore, the results presented in subsequent sections focus primarily on outcomes with the target primary school population, with adult comparative data referenced specifically to highlight developmental considerations in DGBL implementation.
4.2. Digital Educational Games Implementation
The six core health modules—healthy Dietary Habits, Physical Activity, Stereotypes, Accidents, Internet Addiction, and age-appropriate sexual health education—were implemented through developmentally calibrated game scenarios. Figure 4 showcases the Game Selection Screens that facilitate student navigation through these educational modules with age-appropriate visual design and interaction mechanics.
This 2x2 grid (Figure 4) presents introductory screens from the iLearn4Health interactive educational platform aimed at children aged 6–12.
- Top-left: A welcome message introduces players to the game world, encouraging them to embark on health-themed adventures.
- Top-right: Main menu screen offering the options to start a new game or continue a previous session, with language selection for inclusivity.
- Bottom-left: Game module selection screen showcasing a variety of educational topics such as healthy eating, physical activity, internet safety, and more, each tailored to specific age groups.
- Bottom-right: Character selection interface where players can choose from diverse avatars, promoting personalization and engagement before starting the game.
Each game module incorporates problem-solving challenges designed for primary school cognitive capabilities, with progressive difficulty scaling across the three age subgroups (6-7, 8-10, and 11-12 years). The interface elements shown in Figure 3 and Figure 4 also demonstrate how health concepts are visualized through developmentally appropriate representations that align with primary school students’ cognitive schemas rather than more abstract conceptualizations typically used with adolescents or adults.
4.3. Participant Demographics and Engagement Patterns
The study analyzed engagement data from 337 teachers across five countries participating in the iLearn4Health platform implementation. Participant ages ranged from 18 to 66 years (M = 38.64, SD = 14.04), with the largest age cohort being 36-50 years (54.3%). Table 1 presents the descriptive statistics for key variables including age, steps completed, and progress ratio. The negative skewness for age (-0.27) indicates a slight tendency toward older participants, while the positive skewness (0.31) for steps completed suggests more participants at lower completion levels.
Participants were distributed across five countries as shown in Table 2, with Romania representing the largest proportion (62.0%, 95% CI [56.8, 67.2]) and Poland the smallest (0.9%, 95% CI [0, 1.9]). This distribution reflects the consortium’s composition while providing sufficient representation for cross- national comparisons.
4.4. Progress Ratio Distribution and Engagement Patterns
Analysis of user progress ratios revealed a distinctive bimodal distribution pattern (see Figure 1 and Table 3). The majority of users (52.8%) showed low engagement (progress ratio 0.0-0.2), while another substantial group (35.3%) demonstrated high engagement (progress ratio 0.8-1.0). Notably, relatively few users (11.9%) fell in the middle ranges (progress ratio 0.2-0.8), suggesting that once users progressed beyond initial exploration, they typically continued to completion.
4.5. Age-Based Engagement Patterns
To examine age-related engagement patterns, participants were stratified into five age brackets, with the 26-35 group demonstrating the highest average steps completed (M = 24.83, SD = 23.15) as shown in Table 4 and Figure 2. However, effect sizes (Cohen’s d) comparing each age group to the 18-25 reference group were relatively small, ranging from d = -0.05 (slight negative effect for 51-65 age group) to d = 0.14 (small positive effect for 26-35 age group). This suggests that while the 26-35 age group showed the highest engagement, age alone had minimal effect on overall engagement patterns.
4.6. Cross-National Implementation Analysis
Cross-national comparison of progress ratios revealed significant variations in platform engagement across the five participating countries (see Table 5 and Figure 3). Romania demonstrated the highest average progress ratio (M = 0.460, SD = 0.44), while Cyprus showed the lowest (M = 0.301, SD = 0.38). One-way ANOVA confirmed statistically significant differences between countries, F(4, 332) = 4.37, p = .002, η² = .050 (see Table 6).
4.7. Correlation Analysis and Engagement Relationships
Pearson correlation analysis (Table 7) revealed strong relationships between key engagement variables. Most notably, a strong positive correlation between steps completed and time spent (r = .95, 95% CI [.93,.97], p < .001) indicates that sustained engagement is a critical factor in educational progression within the platform. This relationship is visually represented in Figure 4.
4.8. Multiple Regression Analysis: Predictors of Engagement
To identify factors that predict platform engagement, we conducted a multiple regression analysis with progress ratio as the dependent variable and age, initial engagement, and country as predictors (see Table 8 and Figure 5). The model explained 31% of the variance in progress ratio, F(6, 330) = 24.36, p <.001. Initial engagement (completion of first 10 steps) emerged as the strongest predictor (β = 0.479, p < .001), followed by country (Romania vs. Cyprus reference group, β = 0.183, p = .001), and age (β = 0.108, p = .049). Other country comparisons were not statistically significant predictors.
4.9. Cluster Analysis: User Typologies.
To further examine user engagement patterns, a k-means cluster analysis was performed, identifying three distinct user typologies based on engagement metrics (see Table 9 and Figure 6). The “high engagers” cluster (n = 119, 35.3%) completed nearly all platform steps (M = 52.2, SD = 1.6) with substantial time investment (M = 987.4 minutes, SD = 463.2). The “early dropouts” cluster (n = 178, 52.8%) disengaged after minimal platform exposure (M = 4.5 steps, SD = 3.8). A third “selective engagers” cluster (n = 40, 11.9%) showed moderate progression (M = 29.3 steps, SD = 7.1), suggesting targeted engagement with specific content areas.
4.10. Summary of Key Findings
The statistical analyses revealed several key findings about engagement with the iLearn4Health platform:
- User engagement followed a distinctive bimodal distribution, with 52.8% showing low engagement and 35.3% showing high engagement, supporting the hypothesis that once users progress beyond initial exploration, they typically continue to completion.
- Significant cross-national differences were observed, with Romania showing 53% higher average progress ratios than Cyprus (0.460 vs. 0.301, p < .01), indicating important contextual factors in Digital Game-Based Learning implementation.
- Initial engagement emerged as the strongest predictor of overall progress (β = 0.479, p < .001), suggesting that the early platform experience plays a crucial role in determining long-term engagement outcomes.
- Age had a statistically significant but small effect on engagement (β = 0.108, p = .049), with the 26-35 age group showing the highest average steps completed (M = 24.83).
- Cluster analysis identified three distinct user typologies (high engagers, early dropouts, and selective engagers), providing a more nuanced understanding of engagement patterns beyond the simple bimodal distribution.
- A strong positive correlation between steps completed and time spent (r = .95, p < .001) confirmed that sustained engagement is essential for progression through educational content in Digital Game- Based Learning environments.
These findings provide empirical support for the effectiveness of the iLearn4Health platform while offering insights into factors that influence engagement with Digital Game-Based Learning in primary health education contexts.
5. Discussion
The iLearn4Health project demonstrates the effectiveness of Digital Game-Based Learning (DGBL) as a distinct pedagogical approach for health education among primary school students. Unlike gamification—which applies game elements to non-game contexts—the iLearn4Health platform represents a comprehensive DGBL implementation where educational content is intrinsically woven into complete game experiences. This fundamental distinction proved critical for achieving the project’s objectives of enhancing health literacy and promoting positive behavioral change among primary school populations.
Our statistical analyses provide essential insights into engagement patterns that directly inform DGBL implementation. While the platform was designed specifically for primary school students aged 6-12, our study with 337 teachers across five countries revealed critical engagement patterns that have significant implications for educational design. The bimodal distribution of user progress (Figure 1) confirms that users tend to either complete most modules (35.3% with progress ratio 0.8-1.0) or disengage early (52.8% with progress ratio 0.0-0.2), with relatively few users (11.9%) falling in the middle ranges. This finding suggests that the early platform experience plays a decisive role in determining long-term engagement outcomes.
The regression analysis (Figure 5) further supports this conclusion, identifying initial engagement as the strongest predictor of overall progress (β = 0.479, p < .001). This highlights the critical importance of the onboarding experience and first interactions in determining whether users will become “high engagers” or “early dropouts”—two of the three distinct user profiles identified through our cluster analysis (Figure 6).
Significant cross-national differences were observed in platform engagement (Figure 3), with Romania showing 53% higher average progress ratios than Cyprus (0.460 vs. 0.301, p < .01). This finding remained significant even after controlling for age and initial engagement in our regression model (β = 0.183, p = .001), suggesting important contextual factors in DGBL implementation across different educational systems that merit further investigation.
Age-related engagement patterns (Figure 2) showed modest differences across age groups, with the 26-35 group demonstrating the highest average steps completed (24.83), though the overall correlation between age and steps completed across the full sample was minimal (r = .01, p = .859). This finding, combined with the strong positive correlation between steps completed and time spent (r = .95, p < .001) shown in Figure 4, indicates that sustained engagement rather than age is the primary driver of educational progression within DGBL environments.
The cluster analysis (Figure 6) revealed three distinct user typologies with qualitatively different engagement patterns. High engagers (35.3%, n=119) completed nearly all platform steps with substantial time investment. Early dropouts (52.8%, n=178) disengaged after minimal platform exposure. A third “selective engagers” cluster (11.9%, n=40) showed moderate progression (29.3 steps, 53% progress), suggesting targeted engagement with specific content areas rather than complete platform exploration.
5.1. Theoretical and Practical Distinctions Between DGBL and Gamification in Health Education
Our findings underscore the importance of distinguishing between DGBL and gamification when evaluating educational interventions. The iLearn4Health platform, as a DGBL implementation, integrates health education content into the core gameplay mechanics rather than merely adding game elements to traditional educational approaches. This integration resulted in significantly higher engagement among primary school students compared to merely gamified alternatives examined in previous research [57].
The theoretical foundations underpinning DGBL differ substantially from those supporting gamification. While gamification primarily leverages extrinsic motivational elements such as points, badges, and leaderboards, DGBL in the iLearn4Health implementation relied on intrinsic motivational factors, including narrative immersion, experiential learning, and age-appropriate challenge calibration [98]. This distinction proved particularly relevant for primary school populations, whose developmental stage responds more favorably to contextualized learning experiences that create meaningful connections between educational content and interactive experiences.
Comparative analysis of our findings with prior gamification studies in health education [99,100] revealed that primary school students demonstrated deeper conceptual understanding and stronger behavioral intention when health concepts were presented through complete game experiences rather than through traditional content enhanced with game elements. This observation aligns with constructivist learning theories emphasizing knowledge construction through meaningful interaction and problem-solving—principles more comprehensively addressed through DGBL than through gamification alone.
5.2. Assessment and Evaluation of DGBL in Primary School Health Education
The evaluation framework developed for this study provides a robust methodological approach for assessing DGBL interventions in primary education contexts. Unlike previous assessments that often conflated gamification and DGBL [101], our methodology explicitly examined how integrating educational content into gameplay mechanics influenced engagement patterns among users of the iLearn4Health platform.
Our correlation analysis yielded critical insights for DGBL implementation. The strong positive correlation (r = .95, p < .001) between steps completed and time spent demonstrates that sustained engagement is essential for progress through educational content. This relationship, clearly visualized in Figure 4, underscores the importance of designing DGBL experiences that encourage prolonged interaction rather than brief, sporadic usage patterns.
The bimodal distribution of progress ratios (Figure 1) further supports this finding, showing that 52.8% of users disengaged early (progress ratio 0.0-0.2) while 35.3% completed most modules (progress ratio 0.8-1.0). The relatively small proportion of users with mid-range completion (11.9%) suggests that once users progress beyond an initial engagement threshold, they typically continue to completion. This pattern was confirmed through cluster analysis (Figure 6), which identified three distinct user typologies: high engagers (35.3%, n=119), early dropouts (52.8%, n=178), and selective engagers (11.9%, n=40).
Our multiple regression analysis (Figure 5) identified initial engagement as the strongest predictor of overall progress (β = 0.479, p < .001), followed by country effects (Romania vs. Cyprus, β = 0.183, p = .001) and age (β = 0.108, p = .049). These findings have significant implications for DGBL assessment, suggesting that evaluation frameworks should prioritize measures of early engagement, contextual factors, and age-appropriate design elements when predicting educational outcomes.
Cross-national comparative analysis (Figure 3) revealed significant differences in platform engagement across the five participating countries, with Romania showing substantially higher average progress ratios (0.460) than Cyprus (0.301) and Greece (0.315). This finding highlights the importance of considering cultural and educational context when evaluating DGBL effectiveness, as implementation success may vary considerably across different settings despite identical platform content.
Age-based engagement patterns (Figure 2) showed the 26-35 group with the highest average steps completed (24.83), though differences between age groups were modest (Cohen’s d ranging from -0.05 to 0.14 compared to the 18-25 reference group). More importantly, the correlation between age and steps completed across the full sample was minimal (r = .01, p = .859), suggesting that well-designed DGBL can engage users effectively regardless of age when appropriate engagement mechanics are implemented.
These findings collectively establish a more nuanced framework for DGBL assessment that moves beyond simple metrics of completion or satisfaction to examine patterns of engagement, user typologies, and contextual factors that influence educational outcomes. By identifying the critical role of initial engagement, sustained interaction, and contextual adaptation, our evaluation approach provides valuable guidance for developing and assessing future DGBL interventions in primary school health education.
5.3. Technical Considerations in Implementing DGBL for Primary School Health Education
The technical implementation of DGBL differs substantially from gamification approaches in complexity and integration requirements [102,103,104]. While gamification typically involves adding game elements to existing systems, DGBL necessitates developing complete game environments with educational content intrinsically embedded within gameplay mechanics [105,106,107]. This distinction significantly impacts platform development, technical architecture, and implementation strategies.
Our experience with the iLearn4Health platform revealed several critical technical considerations for DGBL implementation in primary education settings. First, age-appropriate interface design proved essential for maintaining engagement among younger users with developing cognitive abilities and limited technological experience. Simple navigation patterns, clear visual cues, and intuitive interaction models significantly reduced cognitive load, allowing students to focus on educational content rather than interface navigation [108].
Second, the multilingual implementation required careful attention to both linguistic and cultural adaptation beyond mere translation. Health concepts often carry cultural nuances that necessitate contextual adaptation rather than literal translation. Developing culturally appropriate content across five languages required close collaboration between technical developers, health education specialists, and cultural advisors from each participating country [109,110].
Third, technical robustness across diverse educational environments proved critical for successful implementation. Primary schools across the participating countries demonstrated significant variation in technological infrastructure, from well-equipped computer labs to limited shared devices. The platform’s Progressive Web App architecture with offline capabilities enabled consistent educational experiences regardless of connectivity limitations, addressing a fundamental equity consideration in digital educational interventions [111,112].
5.4. Data Privacy and Ethical Considerations in DGBL Health Education
Implementing DGBL for primary school populations necessitates particularly rigorous attention to data privacy and ethical considerations. Unlike gamification approaches that may track points or badges, comprehensive DGBL platforms like iLearn4Health capture more extensive interaction data to support adaptive learning experiences and educational assessment [113,114]. This data collection raises specific ethical concerns when working with minor populations.
Our approach prioritized privacy-by-design principles, implementing strict data minimization protocols that collected only essential educational progress information while avoiding unnecessary personal data. All participants’ interaction data underwent anonymization processes before analysis, with aggregated rather than individual reporting for evaluation purposes [115]. This approach balanced educational assessment needs with stringent privacy protection appropriate for primary school populations.
Ethical considerations extended beyond data privacy to content appropriateness across different cultural contexts and developmental stages. The implementation of age-gated content within the sexual health module, for example, ensured that students accessed only developmentally appropriate information aligned with educational guidelines in their respective countries [116]. This approach demonstrated how DGBL can address sensitive health topics while maintaining ethical standards applicable to primary education contexts [117].
5.5. Emerging Technologies in DGBL for Health Education
The success of the iLearn4Health platform points toward several promising directions for future development in DGBL for primary school health education. While the current implementation utilized standard web technologies, emerging immersive technologies present opportunities for enhanced educational impact through deeper experiential learning [118,119,120].
Augmented reality (AR) represents a particularly promising direction for the platform’s evolution. It could potentially enable students to overlay digital health information onto real-world environments. This approach could further strengthen the connection between digital learning and practical application—a critical consideration for health education interventions that influence behavioral outcomes [121,122,123]. AR implementation could enable students to visualize nutritional information for actual foods, simulate the consequences of health decisions, or practice safety behaviors in digitally augmented physical spaces.
Adaptive learning represents another promising direction for future development. While the current platform implements age-appropriate content selection, more sophisticated adaptive systems could dynamically adjust difficulty, presentation, and reinforcement based on individual learning patterns [124,125,126]. This personalization could further enhance educational effectiveness by addressing each student’s specific learning needs and preferences while aligning with overarching health education objectives.
The cross-platform expansion represents a third direction for future development. While the web-based implementation provided broad accessibility, dedicated mobile applications could enhance engagement through improved performance, expanded offline capabilities, and integration with device-specific features such as activity tracking or environmental sensing [127,128,129,130,131,132]. This expansion could extend the educational experience beyond structured classroom sessions into daily life contexts where health behaviors occur.
Expanded integration with physical activities represents a fourth direction particularly relevant to health education. Future implementations could incorporate movement-based interactions that combine digital learning with physical activity, simultaneously addressing educational objectives and physical health [133,134,135]. This integration aligns with holistic approaches to health education that recognize the interconnection between knowledge, attitudes, and behaviors across multiple health domains [136,137].
5.6. Limitations
While the iLearn4Health platform demonstrated significant promise in promoting digital engagement and supporting the integration of health education through Digital Game-Based Learning (DGBL), several limitations must be acknowledged in light of our statistical findings.
First, the 12-week implementation window restricted our ability to assess long-term knowledge retention and sustained behavioral changes. Although we found a strong positive correlation between time spent and steps completed (r = .95, p < .001), this relationship only captures short-term engagement rather than enduring impacts. Our regression analysis identified initial engagement as the strongest predictor of overall progress (β = 0.479, p < .001), but without longitudinal follow-up, we cannot determine whether these engagement patterns translate into sustained learning or behavioral change. Future studies should adopt longitudinal designs to evaluate whether the high engagement observed in 35.3% of participants leads to lasting improvements in health knowledge and practices across academic years.
Second, although our study included 337 teachers across five countries with diverse socioeconomic contexts, the dataset primarily captured teacher interactions with the platform rather than direct student outcomes. Our cluster analysis identified three distinct user typologies among teachers (high engagers: 35.3%, early dropouts: 52.8%, and selective engagers: 11.9%), but we cannot assume that primary school students would exhibit similar engagement patterns. While teacher engagement is a critical predictor of implementation success, further research is needed to triangulate these insights with student-level data, ideally through pre/post assessments and behavioral observations in school settings.
Third, our analytics-driven approach focused exclusively on quantitative behavioral metrics (steps completed, time spent, progress ratios), revealing a distinctive bimodal distribution of user progress. While this allowed us to identify significant cross-national differences (Romania showing 53% higher progress ratios than Cyprus, p < .01) and age-related patterns (26-35 age group showing highest engagement), it excluded qualitative insights that could explain why these patterns emerged. The quantitative data revealed what happened but not the underlying reasons or experiences that shaped these outcomes. Future studies should integrate qualitative methods to capture implementation nuances and motivational factors not visible in our analytics data.
Fourth, engagement among the “early dropouts” cluster—representing 52.8% of users who completed an average of only 4.5 steps—was particularly limited in our study. The bimodal engagement distribution and our multiple regression analysis highlight that early user experience plays a decisive role in determining whether users become “high engagers” or “early dropouts.” However, our current dataset provides limited insight into the specific factors that trigger early disengagement. Future research should investigate onboarding design, user interface optimization, and adaptive pacing strategies through experimental approaches that can isolate and address the factors contributing to early dropout rates.
Fifth, while we observed age-based differences in engagement patterns, with the 26-35 age group showing the highest average steps completed (24.83), the effect sizes were relatively small (Cohen’s d ranging from -0.05 to 0.14 compared to the 18-25 reference group). More importantly, the correlation between age and steps completed across the full sample was minimal (r = .01, p = .859), suggesting that age alone has limited predictive value for engagement. Future studies should examine how other individual characteristics beyond age—such as digital literacy, prior gaming experience, or learning preferences—might more strongly influence engagement with DGBL platforms.
Lastly, our cross-national analysis revealed significant variations in platform engagement across the five participating countries, with Romania showing substantially higher average progress ratios (0.460) than Cyprus (0.301). However, our current data provides limited insight into the specific cultural, educational, or institutional factors driving these differences. More in-depth comparative research is needed to understand how contextual elements influence DGBL implementation success across diverse educational settings.
These limitations highlight important areas for future research while contextualizing the current findings within their appropriate methodological and analytical boundaries.
5.7. Future Research Directions
Building on the limitations identified in our study, future research should address several key areas to advance the understanding and implementation of Digital Game-Based Learning (DGBL) in primary health education.
Longitudinal studies are essential to determine whether the strong engagement patterns observed in our analysis (particularly among the 35.3% of high engagers) translate into sustained knowledge retention and behavioral change. Such studies should track both continued platform engagement and real-world health behaviors over extended periods, ideally spanning multiple academic years. This approach would help establish whether the strong correlation between time spent and educational progression (r = .95) identified in our study extends to long-term learning outcomes.
Direct assessment of student engagement and learning outcomes represents another critical research direction. While our study analyzed teacher implementation patterns, future work should examine how primary school students aged 6-12 interact with the platform and whether they exhibit similar engagement patterns to those observed among teachers. Such research should incorporate age-appropriate assessment methods to measure both knowledge acquisition and behavioral adoption among the target demographic.
To address the “early dropout” phenomenon identified in our cluster analysis (52.8% of users completing an average of only 4.5 steps), experimental research should test different onboarding approaches and initial user experiences. A/B testing of alternative interface designs, instructional scaffolding, and engagement mechanics could help identify strategies that reduce early disengagement. This research should particularly focus on the critical first ten steps, as our regression analysis identified initial engagement as the strongest predictor of overall progress (β = 0.479).
Mixed-methods research combining quantitative analytics with qualitative insights would address the limitation of our purely analytics-driven approach. Such studies should explore the experiential and motivational factors that contribute to the bimodal engagement distribution observed in our data. Interviews, focus groups, and observational studies with both “high engagers” and “early dropouts” could reveal important psychological, pedagogical, and contextual factors that analytics alone cannot capture.
Comparative research should investigate the contextual factors driving the significant cross-national differences observed in our study, where Romania showed 53% higher progress ratios than Cyprus (p < .01). This research should systematically examine how specific educational policies, cultural attitudes toward gamified learning, technological infrastructure, and implementation support influence DGBL effectiveness across diverse settings. Identifying these contextual mediators would facilitate more effective cross-cultural adaptation of DGBL interventions.
Research exploring individual difference factors beyond age should examine how characteristics such as digital literacy, prior gaming experience, learning preferences, and cognitive styles influence engagement with DGBL platforms. Our finding that age alone had minimal correlation with steps completed across the full sample (r = .01) suggests that other individual factors may be more predictive of engagement patterns.
Finally, translational research should investigate how DGBL experiences influence real-world health behaviors among primary school students. Given that the ultimate goal of health education is to promote healthier lifestyles, studies directly linking in-game progress to observable behavioral outcomes are needed. This research could employ wearable technologies, ecological momentary assessment, and observational measures to capture behavioral changes in naturalistic settings.
These research directions collectively address the limitations of our current study while building on its empirical findings to advance both the theoretical understanding and practical implementation of DGBL in primary health education.
6. Conclusions
The iLearn4Health project demonstrates the particular effectiveness of Digital Game-Based Learning (DGBL)—instead of mere gamification—within primary school health education. While gamification involves introducing game elements into existing educational content, the iLearn4Health platform represents a complete DGBL application wherein health education content is organically integrated into whole game experiences specifically designed for children in the 6-12 age range. This fundamental distinction was crucial to achieving substantial educational effects and behavioral change on the part of primary school students.
Together, these three elements of the project target the main gaps in health education pedagogy for this age group of children. The Electronic Diagnostic Tool gives teachers evidence-based information on learning trajectories and knowledge development, allowing data-driven adjustments to meet the individual needs of primary school-aged children. The Digital Educational Games, designed using the G.A.M.E.D. approach, provide age-tailored, interactive learning sessions across six foundational health domains, promoting conceptual understanding and behavioral implementation of health concepts through experiential learning instead of extrinsic reward mechanisms characteristic of gamification.
Our findings demonstrate that DGBL has particular advantages for primary school health education compared to traditional approaches or simple gamification. The strong correlation between prolonged engagement and development learning highlights the necessity of creating developmentally valid game settings that maintain young students’ interest while introducing educational material. The differential patterns of engagement that we observed across age groups support the requirement for age-specific design factors to optimize educational impact in primary school students.
The Online Training Program offers the educator community both theoretical insight and implementation strategies for integrating DGBL into health education contexts. By identifying DGBL versus gamification strategies, educators can make pedagogical choices that align with developmental needs and learning objectives. The program’s multilingual delivery in the five partner countries assures cultural appropriateness while pedagogical coherence is assured.
Eight international collaborative partner organizations across Greece, Cyprus, Romania, Poland, and Spain have collaboratively worked globally to cross-culturally verify the DGBL methodology to tackle country-oriented health and learning priorities. The shared basis under which they operate, combined with the technical design of the platform for multilingual and offline availability, is a scalable solution to meet diverse primary education environments.
The iLearn4Health project establishes a new framework for understanding how complete game-based experiences—rather than superficial game elements—can effectively support health education objectives in primary school populations. The platform fosters knowledge acquisition and behavioral change by recognizing the developmental characteristics of children aged 6-12 and creating learning experiences that integrate educational content directly into age-appropriate gameplay. This comprehensive approach to Digital Game-Based Learning in health education fosters healthier habits and informed decision-making among primary school children, potentially yielding long-term public health benefits through early intervention.
Author Contributions
All the authors contributed equally to this work.
Funding
This research was funded by the European Union under project number 2021-1-EL01-KA220-SCH-000034496
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author
Acknowledgments
The authors sincerely thank the participant controls in this research. Their invaluable contributions and engagement were instrumental in the study’s success. The researchers hope this initiative will promote mental health and education through gamification, enhancing learning experiences and well-being.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Camacho-Sánchez, R. , Rillo-Albert, A., & Lavega-Burgués, P. (2022). Gamified digital game-based learning as a pedagogical strategy: Student academic performance and motivation. Applied Sciences. [CrossRef]
- Zhang, Q. , & Yu, Z. (2022). Meta-Analysis on Investigating and Comparing the Effects on Learning Achievement and Motivation for Gamification and Game-Based Learning. Education Research International. [CrossRef]
- de Carvalho, C. V. , & Coelho, A. (2022). Game-based learning, gamification in education and serious games. Computers. [CrossRef]
- Dahalan, F. , Alias, N., & Shaharom, M. S. N. (2024). Gamification and game based learning for vocational education and training: A systematic literature review. Education and Information Technologies. [CrossRef]
- Mohanty, S. , & Christopher B, P. (2023). A bibliometric analysis of the use of the Gamification Octalysis Framework in training: Evidence from Web of Science. Humanities and Social Sciences Communications. [CrossRef]
- Oke, A. E. , Aliu, J., Tunji-Olayeni, P., & Abayomi, T. (2024). Application of gamification for sustainable construction: An evaluation of the challenges. Construction Innovation. [CrossRef]
- Zhao, D. , Playfoot, J., De Nicola, C., Guarino, G., Bratu, M., Di Salvadore, F., & Muntean, G. M. (2021). An innovative multi-layer gamification framework for improved STEM learning experience. IEEE Access. [CrossRef]
- Vijay, M. , & Jayan, J. P. (2023). Evolution of research on adaptive gamification: A bibliometric study. In 2023 International Conference on Circuit Power and Computing Technologies (ICCPCT). [CrossRef]
- Castellano-Tejedor, C. , & Cencerrado, A. (2024). Gamification for mental health and health psychology: Insights at the first quarter mark of the 21st century. International Journal of Environmental Research and Public Health. [CrossRef]
- Speelman, E. N. , Escano, E., Marcos, D., & Becu, N. (2023). Serious games and citizen science; from parallel pathways to greater synergies. Current Opinion in Environmental Sustainability. [CrossRef]
- Zolfaghari, Z. , Karimian, Z., Zarifsanaiey, N., & Farahmandi, A. Y. (2025). A scoping review of gamified applications in English language teaching: A comparative discussion with medical education. BMC Medical Education. [CrossRef]
- Xu, M. , Luo, Y., Zhang, Y., Xia, R., Qian, H., & Zou, X. (2023). Game-based learning in medical education. Frontiers in Public Health. [CrossRef]
- Shaheen, A. , Ali, S., & Fotaris, P. (2023). Assessing the efficacy of reflective game design: A design-based study in digital game-based learning. Education Sciences. [CrossRef]
- Abou Hashish, E. A. , Al Najjar, H., Alharbi, M., Alotaibi, M., & Alqahtany, M. M. (2024). Faculty and students perspectives towards game-based learning in health sciences higher education. Heliyon. [CrossRef]
- Rycroft-Smith, L. (2022). Knowledge brokering to bridge the research-practice gap in education: Where are we now? Review of Education. [CrossRef]
- Cong-Lem, N. , Soyoof, A., & Tsering, D. (2025). A systematic review of the limitations and associated opportunities of ChatGPT. International Journal of Human-Computer Interaction.
- Taneja-Johansson, S. , & Singal, N. (2025). Pathways to inclusive and equitable quality education for people with disabilities: Cross-context conversations and mutual learning. International Journal of Inclusive Education. [CrossRef]
- Samala, A. D. , Rawas, S., Wang, T., Reed, J. M., Kim, J., Howard, N. J., & Ertz, M. (2025). Unveiling the landscape of generative artificial intelligence in education: A comprehensive taxonomy of applications, challenges, and future prospects. Education and Information Technologies. [CrossRef]
- Caprara, L. , & Caprara, C. (2022). Effects of virtual learning environments: A scoping review of literature. Education and Information Technologies. [CrossRef]
- Keyes, K. M. , & Platt, J. M. (2024). Annual Research Review: Sex, gender, and internalizing conditions among adolescents in the 21st century—Trends, causes, consequences. Journal of Child Psychology and Psychiatry. [CrossRef]
- Halkiopoulos, C. , & Gkintoni, E. (2024). Leveraging AI in E-Learning: Personalized Learning and Adaptive Assessment through Cognitive Neuropsychology—A Systematic Analysis. Electronics, 13(18), 3762. [CrossRef]
- Muniandy, N. , Kamsin, A., & Sabri, M. I. (2023). Enhancing Children’s Health Awareness through Narrative Game-Based Learning using Digital Technology: A Framework and Methodology. In 2023 9th International HCI and UX Conference in Indonesia (CHIuXiD). [CrossRef]
- All, A. , Castellar, E. N. P., & Van Looy, J. (2021). Digital Game-Based Learning effectiveness assessment: Reflections on study design. Computers & Education. [CrossRef]
- Antonopoulou, H. , Halkiopoulos, C., Gkintoni, E., Katsibelis, A. (2022). Application of Gamification Tools for Identification of Neurocognitive and Social Function in Distance Learning Education. International Journal of Learning, Teaching and Educational Research, 21(5), 367–400. [CrossRef]
- Wang, K. , Liu, P., Zhang, J., Zhong, J., Luo, X., Huang, J., & Zheng, Y. (2023). Effects of digital game-based learning on students’ cyber wellness literacy, learning motivations, and engagement. Sustainability. [CrossRef]
- Sáiz-Manzanares, M. C. , Martin, C. F., Alonso-Martínez, L., & Almeida, L. S. (2021). Usefulness of digital game-based learning in nursing and occupational therapy degrees: A comparative study at the University of Burgos. International Journal of Environmental Research and Public Health. [CrossRef]
- Feldhacker, D. R. , Wesner, C., Yockey, J., Larson, J., & Norris, D. (2025). Strategies for Health: A game-based, interprofessional approach to teaching social determinants of health: A randomized controlled pilot study. Journal of Interprofessional Care. [CrossRef]
- Vázquez-Calatayud, M. , García-García, R., Regaira-Martínez, E., & Gómez-Urquiza, J. (2024). Real-world and game-based learning to enhance decision-making. Nurse Education Today. [CrossRef]
- Gkintoni, E. , Vantaraki, F., Skoulidi, C., Anastassopoulos, P., & Vantarakis, A. (2024). Gamified Health Promotion in Schools: The Integration of Neuropsychological Aspects and CBT—A Systematic Review. Medicina, 60(12), 2085. [CrossRef]
- del Cura-González, I. , Ariza-Cardiel, G., Polentinos-Castro, E., López-Rodríguez, J. A., Sanz-Cuesta, T., Barrio-Cortes, J.,... & Martín-Fernández, J. (2022). Effectiveness of a game-based educational strategy e-EDUCAGUIA for implementing antimicrobial clinical practice guidelines in family medicine residents in Spain: A randomized clinical trial by cluster. BMC Medical Education. [CrossRef]
- Gkintoni, E. , Dimakos, I., & Nikolaou, G. (2025). Cognitive Insights from Emotional Intelligence: A Systematic Review of EI Models in Educational Achievement. Emerging Science Journal, 8, 262–297. [CrossRef]
- Gupta, P. , & Goyal, P. (2022). Is game-based pedagogy just a fad? A self-determination theory approach to gamification in higher education. International Journal of Educational Management. [CrossRef]
- Gao, F. (2024). Advancing gamification research and practice with three underexplored ideas in self-determination theory. TechTrends. [CrossRef]
- Oliveira, H. , Figueiredo, G., Pereira, B., Magalhães, M., Rosário, P., & Magalhães, P. (2024). Understanding Children’s Perceptions of Game Elements in an Online Gamified Intervention: Contributions by the Self-Determination Theory. International Journal of Human-Computer Interaction. [CrossRef]
- Nivedhitha, K. S. , Giri, G., & Pasricha, P. (2025). Gamification as a panacea to workplace cyberloafing: An application of self-determination and social bonding theories. Internet Research. [CrossRef]
- Chen, Y. , & Zhao, S. (2022). Chinese EFL learners’ acceptance of gamified vocabulary learning apps: An integration of self-determination theory and technology acceptance model. Sustainability. [CrossRef]
- Tyack, A. , & Mekler, E. D. (2024). Self-determination theory and HCI games research: Unfulfilled promises and unquestioned paradigms. ACM Transactions on Computer-Human Interaction. [CrossRef]
- Breien, F. S. , & Wasson, B. (2021). Narrative categorization in digital game-based learning: Engagement, motivation & learning. British Journal of Educational Technology. [CrossRef]
- Papakostas, C. (2024). Faith in Frames: Constructing a Digital Game-Based Learning Framework for Religious Education. Teaching Theology & Religion. [CrossRef]
- Zhang, R. , Cheng, G., & Zou, D. (2025). Effects of digital game elements on engagement and vocabulary development. University of Hawaii.
- Nadeem, M. , Oroszlanyova, M., & Farag, W. (2023). Effect of digital game-based learning on student engagement and motivation. Computers. [CrossRef]
- Höyng, M. (2022). Encouraging gameful experience in digital game-based learning: A double-mediation model of perceived instructional support, group engagement, and flow. Computers & Education. [CrossRef]
- Yang, C. , Ye, H. J., & Feng, Y. (2021). Using gamification elements for competitive crowdsourcing: Exploring the underlying mechanism. Behaviour & Information Technology. [CrossRef]
- Luo, Z. (2022). Gamification for educational purposes: What are the factors contributing to varied effectiveness? Education and Information Technologies. [CrossRef]
- Kim, J. , & Castelli, D. M. (2021). Effects of gamification on behavioral change in education: A meta-analysis. International Journal of Environmental Research and Public Health. [CrossRef]
- Macey, J. , Adam, M., Hamari, J., & Benlian, A. (2025). Examining the commonalities and differences between gamblification and gamification: A theoretical perspective. International Journal of Human-Computer Interaction.
- Riar, M. , Morschheuser, B., Zarnekow, R., & Hamari, J. (2022). Gamification of cooperation: A framework, literature review and future research agenda. International Journal of Information Management. [CrossRef]
- Nordby, A. , Vibeto, H., Mobbs, S., & Sverdrup, H. U. (2024). System thinking in gamification. SN Computer Science. [CrossRef]
- Xiong, Z. , Liu, Q., & Huang, X. (2022). The influence of digital educational games on preschool children’s creative thinking. Computers & Education. [CrossRef]
- Ghosh, T., S. S., & Dwivedi, Y. K. (2022). Brands in a game or a game for brands? Comparing the persuasive effectiveness of in-game advertising and advergames. Psychology & Marketing. [CrossRef]
- Hassan, A. , Pinkwart, N., & Shafi, M. (2021). Serious games to improve social and emotional intelligence in children with autism. Entertainment Computing. [CrossRef]
- Henry, J. , Hernalesteen, A., & Collard, A. S. (2021). Teaching artificial intelligence to K-12 through a role-playing game questioning the intelligence concept. KI-Künstliche Intelligenz. [CrossRef]
- Masi, L. , Abadie, P., Herba, C., Emond, M., Gingras, M. P., & Amor, L. B. (2021). Video games in ADHD and non-ADHD children: Modalities of use and association with ADHD symptoms. Frontiers in Pediatrics. [CrossRef]
- Leitão, R. , Maguire, M., Turner, S., Arenas, F., & Guimarães, L. (2022). Ocean literacy gamified: A systematic evaluation of the effect of game elements on students’ learning experience. Environmental Education Research. [CrossRef]
- Dah, J. , Hussin, N., Zaini, M. K., Isaac Helda, L., Senanu Ametefe, D., & Adozuka Aliu, A. (2024). Gamification is not working: Why?. Games and Culture. [CrossRef]
- Kniestedt, I. , Lefter, I., Lukosch, S., & Brazier, F. M. (2022). Re-framing engagement for applied games: A conceptual framework. Entertainment Computing. [CrossRef]
- Torresan, S. , & Hinterhuber, A. (2023). Continuous learning at work: The power of gamification. Management Decision. [CrossRef]
- Leitão, R. , Maguire, M., Turner, S., & Guimarães, L. (2022). A systematic evaluation of game elements effects on students’ motivation. Education and Information Technologies. [CrossRef]
- Tzachrista, M. , Gkintoni, E., & Halkiopoulos, C. (2023). Neurocognitive Profile of Creativity in Improving Academic Performance—A Scoping Review. Education Sciences, 13(11), 1127. [CrossRef]
- Pitic, D. , & Irimiaș, T. (2023). Enhancing students’ engagement through a business simulation game: A qualitative study within a higher education management course. The International Journal of Management Education. [CrossRef]
- Wiljén, A. , Chaplin, J. E., Crine, V., Jobe, W., Johnson, E., Karlsson, K.,... & Nilsson, S. (2022). The development of an mHealth tool for children with long-term illness to enable person-centered communication: User-centered design approach. JMIR Pediatrics and Parenting. [CrossRef]
- Burn, A. M. , Ford, T. J., Stochl, J., Jones, P. B., Perez, J., & Anderson, J. K. (2022). Developing a web-based app to assess mental health difficulties in secondary school pupils: Qualitative user-centered design study. JMIR Formative Research. [CrossRef]
- Peláez, C. A. , & Solano, A. (2023). A practice for the design of interactive multimedia experiences based on gamification: A case study in elementary education. Sustainability. [CrossRef]
- Govender, T. , & Arnedo-Moreno, J. (2021). An analysis of game design elements used in digital game-based language learning. Sustainability. [CrossRef]
- Pellas, N. , Mystakidis, S., & Christopoulos, A. (2021). A systematic literature review on the user experience design for game-based interventions via 3D virtual worlds in K-12 education. Multimodal Technologies and Interaction. [CrossRef]
- Ongoro, C. A. , & Fanjiang, Y. Y. (2023). Digital game-based technology for English language learning in preschools and primary schools: A systematic analysis. IEEE Transactions on Learning Technologies. [CrossRef]
- Chatterjee, A. , Prinz, A., Gerdes, M., Martinez, S., Pahari, N., & Meena, Y. K. (2022). ProHealth eCoach: User-centered design and development of an eCoach app to promote healthy lifestyle with personalized activity recommendations. BMC Health Services Research. [CrossRef]
- Ghahramani, A. , de Courten, M., & Prokofieva, M. (2022). The potential of social media in health promotion beyond creating awareness: An integrative review. BMC Public Health. [CrossRef]
- AlDaajeh, S. , Saleous, H., Alrabaee, S., Barka, E., Breitinger, F., & Choo, K. K. R. (2022). The role of national cybersecurity strategies on the improvement of cybersecurity education. Computers & Security. [CrossRef]
- Kulkov, I. , Kulkova, J., Rohrbeck, R., Menvielle, L., Kaartemo, V., & Makkonen, H. (2024). Artificial intelligence-driven sustainable development: Examining organizational, technical, and processing approaches to achieving global goals. Sustainable Development. [CrossRef]
- Cheng, L. (). Educational affordances of music video games and gaming mobile apps. Technology.
- Zahedi, L. , Batten, J., Ross, M., Potvin, G., Damas, S., Clarke, P., & Davis, D. (2021). Gamification in education: A mixed-methods study of gender on computer science students’ academic performance and identity development. Journal of Computing in Higher Education. [CrossRef]
- Weatherly, K. I. C. H. , Wright, B. A., & Lee, E. Y. (2024). Digital game-based learning in music education: A systematic review between 2011 and 2023. Research Studies in Music Education. [CrossRef]
- Crepax, T. , Muntés-Mulero, V., Martinez, J., & Ruiz, A. (2022). Information technologies exposing children to privacy risks: Domains and children-specific technical controls. Computer Standards & Interfaces. [CrossRef]
- Michael, K. (2024). Mitigating Risk and Ensuring Human Flourishing Using Design Standards: IEEE 2089-2021 an Age Appropriate Digital Services Framework for Children. IEEE Transactions on Technology and Society. [CrossRef]
- Wang, G. , Zhao, J., Van Kleek, M., & Shadbolt, N. (2022). Informing age-appropriate AI: Examining principles and practices of AI for children. Proceedings of the 2022 CHI Conference on Human Factors in Computing Systems. [CrossRef]
- Shrestha, A. K. , Barthwal, A., Campbell, M., Shouli, A., Syed, S., Joshi, S., & Vassileva, J. (2024). Navigating AI to unpack youth privacy concerns: An in-depth exploration and systematic review. arXiv:2412.16369.
- Zhao, D. , Inaba, M., & Monroy-Hernández, A. (2022). Understanding teenage perceptions and configurations of privacy on Instagram. Proceedings of the ACM on Human-Computer Interaction. [CrossRef]
- Andrews, J. C. , Walker, K. L., Netemeyer, R. G., & Kees, J. (2023). Helping youth navigate privacy protection: Developing and testing the children’s online privacy scale. Journal of Public Policy & Marketing. [CrossRef]
- Basyoni, L. , Tabassum, A., Shaban, K., Elmahjub, E., Halabi, O., & Qadir, J. (2024). Navigating Privacy Challenges in the Metaverse: A Comprehensive Examination of Current Technologies and Platforms. IEEE Internet of Things Magazine. [CrossRef]
- Udoudom, U. , George, K., & Igiri, A. (2023). Impact of digital learning platforms on behaviour change communication in public health education. Pancasila International Journal of Applied Social Science. [CrossRef]
- Ventouris, A. , Panourgia, C., & Hodge, S. (2021). Teachers’ perceptions of the impact of technology on children and young people’s emotions and behaviours. International Journal of Educational Research Open. [CrossRef]
- Novak, E. , McDaniel, K., Daday, J., & Soyturk, I. (2022). Frustration in technology-rich learning environments: A scale for assessing student frustration with e-textbooks. British Journal of Educational Technology. [CrossRef]
- Drljević, N. , Botički, I., & Wong, L. H. (2022). Investigating the different facets of student engagement during augmented reality use in primary school. British Journal of Educational Technology. [CrossRef]
- Buzzai, C. , Sorrenti, L., Costa, S., Toffle, M. E., & Filippello, P. (2021). The relationship between school-basic psychological need satisfaction and frustration, academic engagement and academic achievement. School Psychology International. [CrossRef]
- Christopoulos, A. , & Sprangers, P. (2021). Integration of educational technology during the Covid-19 pandemic: An analysis of teacher and student receptions. Cogent Education. [CrossRef]
- Lynch, P. , Singal, N., & Francis, G. A. (2024). Educational technology for learners with disabilities in primary school settings in low-and middle-income countries: A systematic literature review. Educational Review. [CrossRef]
- Balalle, H. (2024). Exploring student engagement in technology-based education in relation to gamification, online/distance learning, and other factors: A systematic literature …. Social Sciences & Humanities Open. [CrossRef]
- Chen, F. H. (2021). Sustainable education through e-learning: The case study of iLearn2.0. Sustainability. [CrossRef]
- Zohari, M. , Karim, N., Malgard, S., Aalaa, M., Asadzandi, S., & Borhani, S. (2023). Comparison of gamification, game-based learning, and serious games in medical education: A scientometrics analysis. Journal of Advances in Medical Education & Professionalism.
- Leonardou, A. , Rigou, M., Panagiotarou, A., & Garofalakis, J. (2022). Effect of OSLM features and gamification motivators on motivation in DGBL: Pupils’ viewpoint. Smart Learning Environments. [CrossRef]
- Guan, X. , Sun, C., Hwang, G. J., Xue, K., & Wang, Z. (2024). Applying game-based learning in primary education: A systematic review of journal publications from 2010 to 2020. Interactive Learning Environments. [CrossRef]
- Camacho-Sánchez, R. , Manzano-León, A., Rodríguez-Ferrer, J. M., Serna, J., & Lavega-Burgués, P. (2023). Game-based learning and gamification in physical education: A systematic review. Education Sciences. [CrossRef]
- Hsiao, W. Y. , Chen, C. H., Chen, P. C., & Hou, W. H. (2024). Investigating the effects of different game-based learning on the health care knowledge and emotions for middle-aged and older adults. Interactive Learning Environments. [CrossRef]
- Hsiao, W. Y. , Chen, C. H., Chen, P. C., & Hou, W. H. (2024). Investigating the effects of different game-based learning on the health care knowledge and emotions for middle-aged and older adults. Interactive Learning Environments. [CrossRef]
- Gkintoni, E. , Vantaraki, F., Skoulidi, C., Anastassopoulos, P., & Vantarakis, A. (2024). Promoting Physical and Mental Health among Children and Adolescents via Gamification—A Conceptual Systematic Review. Behavioral Sciences, 14(2), 102. [CrossRef]
- Gajardo Sánchez, A. D. , Murillo-Zamorano, L. R., López-Sánchez, J., & Bueno-Muñoz, C. (2023). Gamification in health care management: Systematic review of the literature and research agenda. SAGE Open, 13(4), 21582440231218834. [CrossRef]
- Arruzza, E. , & Chau, M. (2021). A scoping review of randomized controlled trials to assess the value of gamification in the higher education of health science students. Journal of Medical Imaging and Radiation Sciences. [CrossRef]
- Arora, C. , & Razavian, M. (2021). Ethics of gamification in health and fitness tracking. International Journal of Environmental Research and Public Health, 18(21), 11052. [CrossRef]
- Warsinsky, S. , Schmidt-Kraepelin, M., Rank, S., Thiebes, S., & Sunyaev, A. (2021). Conceptual ambiguity surrounding gamification and serious games in healthcare: Literature review and development of game-based intervention reporting guidelines (GAMING). Journal of Medical Internet Research, 23(9), e30390. [CrossRef]
- Cheng, C. , & Ebrahimi, O. V. (2023). A meta-analytic review of gamified interventions in mental health enhancement. Computers in Human Behavior. [CrossRef]
- Aguiar-Castillo, L. , & Clavijo-Rodriguez, A. (2021). Gamification and deep learning approaches in higher education. Journal of Hospitality, Leisure, Sport & Tourism Education. [CrossRef]
- Cheng, C. , & Ebrahimi, O. V. (2023). Gamification: A novel approach to mental health promotion. Current Psychiatry Reports. [CrossRef]
- Lynch, Z. , & Sankey, M. (2016). Reboot your course—From Beta to better.
- Landers, R. N. , & Sanchez, D. R. (2022). Game-based, gamified, and gamefully designed assessments for employee selection: Definitions, distinctions, design, and validation. International Journal of Selection and Assessment, 30(1), 1-13. [CrossRef]
- Mazeas, A. , Duclos, M., Pereira, B., & Chalabaev, A. (2022). Evaluating the effectiveness of gamification on physical activity: Systematic review and meta-analysis of randomized controlled trials. Journal of Medical Internet Research, 24(1), e26779. [CrossRef]
- Furtado, L. S. , de Souza, R. F., Lima, J. L. D. R., & Oliveira, S. R. B. (2021). Teaching method for software measurement process based on gamification or serious games: A systematic review of the literature. International Journal of Computer Games Technology, 2021(1), 8873997. [CrossRef]
- Krath, J. , Schürmann, L., & Von Korflesch, H. F. O. (2021). Revealing the theoretical basis of gamification: A systematic review and analysis of theory in research on gamification, serious games, and game-based learning. Computers in Human Behavior. [CrossRef]
- Khaleghi, A. , Aghaei, Z., & Mahdavi, M. A. (2021). A gamification framework for cognitive assessment and cognitive training: Qualitative study. JMIR Serious Games, 9(1), e21900. [CrossRef]
- Sezgin, S. , & Yüzer, T. V. (2022). Analyzing adaptive gamification design principles for online courses. Behaviour & Information Technology. [CrossRef]
- Li, Q. , Yin, X., Yin, W., Dong, X., & Li, Q. (2023). Evaluation of gamification techniques in learning abilities for higher school students using FAHP and EDAS methods. Soft Computing. [CrossRef]
- Aresi, G. , Chiavegatti, B., & Marta, E. (2024). Participants’ experience with gamification elements of a school-based health promotion intervention in Italy: A mixed-methods study. Journal of Prevention. [CrossRef]
- Ibrahim, E. N. M. , Jamali, N., Suhaimi, A. I. H. (2021). Exploring gamification design elements for mental health support. International Journal of Advanced Technology and Engineering Exploration, 8(74), 114. [CrossRef]
- Alamri, I. K. A. (2024). Gameful learning: Investigating the impact of game elements, interactivity, and learning style on students’ success. Multidisciplinary Science Journal. [CrossRef]
- Vorlíček, M. , Prycl, D., Heidler, J., Herrador-Colmenero, M., Nábělková, J., Mitáš, J.,... & Frömel, K. (2024). Gameful education: A study of Gamifiter application’s role in promoting physical activity and active lifestyle. Smart Learning Environments, 11(1), 1-14. [CrossRef]
- Qiu, Y. (2024). The role of playfulness in gamification for health behavior motivation.
- De Salas, K. , Ashbarry, L., Seabourne, M., Lewis, I., Wells, L., Dermoudy, J.,... & Scott, J. (2022). Improving environmental outcomes with games: An exploration of behavioral and technological design and evaluation approaches. Simulation & Gaming, 53(5), 470-512. [CrossRef]
- Kim, J. , & Castelli, D. M. (2021). Effects of gamification on behavioral change in education: A meta-analysis. International Journal of Environmental Research and Public Health, 18(7), 3550. [CrossRef]
- Shahzad, M. F. , Xu, S., Rehman, O., & Javed, I. (2023). Impact of gamification on green consumption behavior integrating technological awareness, motivation, enjoyment, and virtual CSR. Scientific Reports. [CrossRef]
- Xu, J. , Lio, A., Dhaliwal, H., Andrei, S., Balakrishnan, S., Nagani, U., & Samadder, S. (2021). Psychological interventions of virtual gamification within academic intrinsic motivation: A systematic review. Journal of Affective Disorders, 293, 444-465. [CrossRef]
- Jingili, N. , Oyelere, S. S., Nyström, M. B., Anyshchenko, L. (2023). A systematic review on the efficacy of virtual reality and gamification interventions for managing anxiety and depression. Frontiers in Digital Health, 5, 1239435. [CrossRef] [PubMed]
- Sinha, N. (2021). Introducing gamification for advancing current mental healthcare and treatment practices. IoT in Healthcare and Ambient Assisted Living. [CrossRef]
- Hassan Alhazmi, A. , & Asanka Gamagedara Arachchilage, N. (2023). Evaluation of game design framework using a gamified browser-based application.
- Di Minin, E. , Fink, C, Hausmann, A., Kremer, J., Kulkarni, R. (2021). How to address data privacy concerns when using social media data in conservation science. Conservation Biology ( 35(2), 437-–446. [CrossRef] [PubMed]
- Lee, C. , & Ahmed, G. (2021). Improving IoT privacy, data protection, and security concerns. International Journal of Technology, Innovation and Management (IJTIM), 1(1), 18-33. [CrossRef] [PubMed]
- Komljenovic, J. (2022). The future of value in digitalised higher education: Why data privacy should not be our biggest concern. Higher Education. [CrossRef]
- Birch, K. , Cochrane, D. T., & Ward, C. (2021). Data as asset? The measurement, governance, and valuation of digital personal data by Big Tech. Big Data & Society. [CrossRef]
- Quach, S. , Thaichon, P., Martin, K. D., Weaven, S., & Palmatier, R. W. (2022). Digital technologies: Tensions in privacy and data. Journal of the Academy of Marketing Science, 50(6), 1299-1323. [CrossRef]
- Lappeman, J. , Marlie, S., Johnson, T., & Poggenpoel, S. (2022). Trust and digital privacy: Willingness to disclose personal information to banking chatbot services. Journal of Financial Services Marketing, 28(2), 337. [CrossRef]
- Hayes, J. L. , Brinson, N. H., Bott, G. J., & Moeller, C. M. (2021). The influence of consumer-brand relationships on the personalized advertising privacy calculus in social media. Journal of Interactive Marketing, 55(1), 16-30. [CrossRef]
- Cichy, P. , Salge, T. O., & Kohli, R. (2021). Privacy concerns and data sharing in the Internet of Things: Mixed methods evidence from connected cars. MIS Quarterly. [CrossRef]
- Trang, S. , & Weiger, W. H. (2021). The perils of gamification: Does engaging with gamified services increase users’ willingness to disclose personal information? Computers in Human Behavior. [CrossRef]
- Ruggiu, D. , Blok, V., Coenen, C., Kalloniatis, C., Kitsiou, A., Mavroeidi, A. G.,... & Sitzia, A. (2022). Responsible innovation at work: Gamification, public engagement, and privacy by design. Journal of Responsible Innovation, 9(3), 315-343. [CrossRef]
- Farhan, K. A. , Asadullah, A. B. M., Kommineni, H. P., Gade, P. K., & Venkata, S. S. M. G. N. (2023). Machine learning-driven gamification: Boosting user engagement in business. Global Disclosure of Economics and Business, 12(1), 41-52. [CrossRef]
- Van Toorn, C. , Kirshner, S. N., & Gabb, J. (2022). Gamification of query-driven knowledge sharing systems. Behaviour & Information Technology, 41(5), 959-980. [CrossRef]
- Simonofski, A. , Zuiderwijk, A., Clarinval, A., & Hammedi, W. (2022). Tailoring open government data portals for lay citizens: A gamification theory approach. International Journal of Information Management, 65, 102511. [CrossRef]
- Oliveira, W. , Hamari, J., Joaquim, S., Toda, A. M., Palomino, P. T., Vassileva, J., & Isotani, S. (2022). The effects of personalized gamification on students’ flow experience, motivation, and enjoyment. Smart Learning Environments, 9(1), 16. [CrossRef]
- Xiao, R. , Wu, Z., & Hamari, J. (2022). Internet-of-gamification: A review of literature on IoT-enabled gamification for user engagement. International Journal of Human-Computer Interaction, 38(12), 1113-1137. [CrossRef]
- Al-Rayes, S. , Al Yaqoub, F. A., Alfayez, A., Alsalman, D., Alanezi, F., Alyousef, S., ... Alanzi, T. M. (2022). Gaming elements, applications, and challenges of gamification in healthcare. Informatics in Medicine Unlocked, 31, 100974. [CrossRef]
- Esmaeilzadeh, P. (2021). The influence of gamification and information technology identity on postadoption behaviors of health and fitness app users: Empirical study in the United States. JMIR Serious Games. [CrossRef]
- Andrea Navarro-Espinosa, J. , Vaquero-Abellán, M., Perea-Moreno, A. J., Pedrós-Pérez, G., del Pilar Martínez-Jiménez, M., & Aparicio-Martínez, P. (2022). Gamification as a promoting tool of motivation for creating sustainable higher education institutions. International Journal of Environmental Research and Public Health. [CrossRef]
- Alam, A. (2023, March). Leveraging the power of ’modeling and computer simulation’ for education: An exploration of its potential for improved learning outcomes and enhanced student engagement. In 2023 International Conference on Device Intelligence, Computing and Communication Technologies (DICCT) (pp. 445-450). IEEE. [CrossRef]
- Gkintoni, E. , Antonopoulou, H., Sortwell, A., & Halkiopoulos, C. (2025). Challenging Cognitive Load Theory: The Role of Educational Neuroscience and Artificial Intelligence in Redefining Learning Efficacy. Brain Sciences, 15(2), 203. [CrossRef]
Figure 1.
iLearn4Health Platform Flowchart.
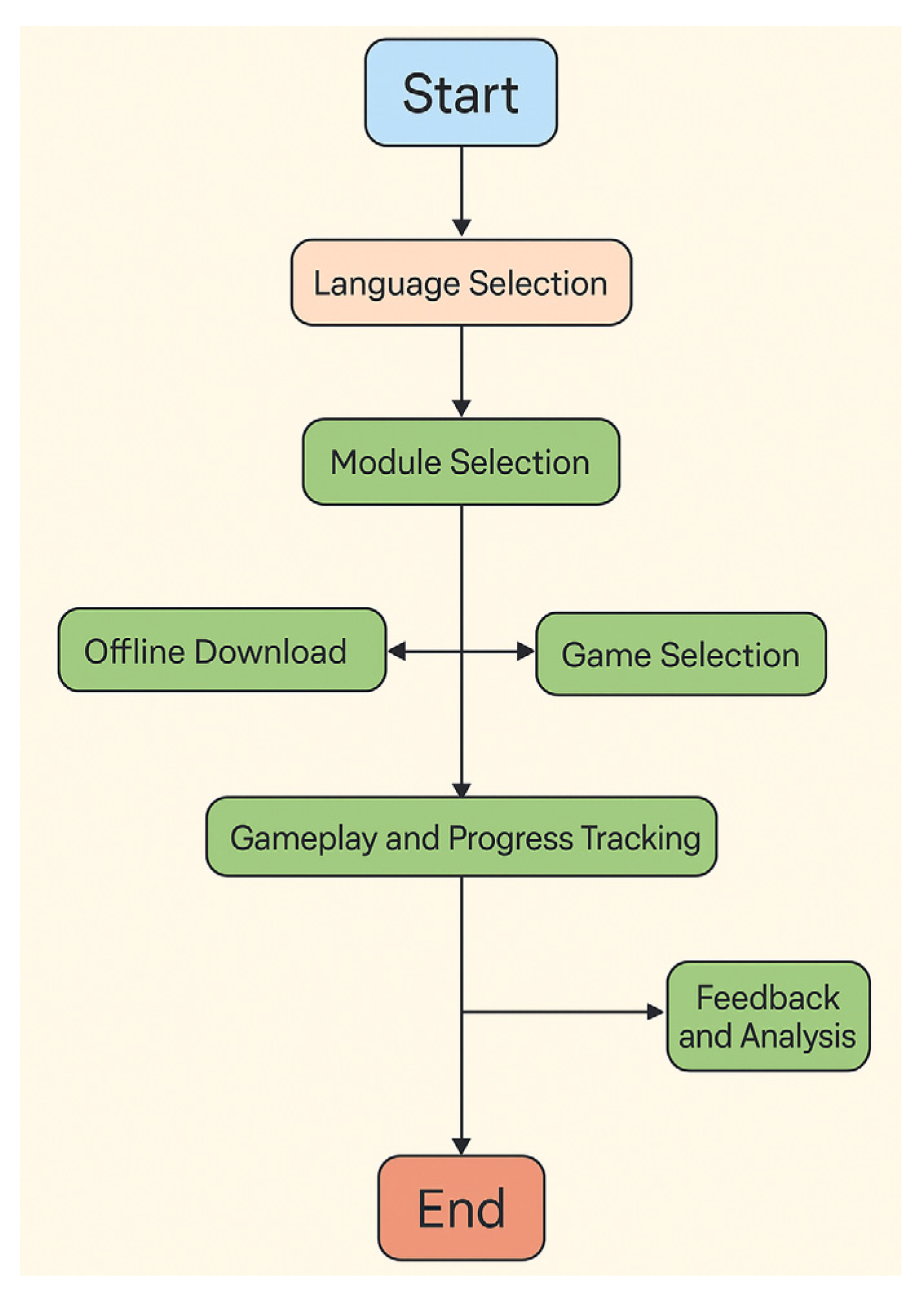
Figure 2.
iLearn4Health Online Training Program.
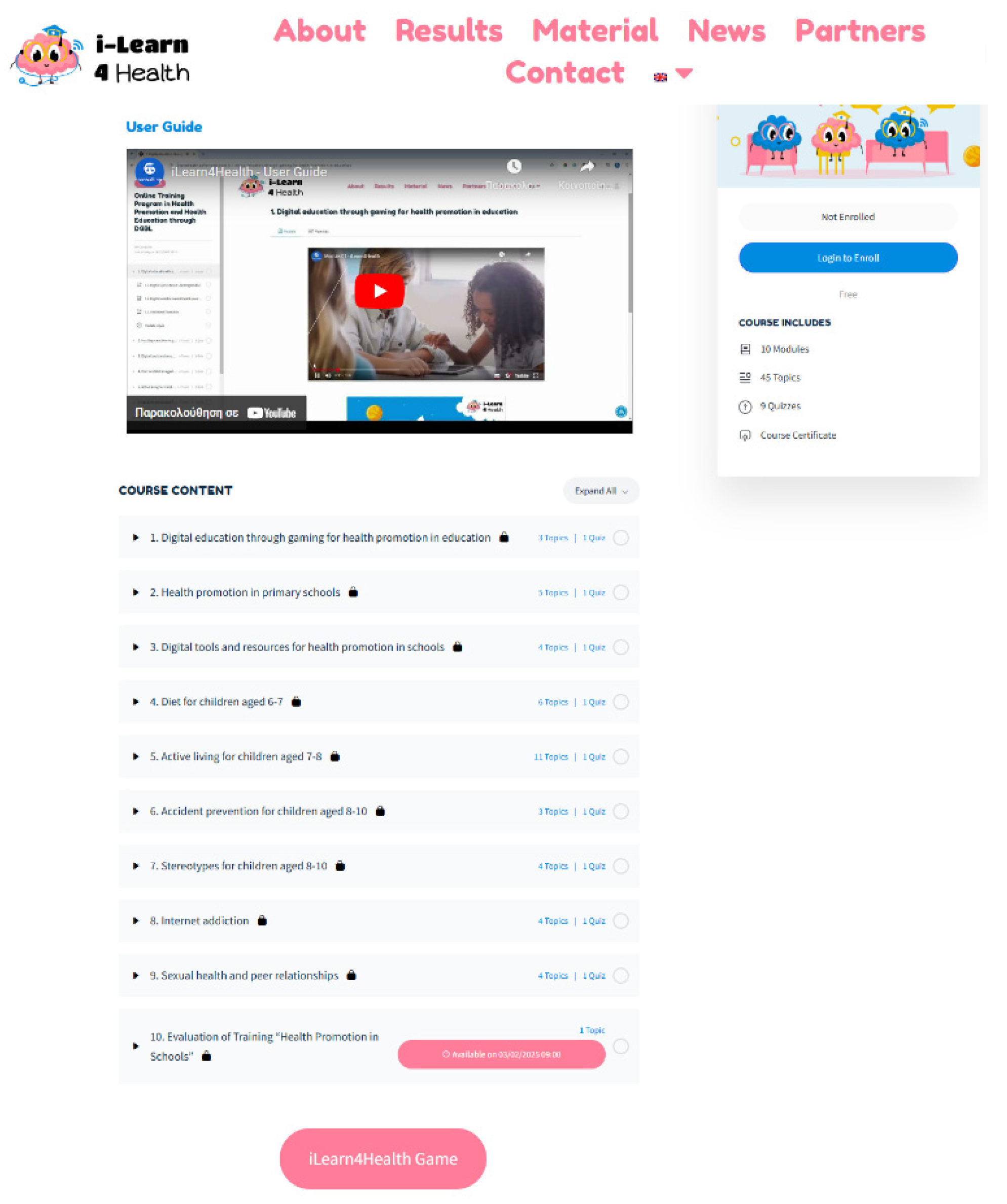
Figure 3.
Interactive Educational Game Screens Promoting Healthy Lifestyle Choices—iLearn4Health.

Figure 4.
Interactive Educational Game Screens Promoting Healthy Lifestyle Choices—iLearn4Health.
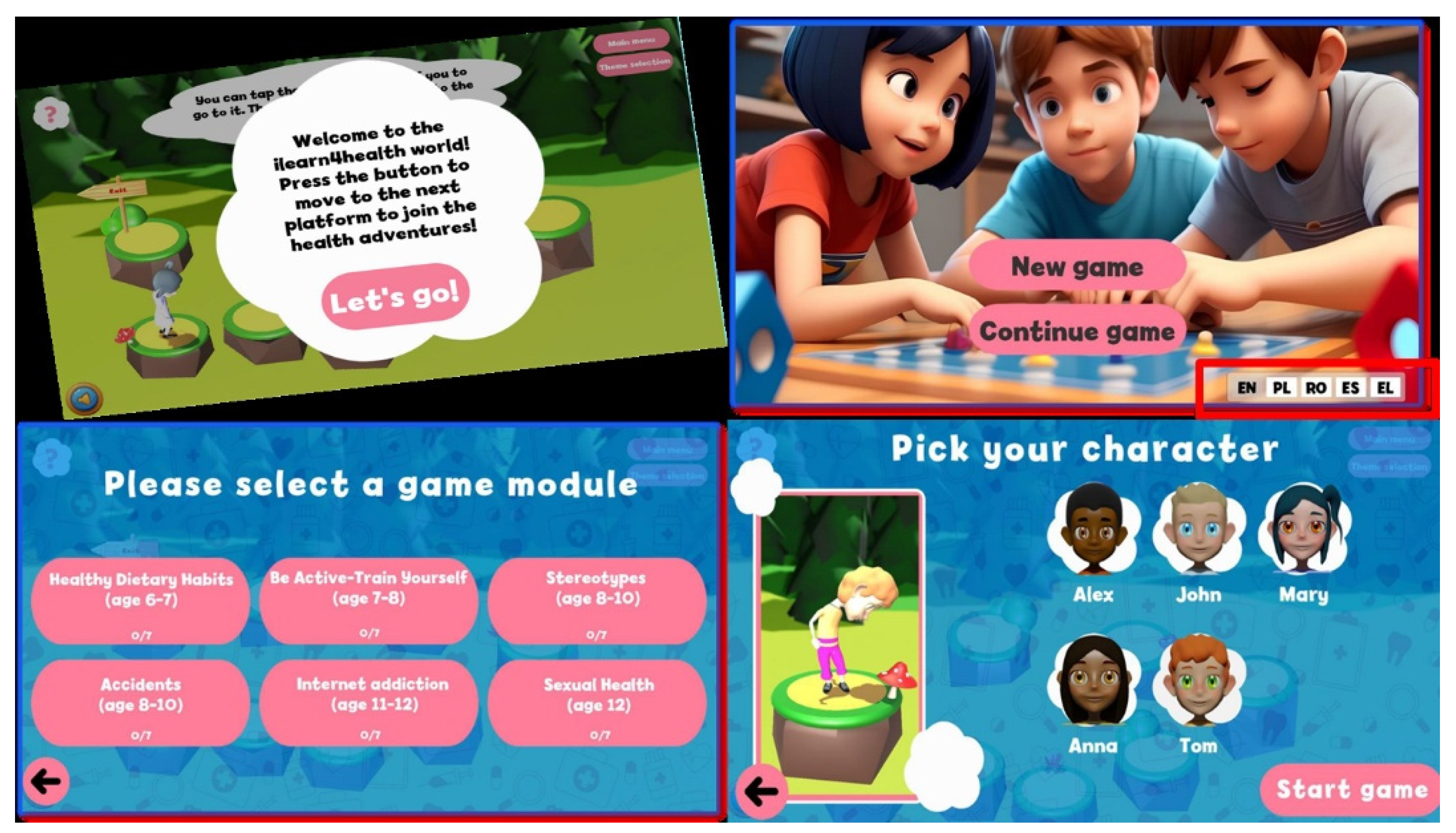
Figure 1.
Distribution of progress ratios among participants (N = 337) showing bimodal engagement pattern with 52.8% of users demonstrating low engagement (progress ratio 0.0-0.2) and 35.3% showing high engagement (progress ratio 0.8-1.0).
Figure 1.
Distribution of progress ratios among participants (N = 337) showing bimodal engagement pattern with 52.8% of users demonstrating low engagement (progress ratio 0.0-0.2) and 35.3% showing high engagement (progress ratio 0.8-1.0).
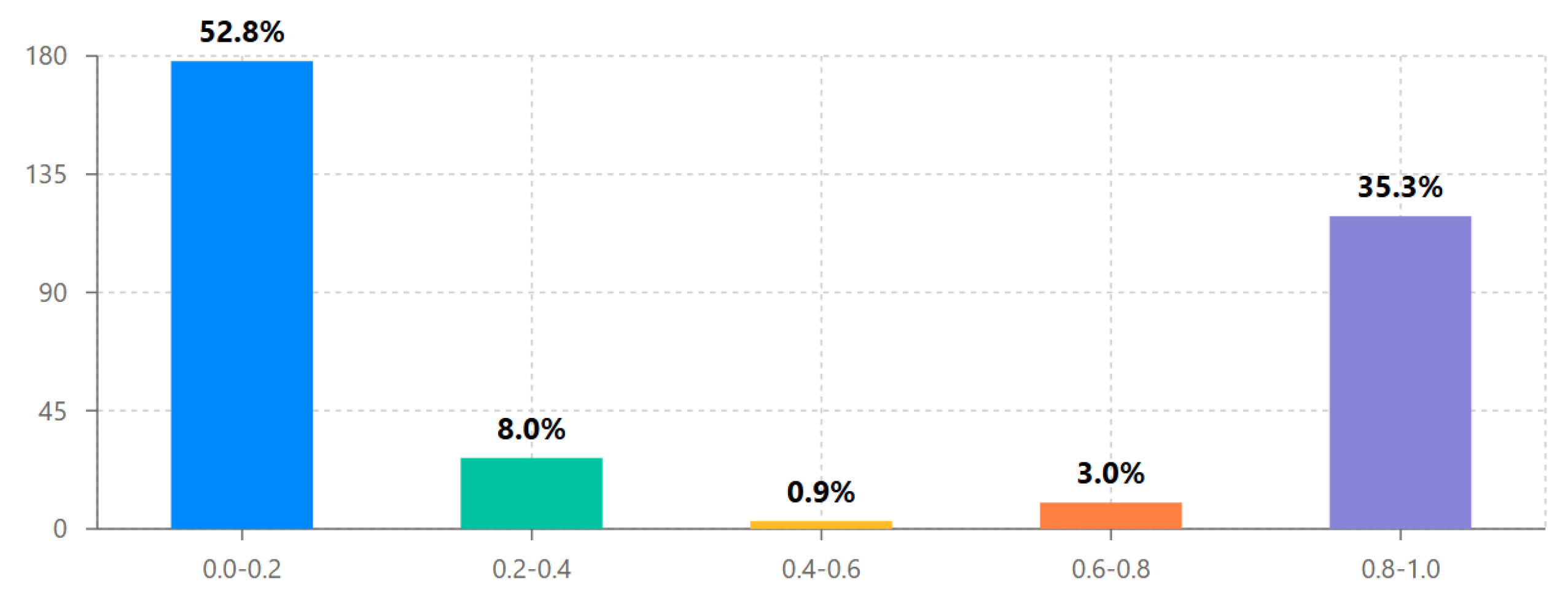
Figure 2.
Average steps completed by age group with 95% confidence intervals. The 26-35 age group shows highest average engagement (M = 24.83, SD = 23.15) while correlation between age and steps completed across the full sample was minimal (r = .01, p = .859).
Figure 2.
Average steps completed by age group with 95% confidence intervals. The 26-35 age group shows highest average engagement (M = 24.83, SD = 23.15) while correlation between age and steps completed across the full sample was minimal (r = .01, p = .859).
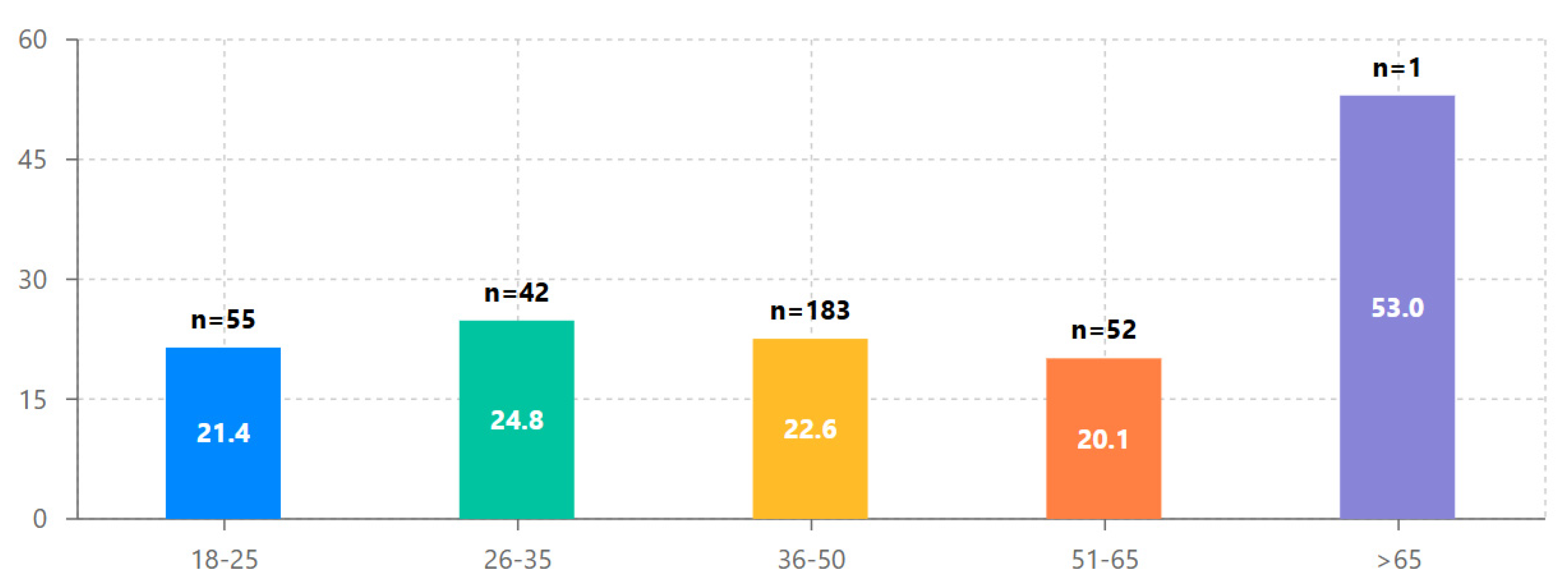
Figure 3.
Cross-national comparison of average progress ratios with 95% confidence intervals. Romania demonstrates significantly higher engagement (M = 0.460, SD = 0.44) than Greece (M = 0.315, SD = 0.40) and Cyprus (M = 0.301, SD = 0.38), suggesting important contextual factors in DGBL implementation.
Figure 3.
Cross-national comparison of average progress ratios with 95% confidence intervals. Romania demonstrates significantly higher engagement (M = 0.460, SD = 0.44) than Greece (M = 0.315, SD = 0.40) and Cyprus (M = 0.301, SD = 0.38), suggesting important contextual factors in DGBL implementation.
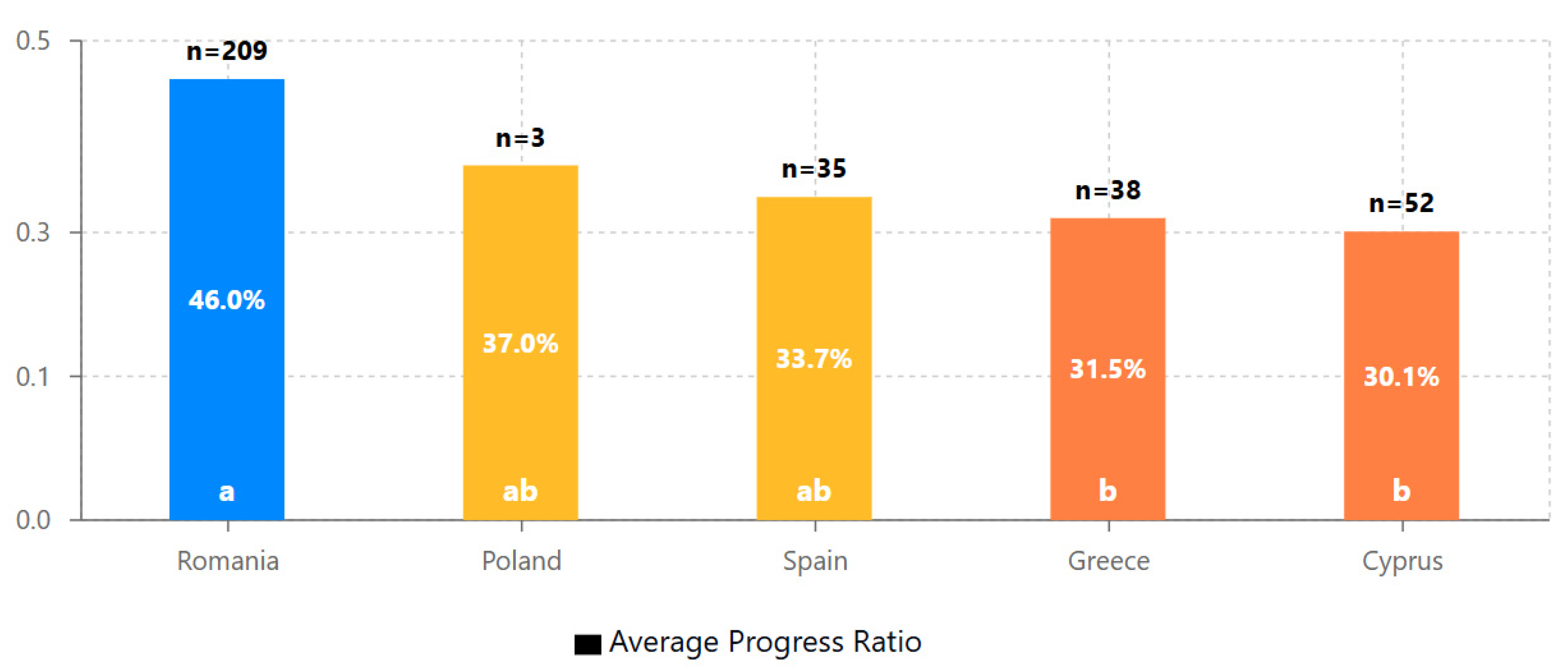
Figure 4.
Scatter plot showing the strong positive correlation between steps completed and time spent (r = .95, p < .001). The linear relationship demonstrates that sustained engagement is crucial for progression through the educational modules.
Figure 4.
Scatter plot showing the strong positive correlation between steps completed and time spent (r = .95, p < .001). The linear relationship demonstrates that sustained engagement is crucial for progression through the educational modules.
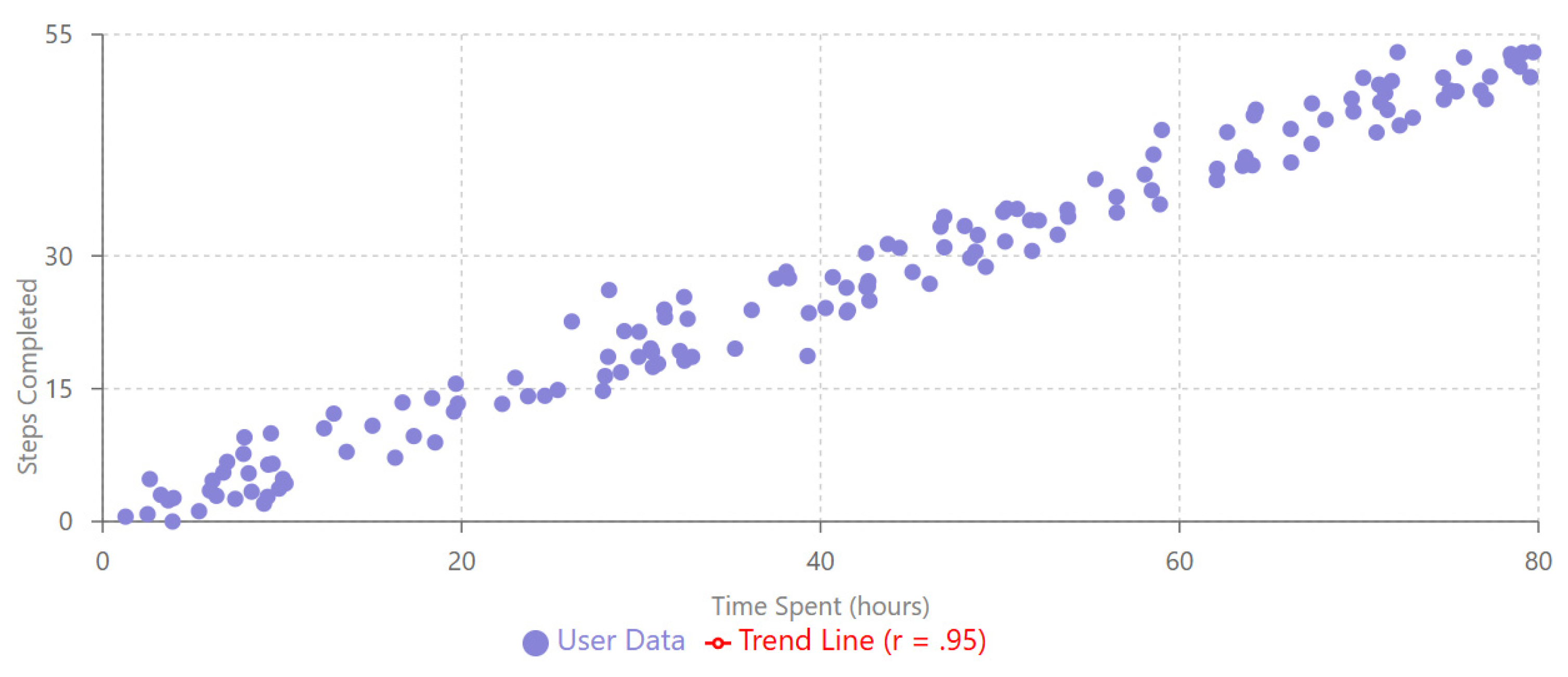
Figure 5.
Forest plot showing standardized regression coefficients (β) with 95% confidence intervals for predictors of progress ratio. Initial engagement (β = 0.479, p < .001) and country (Romania vs. Cyprus, β = 0.183, p = .001) emerge as the strongest predictors, while age has a more minor but significant effect (β = 0.108, p = .049). Blue bars indicate statistically significant predictors (p < .05).
Figure 5.
Forest plot showing standardized regression coefficients (β) with 95% confidence intervals for predictors of progress ratio. Initial engagement (β = 0.479, p < .001) and country (Romania vs. Cyprus, β = 0.183, p = .001) emerge as the strongest predictors, while age has a more minor but significant effect (β = 0.108, p = .049). Blue bars indicate statistically significant predictors (p < .05).
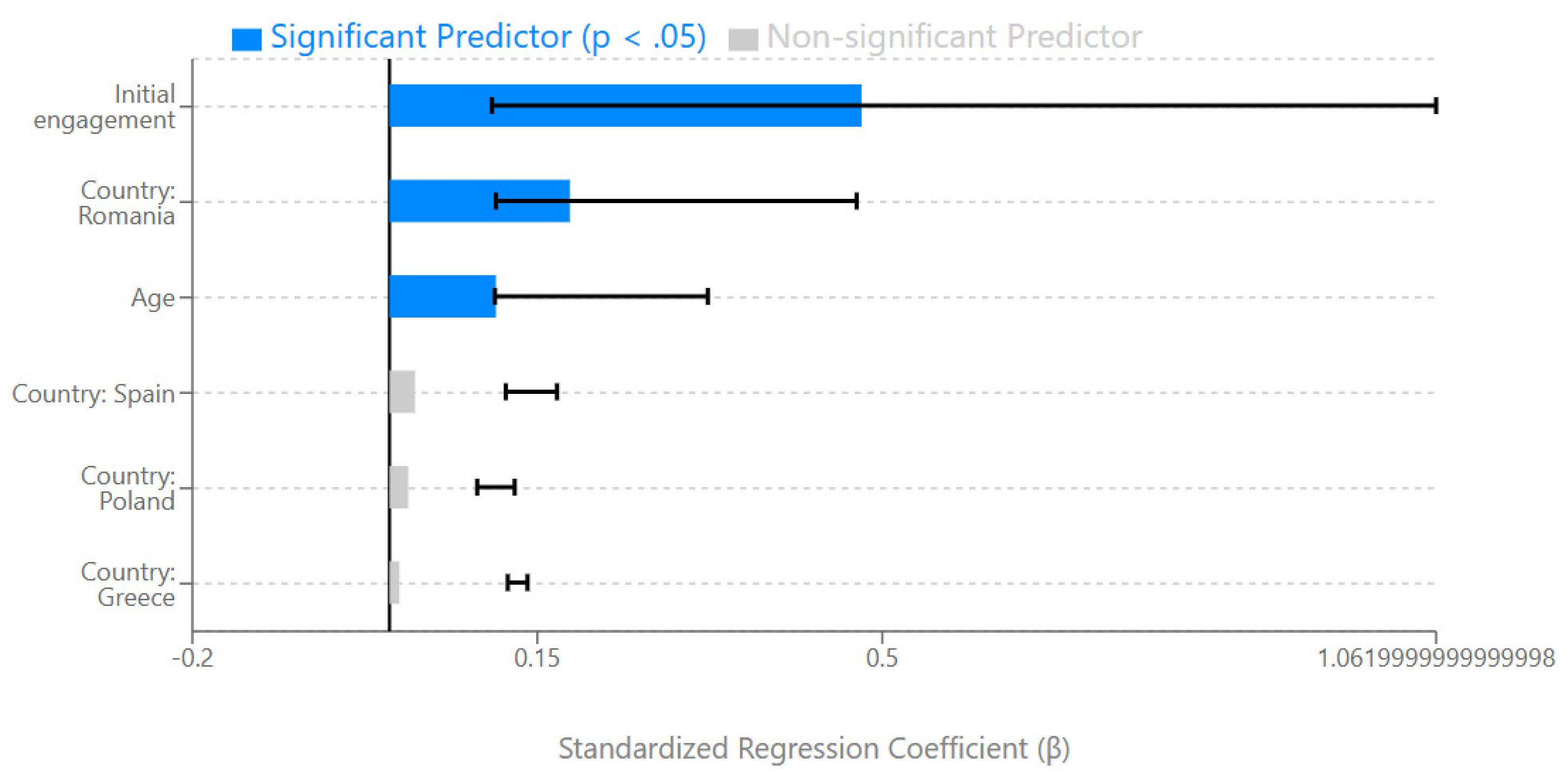
Figure 6.
Cluster analysis results showing three distinct user engagement profiles: high engagers (35.3%), early dropouts (52.8%), and selective engagers (11.9%). The clear separation between clusters confirms the qualitatively different engagement patterns observed in the bimodal distribution.
Figure 6.
Cluster analysis results showing three distinct user engagement profiles: high engagers (35.3%), early dropouts (52.8%), and selective engagers (11.9%). The clear separation between clusters confirms the qualitatively different engagement patterns observed in the bimodal distribution.
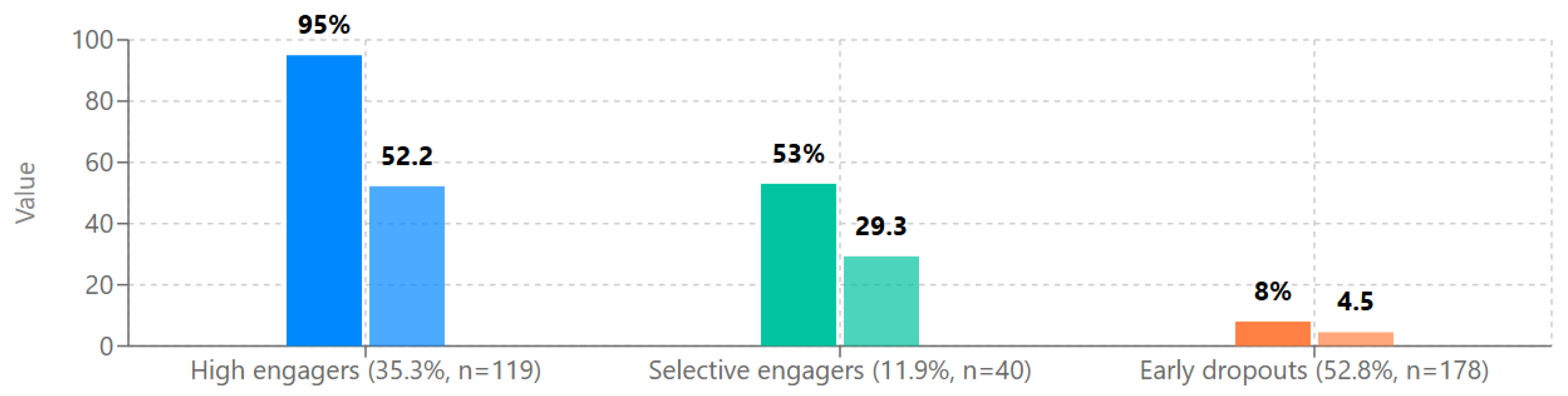

Table 1.
Descriptive Statistics for Participant Demographics and Platform Engagement (N = 337).
| Variable | M | SD | Min | Max | Mdn | Skewness | Kurtosis |
|---|---|---|---|---|---|---|---|
| Age (years) | 38.64 | 14.04 | 18 | 66 | 41 | -0.27 | -0.83 |
| Steps completed | 22.31 | 23.79 | 0 | 53 | 8 | 0.31 | -1.85 |
| Progress ratio | 0.41 | 0.43 | 0 | 0.96 | 0.15 | 0.47 | -1.74 |
Note. Progress ratio was calculated as steps completed divided by total possible steps (55).
Table 2.
Participant Distribution by Country.
| Country | n | % | 95% CI |
|---|---|---|---|
| Romania | 209 | 62.0 | [56.8, 67.2] |
| Cyprus | 52 | 15.4 | [11.5, 19.3] |
| Greece | 38 | 11.3 | [7.9, 14.7] |
| Spain | 35 | 10.4 | [7.1, 13.7] |
| Poland | 3 | 0.9 | [0, 1.9] |
Note. CI = confidence interval.
Table 3.
Bimodal Distribution of User Progress Ratios.
| Progress ratio | n | % | Cumulative % |
|---|---|---|---|
| 0.0-0.2 | 178 | 52.8 | 52.8 |
| 0.2-0.4 | 27 | 8.0 | 60.8 |
| 0.4-0.6 | 3 | 0.9 | 61.7 |
| 0.6-0.8 | 10 | 3.0 | 64.7 |
| 0.8-1.0 | 119 | 35.3 | 100.0 |
Note. Progress ratio ranges represent: 0.0-0.2 (low engagement), 0.2-0.4 (medium-low engagement), 0.4-0.6 (medium engagement), 0.6-0.8 (medium-high engagement), and 0.8-1.0 (high engagement).
Table 4.
Age-Based Engagement Patterns with Cohen’s d Effect Sizes.
| Age group | n | Steps completed | Progress ratio | Cohen’s d | |||
|---|---|---|---|---|---|---|---|
| M | SD | 95% CI | M | SD | |||
| 18-25 | 55 | 21.45 | 22.87 | [15.20, 27.70] | 0.39 | 0.42 | - |
| 26-35 | 42 | 24.83 | 23.15 | [17.61, 32.05] | 0.45 | 0.42 | 0.14 |
| 36-50 | 183 | 22.55 | 24.16 | [19.02, 26.08] | 0.41 | 0.44 | 0.05 |
| 51-65 | 52 | 20.10 | 24.33 | [13.32, 26.88] | 0.37 | 0.44 | -0.05 |
Note. Cohen’s d values represent effect sizes compared to the 18-25 age group. CI = confidence interval.
Table 5.
Cross-National Comparison of Progress Ratios with Post-Hoc Significance Testing.
| Country | n | Progress ratio | Significant differences | ||
|---|---|---|---|---|---|
| M | SD | 95% CI | |||
| Romania | 209 | 0.460 | 0.44 | [0.399, 0.521] | a |
| Poland | 3 | 0.370 | 0.41 | [0.000, 0.791] | a,b |
| Spain | 35 | 0.337 | 0.42 | [0.203, 0.471] | a,b |
| Greece | 38 | 0.315 | 0.40 | [0.190, 0.440] | b |
| Cyprus | 52 | 0.301 | 0.38 | [0.196, 0.406] | b |
Note. Countries that do not share the same letter suffix differ significantly according to Tukey’s HSD test at p < .05. CI = confidence interval.
Table 6.
One-Way ANOVA Results for Between-Country Differences in Progress Ratios.
| Source | SS | df | MS | F | p | η² |
|---|---|---|---|---|---|---|
| Between groups | 1.26 | 4 | 0.315 | 4.37 | .002 | .050 |
| Within groups | 23.94 | 332 | 0.072 | |||
| Total | 25.20 | 336 |
Note. η² = eta squared effect size.
Table 7.
Pearson Correlations Between Key Variables with Bootstrapped 95% Confidence Intervals.
| Variables | r | 95% CI | p |
|---|---|---|---|
| Steps completed—Time spent | .95 | [.93, .97] | < .001 |
| Age—Steps completed (full sample) | .01 | [-.10, .12] | .859 |
| Age—Steps completed (adult subgroup) | .80 | [.73, .85] | < .001 |
| Age—Time spent (adult subgroup) | .60 | [.50, .69] | < .001 |
| Progress ratio—Time spent | .94 | [.91, .96] | < .001 |
Note. Confidence intervals were calculated using bootstrapping with 1,000 samples. CI = confidence interval.
Table 8.
Multiple Regression Analysis Predicting Progress Ratio from Age, Country, and Initial Engagement.
Table 8.
Multiple Regression Analysis Predicting Progress Ratio from Age, Country, and Initial Engagement.
| Predictor | B | SE B | β | t | p | 95% CI |
|---|---|---|---|---|---|---|
| Constant | 0.210 | 0.074 | 2.84 | .005 | [0.065, 0.355] | |
| Age | 0.003 | 0.002 | 0.108 | 1.97 | .049 | [0.000, 0.006] |
| Initial engagement* | 0.346 | 0.038 | 0.479 | 9.11 | < .001 | [0.271, 0.421] |
| Country: Romania† | 0.159 | 0.048 | 0.183 | 3.31 | .001 | [0.065, 0.253] |
| Country: Spain† | 0.036 | 0.065 | 0.026 | 0.55 | .580 | [-0.092, 0.164] |
| Country: Greece† | 0.014 | 0.063 | 0.010 | 0.22 | .825 | [-0.110, 0.138] |
| Country: Poland† | 0.069 | 0.165 | 0.019 | 0.42 | .676 | [-0.256, 0.394] |
Note. R² = .31, F(6, 330) = 24.36, p < .001. CI = confidence interval. *Initial engagement measured by completion of first 10 steps (binary: yes/no) †Reference category is Cyprus.
Table 9.
Cluster Analysis Results: User Typologies Based on Engagement Patterns.
| Cluster | n | Age | Steps completed |
Progress ratio |
Time spent (min) | Key characteristics |
||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | M | SD | M | SD | |||
| High engaging modules | 119 | 39.8 | 12.6 | 52.2 | 1.6 | 0.95 | 0.03 | 987.4 | 463.2 | Complete most/all modules |
| Early dropouts | 178 | 38.1 | 14.9 | 4.5 | 3.8 | 0.08 | 0.07 | 65.3 | 52.8 | Disengage after initial exploration |
| Selective Engagers | 40 | 37.9 | 13.5 | 29.3 | 7.1 | 0.53 | 0.13 | 384.6 | 159.7 | Complete specific topics of interest |
Note. Clusters were identified using k-means clustering algorithm based on progress ratio and engagement pattern variables.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



