Submitted:
28 April 2025
Posted:
29 April 2025
You are already at the latest version
Abstract
This study conducted research on data mining and analysis of post-marketing adverse events related to the neuropsychiatric safety of Sacubitril/Valsartan using the FDA Adverse Event Reporting System (FAERS) database. The goal was to provide guidance for the safe clinical use of Sacubitril/Valsartan. By retrieving relevant reports from Q3 2015 to Q4 2023 and applying Reporting Odds Ratio (ROR) and Proportional Reporting Ratio (PRR) methods for signal detection, we found that Sacubitril/Valsartan, in addition to known common adverse reactions (such as hypotension, hyperkalemia, cough, and vertigo), Sacubitril/Valsartan may also be associated with a range of rare neurological and psychiatric symptoms, including memory impairment, cerebrovascular accidents, stress, and amnesia. A total of 19,688 cases of neuropsychiatric adverse events were attributed to Sacubitril/Valsartan, accounting for 22.20% of all reported adverse events. These adverse events were particularly prevalent among elderly patients. Among the adverse neuropsychiatric events, there were 226 deaths (3.53%), with 17 out of 37 neuropsychiatric symptom-related Preferred Terms (PTs) associated with death as an outcome. This study highlights the importance of closely monitoring the neuropsychiatric safety of patients treated with Sacubitril/Valsartan and provides new insights into the broader safety profile of this medication. However, as this analysis is based on a spontaneous reporting system, which may be subject to reporting bias and inaccuracies, therefore, these findings require further clinical research is necessary to validate these findings.
Keywords:
Sacubitril/Valsartan
; FDA Adverse Event Reporting System
; neuropsychiatric symptoms
; safety
1. Introduction
Cardiovascular diseases are the major threats to human health and remain the leading causes of death worldwide. Despite significant advances in their diagnosis and treatment, the high incidence and mortality rates continue to pose serious concerns [1]. Sacubitril/valsartan is the first angiotensin receptor neprilysin inhibitor (ARNI) approved in the United States and European Union. It exerts dual effects by inhibiting both angiotensin receptors and neprilysin (NEP) [2]. Sacubitril/valsartan is widely used in the management of heart failure [3,4]. Sacubitril is a pro-drug that is converted in the body to its active form, LBQ657, which inhibits NEP activity and reduces the degradation of natriuretic peptides and other vasoactive substances.
Valsartan blocks angiotensin II type 1 receptors, mitigating Ang II–induced effects and suppressing the renin-angiotensin-aldosterone system (RAAS) [5,6]. The most commonly reported adverse reactions include angioedema, hypotension, renal dysfunction, and hyperkalemia [7]. However, concerns have emerged about adverse effects potentially related to NEP inhibition of NEP have attracted extensive scholarly attention.
NEP is an enzyme responsible for degrading various peptides in the body. Chronic inhibition may lead to the accumulation of these peptides, potentially resulting in adverse outcomes, such as vascular edema, cancer, inflammation, and cognitive impairment [8]. Research has shown that the primary function of NEP plays a key role in degrading monomers and oligomers of amyloid β-protein (Aβ). Inhibiting NEP may lead to Aβ accumulation, which exerts neurotoxic effects when deposited in the extracellular matrix [9]. This has raised concerns about the potential impact of sacubitril/valsartan on brain health and its harm to neural function [10].
Although ongoing clinical trials have not identified adverse cognitive effects related to sacubitril/valsartan, and no such effects are listed in the medication guide, case reports have documented rare psychiatric adverse reactions that can cause significant distress to patients¹.
Using the real-world data from the FDA Adverse Event Reporting System (FAERS), we mined and analyzed risk signals of adverse drug events (ADEs) associated with sacubitril/valsartan, with a focus on neuropsychiatric symptoms. The goal is to update the safety profile regarding these symptoms and provide practical guidance for clinical use.
2. Methods
2.1. Study Design and Data Sources
The primary data for this study were obtained from the FDA Adverse Event Reporting System (FAERS) database. Adverse event reports related to sacubitril/valsartan were retrieved using OpenVigil 2.1 (https://openvigil.sourceforge.net/).
Since the approval of sacubitril/valsartan in July 2015, we collected adverse drug event (ADE) reports from the third quarter of 2015 through the fourth quarter of 2023. The dataset includes patient demographics (e.g., gender, age, regional distribution), pharmaceutical details (e.g., formulation, dosage, concomitant medications), descriptions of adverse reaction events, event outcomes (e.g., congenital anomaly, death, disability), and report dates.
After extracting the data extraction and de-duplication, we filtered for reports listing sacubitril/valsartan as the primary suspect drug (PS). Based on version 26.0 of the Medical Dictionary for Regulatory Activities (MedDRA), adverse events were classified according to Preferred Terms (PTs) and System Organ Classes (SOCs). Reports with identical PTs were consolidated [11,12]. For this study, SOCs related to Nervous System Disorders and Psychiatric Disorders were selected for further analysis. The incidence of adverse events was calculated for both the overall dataset and key subgroups. All data processing and analyses were performed using Microsoft Excel 2020.
2.2. Data Mining Algorithm
We employed a disproportionality analysis based on fourfold table metrics, using Reporting Odds Ratio (ROR) and Proportional Reporting Ratio (PRR) for signal detection. These methods are known for their computational simplicity, ability to estimate relative risk, and consistency of results.
For ROR, the value and its 95% confidence interval (CI) were calculated. A signal was considered positive when there were ≥3 cases and the lower limit of the bilateral 95% CI exceeded 1. For PRR, a signal was considered positive when there were ≥3 cases, the PRR was ≥2, and the chi-square (χ²) value was ≥4. An adverse event was defined as a signal when it met the criteria for both ROR and PRR methods.
The magnitudes of the ROR and PRR values reflect the strength of association between sacubitril/valsartan and the ADE: higher values indicate a stronger statistical correlation. Details are summarized in Table 1.
Equation: a, the number of target ADEs for the target drug; b ,the number of other ADEs for the target drug; c, the number of other ADEs for other drugs; d, the number of target ADEs for other drugs. ROR, reporting odds ratio; PRR, proportional reporting ratio; χ2, chi-squared.
3. Results
3.1. Descriptive Results
Between Q3 2015 and Q4 2023, the FAERS database recorded a total of 88,675 adverse event cases associated with sacubitril/valsartan. The clinical characteristics of these cases are summarized in Table 2.
After excluding cases with unspecified gender, males accounted for a higher total number of reported adverse events than females. Similarly, excluding cases with unknown age, the majority of adverse events occurred in individuals aged ≥65 years. When excluding cases with unknown or unspecified outcomes, death emerged as the most common outcome. The United States reported the highest number of cases overall.
3.2. Signal Values Associated with Sacubitril/Valsartan
After screening adverse events in which sacubitril/valsartan was identified as the primary suspect drug, a total of 86,658 adverse event reports with ≥3 cases were analyzed. This analysis identified 2,041 significant Preferred Terms (PTs). The top 50 adverse events associated with Sacubitril/valsartan, including the number of cases and corresponding signal strengths, are presented in Table 3.
Several known adverse reactions listed in the prescribing information were detected, including hypotension, hyperkalemia, cough, vertigo, renal failure, acute kidney injury, angioedema, increased blood creatinine, and generalized pruritus.
In addition, this study identified extremely rare adverse events such as decreased blood triglycerides, increased waist circumference increased, cardiac hypertrophy, ischemic hepatitis, and amaurosis. Notably, some adverse events that are frequently reported adverse events not included in the prescribing information were also detected. These include dizziness, dyspnea, fatigue, weight loss, cardiac failure, asthenia, weight gain, myocardial infarction, hypoacusis, feeling abnormal sensations, memory impairment, and hypertension.
All PTs were categorized into System Organ Classes (SOCs), involving a total of 27 SOCs, as shown in Figure 1. The top five SOCs were general disorders and administration site conditions; respiratory, thoracic and mediastinal disorders; investigations; nervous system disorders; gastrointestinal disorders. Nervous system disorders and psychiatric disorders ranked seventh and eighth, respectively.
3.3. Analysis of Nervous System and Psychiatric Disorders Associated with Sacubitril/Valsartan
This study focused on System Organ Classes (SOCs) related to the nervous system disorders and psychiatric disorders, identifying 19,688 adverse drug event (ADE) cases associated with sacubitril/valsartan. These accounted for 22.20% of all reported ADEs. The clinical characteristics are summarized in Table 4.
After excluding cases with unspecified gender, the total number of adverse events was higher in males than in females. Similarly, excluding cases with unknown age, the majority of adverse events occurred in individuals aged ≥65 years. When excluding cases with unspecified or other outcomes, the most common outcome of adverse events was hospitalization—initial or prolonged. The United States reported the highest number of cases overall.
3.4. Distribution of Preferred Terms (PTs) for Neuropsychiatric Adverse Events
Using the Reporting Odds Ratio (ROR) method, 56 Preferred Terms (PTs) related to neuropsychiatric symptoms were identified. The Proportional Reporting Ratio (PRR) method detected 37 PTs, with 37 PTs meeting the criteria for both methods—indicating a strong association between sacubitril/valsartan and neuropsychiatric adverse events (Table 5).
A total of 6,396 patients were included in this analysis. The top ten neuropsychiatric adverse event signals being memory impairment, cerebrovascular accident, stress, amnesia, speech disorder, dementia, orthostatic hypotension, hypokinesia, fear, and dementia of the Alzheimer’s type.
3.5. Analysis of PT deaths in neuropsychiatric symptoms ADEs
In reports of adverse reactions to the neuropsychiatric symptoms, the outcome of 17 PTs was death. There were 226 instances of fatalities, accounting for 3.53% of the total reported cases (Table 6). The irregular sleep phase has the highest proportion among them, and the cerebrovascular accident was the most reported case.
4. Discussion
Sacubitril/valsartan, the first angiotensin receptor–neprilysin inhibitor (ARNI), demonstrated superior efficacy and safety compared to enalapril in the PARADIGM-HF trial for patients with chronic heart failure (HF) patients (NYHA class II–IV, LVEF ≤35%), leading to its adoption as a first-line therapy in major clinical guidelines [13]. Sacubitril functions as a neprilysin (NEP) inhibitor. NEP is a zinc-dependent metalloprotease located on the cell membranes (also known as endopeptidase), widely distributed in the central nervous system (CNS), peripheral nervous system, kidneys, and systemic vascular endothelium, and also present in a soluble form in the blood, cerebrospinal fluid, and amniotic fluid [14,15,16,17]. NEP is involved in various brain functions through the regulation of neuropeptides, influencing sensory activities like pain perception and motor control [18]. Altering NEP activity may thus impact brain function. Sacubitril, with its low molecular weight and few hydrogen bonds, can cross the blood–brain barrier and directly affect amyloid β-protein (Aβ) deposition of Aβ in the CNS [19,20].
Langenickel and Schoenfeld conducted two studies evaluating the effect of sacubitril on Aβ metabolism in both monkeys and humans, assessing blood–brain barrier permeability and Aβ concentrations of Aβ in plasma and cerebrospinal fluid [21,22]. They found that sacubitril can effectively inhibits NEP in the brain and is retained in cerebrospinal fluid at significant levels—raising concerns about possible neurotoxic exposure. However, published case reports of neuropsychiatric symptoms linked to sacubitril/valsartan use remain limited [23]. In this study, we analyzed adverse drug events (ADEs) from the FAERS database, focusing on a large-scale analysis of real-world data regarding neuropsychiatric adverse reactions based on real-world data—marking the first large-scale monitoring report of its kind.
The most common adverse reactions to sacubitril/valsartan (with an incidence ≥5%) include hypotension, hyperkalemia, cough, dizziness, and renal failure, which are consistent with prior findings [24]. Additionally, we identified extremely rare ADE signals, such as decreased blood triglycerides, increased waist circumference, cardiac hypertrophy, ischemic hepatitis, and amaurosis. Some newly identified ADEs, if validated, could warrant updates to the drug's package insert.
The PARADIGM-HF trial's neurocognitive sub-analysis of the PARADIGM-HF study found no Alzheimer’s disease (AD)-related adverse effects within 27 months [25]. However, our FAERS-based signal detection analysis (using ROR and PRR methods) identified signals for memory impairment, dementia, and speech disorders. In animal studies, sacubitril/valsartan exacerbated cognitive decline in AD rat models, with increased Aβ deposition, oxidative stress, and inflammation compared to valsartan alone [26]. Case reports have described neuropsychiatric symptoms (e.g., anxiety, confusion) emerging after initiating or increasing the dose of sacubitril/valsartan [27]. In these cases, a clear temporal relationship was noted between dose initiation or escalation of sacubitril/valsartan, with improvements following dose reduction or discontinuation. These findings suggest a potential neurological impact, emphasizing the importance of regular cognitive assessments during therapy.
We also analyzed fatalities among neuropsychiatric-related ADEs. Death reports accounted for 3.53% of neuropsychiatric adverse events, with irregular sleep phase having the highest mortality rate among PTs, and cerebrovascular accident being the PT with the most reported deaths. A case report by Jessica Wooster noted in a case report that a patient experienced sleep disorders following sacubitril/valsartan use, which improved after stopping the drug [28]. This suggests that the medication may disrupt sleep architecture, leading to insomnia or frequent nocturnal awakenings. Furthermore, the drug’s blood pressure–lowering effects may reduce cerebral perfusion, potentially contributing to dizziness, headaches, and cerebrovascular events.
Elderly patients (≥65 years) represented the majority of reported neuropsychiatric events, likely due to decreased physiological resilience and heightened vulnerability to central nervous system effects. The large number of cerebrovascular accident reports—contradicting the drug’s therapeutic intent—suggests that clinicians should carefully weigh risks of serious cerebrovascular events when prescribing sacubitril/valsartan.
This study offers several strengths. First, it provides a comprehensive analysis of ADE signals and their intensity for sacubitril/valsartan using real-world pharmacovigilance data, offering greater external validity than clinical trials limited by small sample sizes or short durations. Second, it represents the most extensive real-world investigation to date based on real-world monitoring data concerning the neuropsychiatric risks of sacubitril/valsartan.
However, our study has limitations. As a spontaneous ADE reporting system, FAERS is subject to under-reporting, misreporting, and reporting biases, which may skew results. The absence of a true denominator (total exposed population) also precludes accurate incidence rate calculations. Although this study identified positive signals for cerebrovascular accidents and other ADEs in the neuropsychiatric ADEs not listed in the drug’s official labeling, these findings must be confirmed through well-designed clinical studies.
Lastly, while ROR and PRR methods offer simplicity and high sensitivity and simple calculation methods, they are susceptible to false positives. These statistical signals indicate associations, not causality. Further preclinical and clinical research is needed to validate these observations and inform evidence-based updates to prescribing information.
References
- Lavie, C. J. Progress in Cardiovascular Diseases Statistics 2022. Prog Cardiovasc Dis., 2022,73:94-95. [CrossRef]
- Huang, E.; Bernard, M.L.; Elise Hiltbold, A.; Khatib, S.; Polin, G.M.; Rogers, P.A.; Dominic, P.; Morin, D.P. Sacubitril/valsartan: An antiarrhythmic drug? J Cardiovasc Electrophysiol., 2022,33(11):2375-2381. [CrossRef]
- Sun, Y.; Yang, H. Comparison of sacubitril/valsartan with olmesartan for hypertension: A meta-analysis of randomized controlled trials. Medicine., 2024,103(14), e37501. [CrossRef]
- Mann, D.L.; Givertz, M.M.; Vader, J.M.; Starling, R.C.; Shah, P.; McNulty; S.E.; Anstrom, K.J.; Margulies, K.B.; Kiernan, M.S.; Mahr, C.; et al. Effect of Treatment With Sacubitril/Valsartan in Patients With Advanced Heart Failure and Reduced Ejection Fraction: A Randomized Clinical Trial. JAMA cardiology., 2022,7(1), 17–25. [CrossRef]
- Wang, F.; Li, C.; Zhang, X. Sacubitril/valsartan improves the prognosis of acute myocardial infarction: a meta-analysis. Coronary artery disease., 2024,35(3), 231–238. [CrossRef]
- Kuang, H.; Huang, X.; Zhou, Z.; Cheng, X.; Xu, G. Sacubitril/valsartan in chronic kidney disease: From pharmacological mechanism to clinical application. European journal of pharmacology., 2021,907, 174288. [CrossRef]
- Matsumoto, S.; McMurray, J.J.V.; Nasu, T.; Ishii, S.; Kagiyama, N.; Kida, K.; Fujimoto, W.; Kikuchi, A.; Ijichi, T.; Shibata, T.; et al. Relevant adverse events and drug discontinuation of sacubitril/valsartan in a real-world Japanese cohort: REVIEW-HF registry. Journal of cardiology., 2024,84(2), 133–140. [CrossRef]
- Galo, J.; Celli, D.; Colombo, R. Effect of Sacubitril/Valsartan on Neurocognitive Function: Current Status and Future Directions. American journal of cardiovascular drugs : drugs, devices, and other interventions., 2021,21(3), 267–270. [CrossRef]
- Watamura, N.; Kakiya, N.; Fujioka, R.; Kamano, N.; Takahashi, M.; Nilsson, P.; Saito, T.; Iwata, N.; Fujisawa, S.; Saido, T.C. The dopaminergic system promotes neprilysin-mediated degradation of amyloid-β in the brain. Science signaling., 2024,17(848), eadk1822. [CrossRef]
- Garnier-Crussard, A. Association between treatment with sacubitril/valsartan and the risk of Alzheimer's disease: a clinical update. Alzheimer's research & therapy., 2024,16(1), 177. [CrossRef]
- Morris, R.; Ali, R.; Cheng, F. Drug Repurposing Using FDA Adverse Event Reporting System (FAERS) Database. Current drug targets., 2024,25(7), 454–464. [CrossRef]
- Zhu, J.; Hu, M.; Liang, Y.; Zhong, M.; Chen, Z.; Wang, Z.; Yang, Y.; Luo, Z.; Zeng, W.; Li, J.; et al. Pharmacovigilance analysis of orlistat adverse events based on the FDA adverse event reporting system (FAERS) database. Heliyon., 2024,10(14), e34837. [CrossRef]
- Docherty, K.F.; Vaduganathan, M.; Solomon, S.D.; McMurray, J.J.V. Sacubitril/Valsartan: Neprilysin Inhibition 5 Years After PARADIGM-HF. JACC. Heart failure., 2020,8(10), 800–810. [CrossRef]
- Tian, Q.; Xiong, Z.; Fan, H.; Ning, T.; Zheng, Z. The Efficacy and Safety of Sacubitril-Valsartan for the Treatment of Heart Failure in Adults: A Meta-Analysis. The Annals of pharmacotherapy., 2023,57(4), 441–449. [CrossRef]
- Erdogan, B.R.; Yesilyurt-Dirican, Z.E.; Karaomerlioglu, I.; Muderrisoglu, A.E.; Sevim, K.; Michel, M.C.; Arioglu-Inan, E. Sacubitril/Valsartan Combination Partially Improves Cardiac Systolic, but Not Diastolic, Function through β-AR Responsiveness in a Rat Model of Type 2 Diabetes. Int J Mol Sci. 2024 Oct 2;25(19):10617. PMID: 39408945; PMCID: PMC11476658. [CrossRef]
- Kim, E.; Kim, H.; Jedrychowski, M.P.; Bakiasi, G.; Park, J.; Kruskop, J.; Choi, Y.; Kwak, S.S.; Quinti, L.; Kim, D.Y.; et al. Irisin reduces amyloid-β by inducing the release of neprilysin from astrocytes following downregulation of ERK-STAT3 signaling. Neuron., 2023,111(22), 3619–3633.e8. [CrossRef]
- Ali, N. H.; Al-Kuraishy, H. M. ; Al-Gareeb, A. I.; Alnaaim, S. A.; Alexiou, A.; Papadakis, M.; Khalifa, A.A; Saad, H.M; Batihaet, E.S. Neprilysin inhibitors and risk of Alzheimer's disease: A future perspective. Journal of cellular and molecular medicine., 2024,28(2), e17993. [CrossRef]
- Qian, C.; Yang, C.; Lu, M.; Bao, J.; Shen, H.; Deng, B.; Li, S.; Li, W.; Zhang, M.; Cao, C. Activating AhR alleviates cognitive deficits of Alzheimer's disease model mice by upregulating endogenous Aβ catabolic enzyme Neprilysin. Theranostics., 2021,11(18), 8797–8812. [CrossRef]
- Dargad, R.R.; Prajapati, M.R.; Dargad, R.R.; Parekh, J.D. Sacubitril/valsartan: A novel angiotensin receptor-neprilysin inhibitor. Indian heart journal., 2018,70 Suppl 1(Suppl 1), S102–S110. [CrossRef]
- He, Y.; Jin, Y.; Xue, H.; Liu, R.; Zhang, M.; Liao, R.; Chen, M.; Zhou, X.; He, X.; Qin, M.; et al. Pharmacokinetics and pharmacodynamics of sacubitril/valsartan in peritoneal dialysis patients. Nephrology, dialysis, transplantation : official publication of the European Dialysis and Transplant Association - European Renal Association., 2023,38(8), 1880–1889. [CrossRef]
- Langenickel, T.H.; Tsubouchi, C.; Ayalasomayajula, S.; Pal, P.; Valentin, M.A.; Hinder, M.; Jhee, S.; Gevorkyan, H.; Rajman, I. The effect of LCZ696 (sacubitril/valsartan) on amyloid-β concentrations in cerebrospinal fluid in healthy subjects. British journal of clinical pharmacology., 2016,81(5), 878–890. [CrossRef]
- Schoenfeld, H.A.; West, T.; Verghese, P.B.; Holubasch, M.; Shenoy, N.; Kagan, D.; Buono, C.; Zhou, W.; DeCristofaro, M.; Douville, J.; et al. The effect of angiotensin receptor neprilysin inhibitor, sacubitril/valsartan, on central nervous system amyloid-β concentrations and clearance in the cynomolgus monkey. Toxicology and applied pharmacology., 2017,323, 53–65. [CrossRef]
- Pena, O.Y.; Kyung, K. Drug-Induced Delirium Associated With Sacubitril/Valsartan in a Patient With Chronic Kidney Disease: A Case Report. Cureus., 2024,16(10), e72524. [CrossRef]
- Martins E Pereira, G. et al., Safety and tolerability of sacubitril-valsartan: a systematic review and meta-analysis. Expert opinion on drug safety., 2021,20(5), 577–588. [CrossRef]
- Dewan, P.; Shen, L.; Pedro Ferreira, J.; Jhund, P.S.; Anand, I.S.; Chandra, A.; Chiang, L.M.; Claggett, B.; Desai, A.S.; Gong, J.; et al. Effect of Sacubitril/Valsartan on Cognitive Function in Patients With Heart Failure With Preserved Ejection Fraction: A Prespecified Analysis of PARAGON-HF. Circulation., 2024,150(4), 272–282. [CrossRef]
- Hammadi, S.H.; Hassan, M.A.; Allam, E.A.; Elsharkawy, A.M.; Shams, S.S. Effect of sacubitril/valsartan on cognitive impairment in colchicine-induced Alzheimer's model in rats. Fundamental & clinical pharmacology., 2023,37(2), 275–286. [CrossRef]
- Pérez-Roselló, V.; Batalla-Monedero, M.; Sánchez-Lázaro, I.; López-Vilella, R.; Sierra-San Miguel, P.; Almenar-Bonet, L. Three cases of psychosis after use of sacubitril/valsartan. Revista espanola de cardiologia (English ed.)., 2021,74(1), 103–105. [CrossRef]
- Wooster, J.; Cook, E.A.; Shipman, D. Psychiatric Manifestations With Sacubitril/Valsartan: A Case Report. Journal of pharmacy practice., 2020,33(4), 553–557. [CrossRef]
Figure 1.
The number of Sacubitril/valsartan induced ADEs at the SOC level in FAERS database.
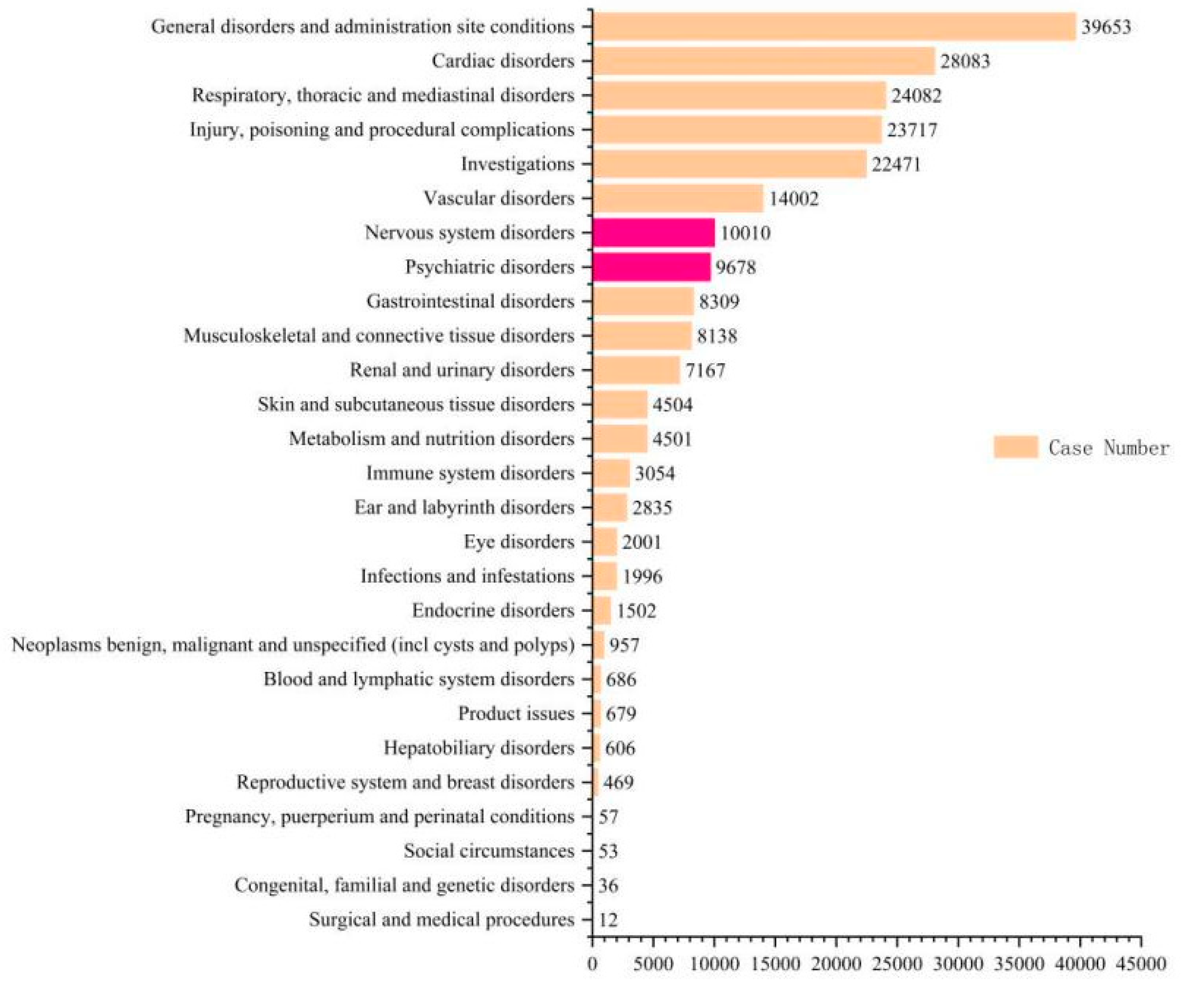

Table 1.
Summary of algorithms used for signal detection.
| Algorithms | Equation | Criteria |
| ROR | ROR =(a / c)/(b / d) 95%CI = eln.ROR±1.96(1/a+1/b+1/c+1/d)^0.5 |
a ≥ 3, lower limit of 95% CI > 1 |
| PRR | PRR = a(c + d)/c(a + b) χ2 = [(ad - bc)2](a + b + c + d)/[(a + b)(c + d)(a + c)(b + d)] |
a ≥ 3, PRR ≥ 2, χ2 ≥ 4 |
Table 2.
Features of adverse event reports associated with sacubitril/valsartan from Q3 2015 to Q4 2023.
Table 2.
Features of adverse event reports associated with sacubitril/valsartan from Q3 2015 to Q4 2023.
| Variables | Characteristics | Case number, n | Case proportion, % |
| Gender | Female | 29311 | 33.05 |
| Male | 53018 | 59.79 | |
| Unknown | 6346 | 7.16 | |
| Age (year) | <18 | 42 | 0.05 |
| 18-44 | 1270 | 1.43 | |
| 45-64 | 8071 | 9.1 | |
| ≥65 | 12907 | 14.56 | |
| Unknown | 66385 | 74.86 | |
| Outcome of ADEs | Unknown | 48229 | 54.39 |
| Other | 16534 | 18.65 | |
| Death | 12747 | 14.37 | |
| Hospitalization - Initial or Prolonged | 9742 | 10.99 | |
| Life-Threatening | 1051 | 1.19 | |
| Disability | 363 | 0.41 | |
| Required Intervention to Prevent Permanent Impairment | 7 | 0.01 | |
| Congenital Anomaly | 2 | 0 | |
| Reported Countries | United States | 46045 | 51.93 |
| Japan | 1640 | 1.85 | |
| India | 1468 | 1.66 | |
| Philippines | 981 | 1.11 | |
| Germany | 802 | 0.9 | |
| France | 579 | 0.65 | |
| China | 531 | 0.6 | |
| Brazil | 517 | 0.58 | |
| Other | 4840 | 5.46 | |
| Country Not Specified | 31272 | 35.27 | |
| Reported years | 2023 | 12043 | 13.58 |
| 2022 | 19189 | 21.64 | |
| 2021 | 14268 | 16.09 | |
| 2020 | 8678 | 9.79 | |
| 2019 | 11979 | 13.51 | |
| 2018 | 10842 | 12.23 | |
| 2017 | 6465 | 7.29 | |
| 2016 | 4574 | 5.16 | |
| 2015 | 637 | 0.72 |
Table 3.
Signals for the top 50 adverse events associated with Sacubitril/valsartan use by number of reported cases (Calculated by By frequency).
Table 3.
Signals for the top 50 adverse events associated with Sacubitril/valsartan use by number of reported cases (Calculated by By frequency).
| PT | N | ROR(95%CI) | PRR(X2) |
| Hypotension | 8609 | 15.94(16.32-15.56) | 14.49(4173449.39) |
| Death | 8377 | 2.26(2.31-2.20) | 2.14(30080690.27) |
| Wrong technique in product usage process | 6577 | 5.79(5.94-5.65) | 5.44(9243891.4) |
| Dizziness | 6349 | 3.94(4.05-3.84) | 3.73(13168883.04) |
| Dyspnoea | 6277 | 3.60(3.70-3.51) | 3.42(14234157.38) |
| Cough | 6223 | 7.21(7.41-7.02) | 6.78(6943847.31) |
| Fatigue | 6139 | 2.23(2.28-2.17) | 2.14(22277132.74) |
| Weight decreased | 3861 | 4.56(4.72-4.42) | 4.41(6789523.83) |
| Malaise | 3485 | 2.08(2.15-2.01) | 2.04(13487983.1) |
| Cardiac failure | 2865 | 11.66(12.12-11.21) | 11.31(1840646.56) |
| Asthenia | 2587 | 2.25(2.34-2.16) | 2.21(9259604.37) |
| Weight increased | 2575 | 3.59(3.74-3.45) | 3.52(5737334.15) |
| Myocardial infarction | 2466 | 7.21(7.51-6.91) | 7.03(2658752.04) |
| Blood pressure decreased | 2256 | 12.62(13.19-12.07) | 12.32(1318323.16) |
| Inappropriate schedule of product administration | 2248 | 3.03(3.16-2.90) | 2.98(5953164.97) |
| Hypoacusis | 2120 | 9.95(10.41-9.51) | 9.74(1608134.65) |
| Feeling abnormal | 2060 | 2.27(2.37-2.17) | 2.24(7297335.07) |
| Cardiac disorder | 1924 | 6.31(6.62-6.03) | 6.2(2375626.01) |
| Memory impairment | 1807 | 3.39(3.56-3.24) | 3.34(4253697.31) |
| Hypertension | 1795 | 2.76(2.89-2.63) | 2.72(5218151.4) |
| Ejection fraction decreased | 1730 | 45.46(48.17-42.9) | 44.59(211321.34) |
| Fluid retention | 1673 | 10.00(10.53-9.51) | 9.83(1256056.74) |
| Peripheral swelling | 1562 | 2.42(2.55-2.30) | 2.39(5181575.16) |
| Prescribed underdose | 1516 | 17.21(18.19-16.29) | 16.94(616643.97) |
| Cerebrovascular accident | 1473 | 3.04(3.20-2.89) | 3.01(3872691.21) |
| Chest pain | 1367 | 2.69(2.84-2.55) | 2.66(4072939.37) |
| Nasopharyngitis | 1363 | 2.21(2.34-2.10) | 2.19(4947533.12) |
| Throat clearing | 1328 | 146.52(159.82-134.34) | 144.35(28130.31) |
| Atrial fibrillation | 1272 | 4.11(4.35-3.89) | 4.07(2448626.26) |
| Illness | 1099 | 2.54(2.70-2.39) | 2.52(3465002.82) |
| Blood potassium increased | 1021 | 25.62(27.47-23.89) | 25.34(257076.92) |
| Cardiac failure congestive | 980 | 6.73(7.18-6.31) | 6.67(1121437.23) |
| Diabetes mellitus | 947 | 3.98(4.24-3.72) | 3.94(1883814.82) |
| Renal impairment | 935 | 2.86(3.05-2.68) | 2.84(2610776.82) |
| Weight fluctuation | 890 | 31.18(33.65-28.89) | 30.88(175269.93) |
| Cardiac arrest | 868 | 3.88(4.16-3.63) | 3.86(1768420.9) |
| Heart rate increased | 844 | 2.81(3.01-2.62) | 2.79(2398489.81) |
| Renal disorder | 821 | 4.60(4.93-4.29) | 4.56(1402732.06) |
| Underdose | 792 | 2.34(2.51-2.18) | 2.33(2715268.83) |
| Product prescribing error | 790 | 6.56(7.06-6.11) | 6.51(926968.3) |
| Heart rate decreased | 769 | 6.81(7.33-6.33) | 6.76(866916.76) |
| Blood creatinine increased | 753 | 3.95(4.25-3.67) | 3.93(1505041.68) |
| Swelling | 743 | 2.23(2.40-2.07) | 2.22(2676216.69) |
| Dehydration | 724 | 2.03(2.19-1.89) | 2.02(2864971.08) |
| Syncope | 670 | 2.08(2.24-1.92) | 2.07(2588998.16) |
| Stress | 630 | 2.68(2.90-2.47) | 2.67(1880648.6) |
| Rhinorrhoea | 621 | 2.69(2.92-2.49) | 2.68(1843046.36) |
| Pollakiuria | 594 | 4.42(4.80-4.07) | 4.4(1055264.21) |
| Pulmonary oedema | 562 | 4.37(4.76-4.01) | 4.35(1011052.68) |
| Hyperkalaemia | 547 | 5.05(5.50-4.63) | 5.02(846078.03) |
Table 4.
fundamental characteristics of nervous system disorders and psychiatric disorders ADEs induced by Sacubitril/Valsartan.
Table 4.
fundamental characteristics of nervous system disorders and psychiatric disorders ADEs induced by Sacubitril/Valsartan.
| Variables | Characteristics | Number of cases of psychoneurotic symptoms | Case proportion, % |
| Gender | Female | 7533 | 38.26 |
| Male | 11580 | 58.82 | |
| Unknown | 575 | 2.92 | |
| <18 | 0 | 0 | |
| Age (year) | 18-44 | 289 | 1.47 |
| 45-64 | 2323 | 11.8 | |
| ≥65 | 2831 | 14.38 | |
| Unknown | 14245 | 72.35 | |
| Outcome of ADEs | Unknown | 7268 | 36.92 |
| Other | 7891 | 40.08 | |
| Death | 708 | 3.6 | |
| Hospitalization - Initial or Prolonged | 2961 | 15.04 | |
| Life-Threatening | 698 | 3.55 | |
| Disability | 159 | 0.81 | |
| Required Intervention to Prevent Permanent Impairment | 3 | 0.02 | |
| Congenital Anomaly | 0 | 0 | |
| Reported Countries | United States | 12379 | 62.88 |
| Japan | 130 | 0.66 | |
| India | 51 | 0.26 | |
| Philippines | 127 | 0.65 | |
| Germany | 156 | 0.79 | |
| France | 67 | 0.34 | |
| China | 29 | 0.15 | |
| Brazil | 203 | 1.03 | |
| Other | 997 | 5.06 | |
| Country Not Specified | 5549 | 28.18 | |
| Reported years | 2023 | 3735 | 18.97 |
| 2022 | 5329 | 27.07 | |
| 2021 | 3564 | 18.1 | |
| 2020 | 1949 | 9.9 | |
| 2019 | 2282 | 11.59 | |
| 2018 | 1568 | 7.96 | |
| 2017 | 857 | 4.35 | |
| 2016 | 375 | 1.9 | |
| 2015 | 29 | 0.15 |
Table 5.
Distribution of PT for Adverse Events of neuropsychiatric symptoms.
| SOC | PT | N | ROR(95%CI) | PRR(X2) |
| Psychiatric disorders | Memory impairment | 1807 | 3.39(3.56-3.24) | 2.43(1642487.56) |
| Stress | 630 | 2.68(2.9-2.47) | 2.28(376033.75) | |
| Amnesia | 501 | 2.44(2.67-2.23) | 2.73(11607.78) | |
| Fear | 145 | 2.19(2.58-1.86) | 4.19(26138.87) | |
| Dementia Alzheimer's type | 114 | 3.2(3.86-2.66) | 3.08(23126.67) | |
| Aphonia | 107 | 2.28(2.76-1.88) | 2.87(55401.95) | |
| Frustration tolerance decreased | 91 | 2.14(2.63-1.74) | 3.12(50875.05) | |
| Laziness | 41 | 6.27(8.61-4.57) | 2.36(23662.9) | |
| Reading disorder | 31 | 3.54(5.06-2.47) | 3.01(3872691.21) | |
| Daydreaming | 21 | 3.38(5.22-2.18) | 5.94(5096.26) | |
| Fear of death | 21 | 3.76(5.82-2.43) | 3.21(24579.45) | |
| Claustrophobia | 10 | 3.21(6.04-1.71) | 3.1(10159.23) | |
| Fear of disease | 9 | 2.11(4.09-1.09) | 3.38(49159.47) | |
| Impaired reasoning | 6 | 4.03(9.13-1.78) | 3.14(921322.65) | |
| Grief reaction | 5 | 2.78(6.77-1.14) | 3.2(282309.69) | |
| Boredom | 4 | 2.73(7.37-1.01) | 2.71(196796.7) | |
| Confabulation | 4 | 3.1(8.4-1.14) | 2.98(45249.93) | |
| Fear of surgery | 3 | 54.39(227.61-13) | 2.19(530848.65) | |
| Fear-related avoidance of activities | 3 | 3.24(10.24-1.02) | 3.76(43910.47) | |
| Nervous system disorders | Cerebrovascular accident | 1473 | 3.04(3.2-2.89) | 2.11(34085.16) |
| Speech disorder | 385 | 2.27(2.52-2.06) | 54.39(225.54) | |
| Dementia | 365 | 3.15(3.5-2.84) | 3.24(7258.02) | |
| Orthostatic hypotension | 188 | 3.25(3.76-2.81) | 2.14(341513.26) | |
| Hypokinesia | 161 | 3.03(3.55-2.59) | 7.55(2922.91) | |
| Near death experience | 96 | 5.97(7.34-4.85) | 2.78(14237.54) | |
| Dysgraphia | 67 | 2.71(3.46-2.13) | 3.03(422255.64) | |
| Carotid artery occlusion | 20 | 2.87(4.48-1.84) | 4.03(11617.85) | |
| Carotid artery stenosis | 20 | 3.12(4.87-1.99) | 3.36(6986.54) | |
| Dyslexia | 17 | 2.98(4.83-1.84) | 6.27(50113.71) | |
| Brain hypoxia | 14 | 4.19(7.16-2.45) | 3.34(4253697.31) | |
| Carotid artery disease | 9 | 3.08(5.98-1.58) | 5.96(123897.14) | |
| Cerebral palsy | 7 | 2.36(5-1.11) | 2.63(21126.97) | |
| Orthostatic hypertension | 7 | 2.63(5.58-1.24) | 3.24(458990.28) | |
| Cerebrovascular insufficiency | 4 | 5.94(16.35-2.16) | 3.53(69208.04) | |
| Visual brightness | 4 | 3.49(9.47-1.28) | 2.27(1356844.21) | |
| Fumbling | 3 | 7.55(24.53-2.33) | 2.67(1880648.6) | |
| Irregular sleep phase | 3 | 3.36(10.63-1.06) | 3.49(8982.67) |
Table 6.
Signal Analysis of Fatal Events within neuropsychiatric symptoms Adverse Events.
| PT | ROR(95%CI) | PRR(X2) | total number of deaths | Total number of reports | % |
| Irregular sleep phase | 3.36(10.63-1.06) | 3.49(8982.67) | 1 | 3 | 33.33 |
| Cerebrovascular insufficiency | 5.94(16.35-2.16) | 3.53(69208.04) | 1 | 4 | 25.00 |
| Impaired reasoning | 4.03(9.13-1.78) | 3.14(921322.65) | 1 | 6 | 16.67 |
| Carotid artery stenosis | 3.12(4.87-1.99) | 3.36(6986.54) | 3 | 20 | 15.00 |
| Orthostatic hypertension | 2.63(5.58-1.24) | 3.24(458990.28) | 1 | 7 | 14.29 |
| Cerebrovascular accident | 3.04(3.20-2.89) | 2.11(34085.16) | 123 | 1473 | 8.35 |
| Dementia Alzheimer's type | 3.20(3.86-2.66) | 3.08(23126.67) | 7 | 114 | 6.14 |
| Dementia | 3.15(3.50-2.84) | 3.24(7258.02) | 22 | 365 | 6.03 |
| Hypokinesia | 3.03(3.55-2.59) | 7.55(2922.91) | 9 | 161 | 5.59 |
| Orthostatic hypotension | 3.25(3.76-2.81) | 2.14(341513.26) | 8 | 188 | 4.26 |
| Speech disorder | 2.27(2.52-2.06) | 54.39(225.54) | 14 | 385 | 3.64 |
| Stress | 2.68(2.90-2.47) | 2.28(376033.75) | 18 | 630 | 2.86 |
| Aphonia | 2.28(2.76-1.88) | 2.87(55401.95) | 3 | 107 | 2.80 |
| Dysgraphia | 2.71(3.46-2.13) | 3.03(422255.64) | 1 | 67 | 1.49 |
| Fear | 2.19(2.58-1.86) | 4.19(26138.87) | 1 | 145 | 0.69 |
| Amnesia | 2.44(2.67-2.23) | 2.73(11607.78) | 3 | 501 | 0.60 |
| Memory impairment | 3.39(3.56-3.24) | 2.43(1642487.56) | 10 | 1807 | 0.55 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



