
Submitted:
08 January 2025
Posted:
09 January 2025
You are already at the latest version
Abstract
Objectives: The aim of this study was to investigate the incidence and severity of oral adverse events in outpatients receiving cancer drug therapy and the need for intervention by dental professionals. Methods: A questionnaire-based survey was conducted among patients who received cancer drug therapy at our hospital between September 1 and 30, 2022. The incidence and severity of oral adverse events and the need for intervention by dental professionals were investigated. The risk factors for these events were also analyzed. Results: Of the 216 patients who answered the questionnaire, 127 (58.8%) experienced oral adverse events such as dysgeusia, oral mucositis, and xerostomia. Of the patients who experienced oral adverse events, 53.5% showed that they wanted to improve their condition, 34.6% showed that the adverse events caused problems in their daily lives, and 26.8% wanted dental intervention. Thirty-two patients (25.2%) reported that the symptoms of these oral events were as severe as or more severe than those of other adverse events. The incidence of adverse oral events was significantly higher in patients treated with 5FU- and taxane-based regimens than in patients treated with other regimens. Conclusions: Our results suggest that oral adverse events have a significant impact on outpatients receiving cancer drug therapy. More than a quarter of outpatients receiving cancer drug therapy wanted oral management through dental interventions. In particular, patients receiving 5FU-, taxane-, and anthracycline-based regimens may require oral management by dental professionals.
Keywords:
outpatient
; cancer drug therapy
; oral adverse events
; oral management
1. Introduction
Oral adverse events during cancer drug therapy not only cause severe pain, difficulty eating, loss of taste, and impaired speech but may also affect the daily lives of patients [1]. Several scientific societies have developed guidelines for the oral management of patients receiving cancer treatment [1,2,3,4]. The Multinational Association of Supportive Care in Cancer/International Society of Oral Oncology (MASCC/ISOO) emphasize the importance of appropriate oral management by multidisciplinary medical teams involving well-trained dentists or dental hygienists to prevent and treat oral adverse events [3,4]. Oral management is generally performed by multidisciplinary teams in patients receiving bone marrow transplantation and head and neck radiotherapy because the incidence of oral adverse events observed during these treatments is high [5,6,7]. However, outpatients receiving cancer drug therapy do not undergo oral management because the incidence of oral adverse events is considered low [1]. Therefore, outpatients receiving cancer drug therapy may not receive appropriate oral management. However, outpatients receiving cancer drug therapy may be at a higher risk of adverse oral events than expected because high-intensity treatments are increasingly being administered on an outpatient basis [8,9].
The aim of this study was to clarify the frequency and severity of oral adverse events in outpatients receiving cancer drug therapy and to clarify patient needs for the management of oral adverse events by medical professionals.
2. Materials and Methods
2.1. Patients
This cross-sectional survey was conducted at the Outpatient Cancer Chemotherapy Center of Niigata University Medical and Dental Hospital from September 1st to 30th, 2022. Patients 1) with cancer, 2) who were receiving cancer drug therapy at the Outpatient Cancer Chemotherapy Center, and 3) who were over 18 years of age, were eligible for inclusion. Patients 1) who did not agree to participate in the study, 2) who were receiving or had received radiation therapy, and 3) who were receiving oral care from dental professionals such as dentists or dental hygienists, were excluded. This study was approved by the Ethics Committee of the Niigata University School of Medicine (approval number: 2022-0120).
2.2. Data Collection and Survey
This survey was conducted using a questionnaire designed with reference to the Patient-Reported Outcome (PRO) Common Terminology Criteria for Adverse Events (PRO-CTCAE) (Table 1) [10,11]. Data on the incidence and severity of oral adverse events, the need for oral adverse event management by dental professionals, and the impact of these events on daily life were collected and evaluated.
2.3. Statistical Analysis
The sample size was not set because this was a cross-sectional study. The relationship between patient characteristics and major oral adverse events was analyzed using EZR ver.1.66 (Saitama Medical Center, Jichi Medical University, Saitama, Japan) [12], which is a graphical user interface for R (The R Foundation for Statistical Computing, Vienna, Austria). It is a modified version of the R commander designed to add statistical functions frequently used in biostatistics. Uni- and multivariate logistic regression analyses were used to identify the predictors of major oral adverse events. P<0.05 was considered statistically significant.
3. Results
Two hundred and sixteen patients were enrolled in this study. The patient characteristics are shown in Table 2.
More than half of the patients were middle-aged (aged 40–69 years). The major cancer types were breast, lung, and gastrointestinal cancers. Patients had received the following cancer drug therapies: immune checkpoint inhibitors (ICIs), taxane-based regimens, 5-fluorouracil-based regimens (5-FU), anthracycline-based regimens, cisplatin (CDDP)-based regimens, and monoclonal antibody drugs targeting epidermal growth factor receptor (EGFR). The most commonly used drug therapies were ICIs, and taxane- and 5FU-based regimens (31.0, 22.7, and 15.3%, respectively).
3.1. Incidence of Oral Adverse Events
One hundred and twenty-seven patients (58.8%) experienced adverse oral events (Table 3-1). These included dysgeusia, oral mucositis, xerostomia, tongue coating, stickiness, oral discomfort, oral pain, and numbness around the mouth (Figure 1). The most prevalent oral adverse events were dysgeusia, oral mucositis, and xerostomia, with incidence rates of 25.9, 21.3, and 19.4%, respectively (Table 3-2).
3.2. Patient Needs for Management of Oral Adverse Events by Medical Professionals
Sixty-eight patients (53.5%) wanted improvement of their oral adverse events. Furthermore, 44 patients (34.6%) had oral adverse events that affected their daily lives, and 34 patients (26.8%) wanted professional oral care from well-trained dentists and dental hygienists. Thirty-two patients (25.2%) experienced oral adverse events that were as severe or even more severe than other adverse events (Table 4).
3.3. The Relationship Between Patient Characteristics and Major Oral Adverse Events
The relationship between oral adverse events and patient characteristics is shown in Table 3-1. Dysgeusia, oral mucositis, and xerostomia were the major oral symptoms (Table 3-2).
Patients with breast cancer experienced significantly more oral adverse events than other patients (OR=6.38; 95%CI=1.05–38.90; P=0.04). Patients receiving 5FU- and taxane-based regimens had significantly more oral adverse events than those receiving other regimens (OR=9.37; 95%CI=1.74–50.40; P<0.01 and OR=5.63; 95%CI=1.91–16.60; P<0.01, respectively). The incidence of oral mucositis did not differ significantly between any of the regimens. Dysgeusia was significantly higher in taxane-based regimens than in the other regimens (OR=4.76; 95%CI=1.61–14.10; P<0.01). The incidence of xerostomia was significantly higher in 5FU-based regimens than in the other regimens (OR=16.5; 95%CI=1.74–157.00; P=0.01).
4. Discussion
The objective of this study was to clarify the frequency and severity of oral adverse events in outpatients receiving cancer drug therapy and to clarify patients’ needs for oral adverse event management by dental professionals. Our findings have several important clinical implications. First, more than half of the outpatients receiving cancer drug therapy had oral adverse events. Second, more than a quarter of the patients who experienced oral adverse events felt that these symptoms were as severe or even more severe than other non-oral adverse events. Third, more than a quarter of the patients who experienced oral adverse events wanted oral management through professional intervention by well-trained dentists and dental hygienists. These results indicate that oral adverse events have a significant negative impact on patients receiving outpatient cancer drug therapy.
The guidelines for supportive care in cancer have described the importance of interventions by multidisciplinary medical teams involving well-trained dentists and dental hygienists to manage oral adverse events [3,4,13]. The guidelines indicate that professional dental intervention is essential for patients at high risk of oral adverse events, such as those undergoing bone marrow transplantation and head and neck radiotherapy. Conversely, outpatient chemotherapy is currently associated with a low risk of adverse oral events. However, our results suggest that adverse oral events also have a significant impact on outpatients receiving cancer drug therapies, highlighting their need for oral management by dental professionals.
Our results showed that taxane-based regimens had the highest incidence of dysgeusia. Taxane-based drug therapies affect neurosensory perception [14]. Therefore, the cause of the dysgeusia was considered to be neuropathy due to taxane-based drug therapies. Prolonged dysgeusia not only worsens nutritional and performance status but may also make it difficult to continue cancer therapy [15,16,17,18]. Therefore, outpatients receiving taxane-based regimens should be aware of the risk of developing dysgeusia due to neuropathy.
According to the 2020 edition of the guidelines for managing mucositis during cancer drug therapy, anticancer drugs such as anthracycline-based, 5FU-based, and methotrexate regimens are associated with a higher incidence of oral mucositis [1]. Our results showed no significant differences in the incidence of oral mucositis among the cancer drug therapies. However, the incidence of oral mucositis was >25% for all regimens, excluding ICIs. Oral mucositis increases the risk of systemic complications, such as malnutrition, cachexia, and systemic infections [19,20]. Furthermore, oral mucositis negatively affects treatment outcomes and medical costs [21]. Therefore, the incidence of oral mucositis should be considered even in outpatient settings.
Our study showed the highest incidence of xerostomia when 5FU-based regimens were used. A previous study reported that patients receiving cyclophosphamide, epirubicin, methotrexate and 5FU experienced a higher incidence of xerostomia [22]. 5FU-based regimens are widely used to treat many solid tumors. They are also used in outpatient chemotherapy. Xerostomia can cause oral discomfort and functional impairment [23]. It results in a reduction in the physiological effects of saliva, including antibacterial activity, mucosal protection, and assistance with taste. Therefore, xerostomia may exacerbate dysgeusia and oral mucositis [24,25,26].
Our results showed that more than a quarter of the patients who experienced oral adverse events wanted oral interventions by dental professionals. These results show that outpatients receiving cancer drug therapy also require appropriate oral management by a multidisciplinary medical team. However, the number of outpatients receiving cancer drug therapy is very high. Therefore, an efficient patient selection system would be essential [27].
Our study has several limitations. First, the results were based on subjective patient-reported questionnaire surveys and did not reflect evaluations by medical professionals. Discrepancies may occur between patient and medical professional evaluations [28,29,30]. Thus, patient and medical professional assessments should be considered in future studies. Second, because the survey in this study was based on patient-reported questionnaires, the communication abilities of the patients and the absence of opinions from non-responders may have influenced the results. Third, although drug therapies containing anthracyclines or anti-EGFR antibodies are associated with a higher incidence of oral mucositis, only a limited number of patients were included in this study. Thus, assessment of the necessity for professional medical intervention in outpatients treated with these drug therapies was difficult. We performed multivariate analysis to reduce these biases. Fourth, because the survey was conducted at a single hospital, there was a potential bias in patient background and cancer drug therapy, leading to possible discrepancies. We plan to focus on 5FU-, taxane-, and anthracycline-based regimens and use more established adverse event assessment methods, such as PRO-CTCAE, for validation in future studies. Finally, our study had a cross-sectional design; therefore, the sample size was small. However, to maximize the number of participants, we requested consent from all eligible individuals.
5. Conclusions
Our results suggest that oral adverse events negatively affect the daily lives of outpatients receiving cancer drug therapy. More than a quarter of outpatients receiving cancer drug therapy wanted oral management through dental interventions. In particular, patients receiving 5FU-, taxane-, and anthracycline-based regimens may require oral management by dental professionals.
Future studies should introduce evaluation methods based on PRO-CTCAE and CTCAE and collect data from a diverse patient population through multicenter collaborative studies. Furthermore, the adoption of a longitudinal study design will facilitate investigation of the time course of oral adverse events and the impact of appropriate oral care on quality of life and treatment continuity. This is expected to lead to more effective and practical interventions and improved quality of care.
Author Contributions
Conceptualization Y.S. and K.K.; Data Collection Y.S. and M.K.; Formal analysis and investigation, Y.S.; Writing original draft preparation: Y.S., K.K., A.T. All authors critically revised the article and approved the final version for publication.
Funding
This research received no external funding.
Institutional Review Board Statement
The survey was conducted among patients who provided voluntary consent. This study was conducted in compliance with the “Ethical Guidelines for Medical Research Involving Human Subjects” and was approved by the Ethics Committee of Niigata University School of Medicine (approval number: 2022-0120). The purpose of the research was posted to the Outpatient Cancer Drug Therapy Center and confidentiality was ensured. Informed consent was obtained from all participants after they returned the completed questionnaire.
Informed Consent Statement
Not applicable.
Data Availability Statement
The datasets used and/or analyzed in the current study are available from the corresponding author upon reasonable request.
Acknowledgments
We would like to thank Editage (www.editage.jp) for the English language editing.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MASCC | Multinational association of supportive care in cancer |
| ISOO | International society of oral oncology |
| PRO-CTCAE | Patient-Reported Outcome Common Terminology Criteria for Adverse Events |
| 5-FU | 5-fluorouracil |
| ICIs | Immune checkpoint inhibitors |
| CDDP | Cisplatin |
| EGFR | Epidermal growth factor receptor |
References
- Japanese Association of Supportive Care in Cancer, Japanese Association of Oral Supportive Care in Cancer: Clinical Guidance of Management for Mucositis; Kanehara Co., Ltd.: Tokyo, 2020.
- Nagasueshoten, K. Japanese Society for Transplantation and Cellular Therapy, Japanese Association of Oral Supportive Care in Cancer: Guidelines for the Oral Management of Hematopoietic Cell Transplant Patients. 1st ed, 2022(in Japanese).
- Elad, S.; Cheng, K.K.F.; Lalla, R.V.; Yarom, N.; Hong, C.; Logan, R.M.; Bowen, J.; Gibson, R.; Saunders, D.P.; Zadik, Y.; et al. MASCC/ISOO clinical practice guidelines for the management of mucositis secondary to cancer therapy. Cancer 2020, 126, 4423–4431. [CrossRef]
- Mercadante, V.; Jensen, S.B.; Smith, D.K.; Bohlke, K.; Bauman, J.; Brennan, M.T.; Coppes, R.P.; Jessen, N.; Malhotra, N.K.; Murphy, B.; et al. Salivary Gland Hypofunction and/or xerostomia Induced by Nonsurgical Cancer Therapies: ISOO/MASCC/ASCO Guideline [ISOO/MASCC/ASCO guideline]. J Clin Oncol 2021, 39, 2825–2843. [CrossRef]
- Soga, Y.; Sugiura, Y.; Takahashi, K.; Nishimoto, H.; Maeda, Y.; Tanimoto, M.; Takashiba, S. Progress of oral care and reduction of oral mucositis-a pilot study in hematopoietic stem cell transplantation ward. Support Care Cancer 2011, 19, 303–307. [CrossRef]
- Yamagata, K.; Arai, C.; Sasaki, H.; Takeuchi, Y.; Onizawa, K.; Yanagawa, T.; Ishibashi, N.; Karube, R.; Shinozuka, K.; Hasegawa, Y.; et al. The effect of oral management on the severity of oral mucositis during hematopoietic SCT. Bone Marrow Transplant 2012, 47, 725–730. [CrossRef]
- Yoshida, K.; Kodama, Y.; Tanaka, Y.; Pak, K.; Soga, M.; Toyama, A.; Katsura, K.; Takagi, R. Pharmacist involved education program in a multidisciplinary team for oral mucositis: Its impact in head-and-neck cancer patients. PLOS ONE 2021, 16, e0260026. [CrossRef]
- Çakmak, S.; Nural, N. Incidence of and risk factors for development of oral mucositis in outpatients undergoing cancer chemotherapy. Int J Nurs Pract 2019, 25, e12710. [CrossRef]
- Wilberg, P.; Hjermstad, M.J.; Ottesen, S.; Herlofson, B.B. Chemotherapy-associated oral sequelae in patients with cancers outside the head and neck region. J Pain Symptom Manage 2014, 48, 1060–1069. [CrossRef]
- US Department of Health and Human Services. Guidance for industry. Patient-reported outcome measures: Use in medical product development to support labeling claims, 2009. Available online: http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM193282.pdf (accessed on 5 Jun 2022).
- Japan Clinical Oncology Group. NCI- PRO-CTCAE® ITEMS-Japanese Item Library. version 1.0. Available online: http://healthcaredelivery.cancer.gov/pro-ctcae/instruments/pro-ctcae/pro-ctcaeJapanese.pdf (accessed on 5 Jun 2022).
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant 2013, 48, 452–458 [Advance online publication 3 Dec 2012]. [CrossRef]
- Brown, T.J.; Gupta, A. Management of cancer therapy–associated oral mucositis: JCO. J Oncol Pract 2020, 16, 103–109.
- Jones, S.E.; Erban, J.; Overmoyer, B.; Budd, G.T.; Hutchins, L.; Lower, E.; Laufman, L.; Sundaram, S.; Urba, W.J.; Pritchard, K.I.; et al. Randomized Phase III Study of Docetaxel Compared With Paclitaxel in Metastatic Breast Cancer. J Clin Oncol 2005, 23, 5542–5551. [CrossRef]
- Holmes, S. Food avoidance in patients undergoing cancer chemotherapy. Support Care Cancer 1993, 1, 326–330. [CrossRef]
- Amézaga, J.; Alfaro, B.; Ríos, Y.; Larraioz, A.; Ugartemendia, G.; Urruticoechea, A.; Tueros, I. Assessing taste and smell alterations in cancer patients undergoing chemotherapy according to treatment. Support Care Cancer 2018, 26, 4077–4086. [CrossRef]
- Speck, R.M.; DeMichele, A.; Farrar, J.T.; Hennessy, S.; Mao, J.J.; Stineman, M.G.; Barg, F.K. Taste alteration in breast cancer patients treated with taxane chemotherapy: Experience, effect, and coping strategies. Support Care Cancer 2013, 21, 549–555. [CrossRef]
- Steinbach, S.; Hummel, T.; Böhner, C.; Berktold, S.; Hundt, W.; Kriner, M.; Heinrich, P.; Sommer, H.; Hanusch, C.; Prechtl, A.; et al. Qualitative and quantitative assessment of taste and smell changes in patients undergoing chemotherapy for breast cancer or gynecologic malignancies. J Clin Oncol 2009, 27, 1899–1905. [CrossRef]
- Peterson, D.E.; Minah, G.E.; Overholser, C.D.; Suzuki, J.B.; Depaola, L.G.; Stansbury, D.M.; Williams, L.T.; Schimpff, S.C. Microbiology of acute periodontal infection in myelosuppressed cancer patients. J Clin Oncol 1987, 5, 1461–1468. [CrossRef]
- Raber-Durlacher, J.E.; Epstein, J.B.; Raber, J.; van Dissel, J.T.; van Winkelhoff, A.J.; Guiot, H.F.L.; van der Velden, U. Periodontal infection in cancer patients treated with high-dose chemotherapy. Support Care Cancer 2002, 10, 466–473. [CrossRef]
- Lalla, R.V.; Sonis, S.T.; Peterson, D.E. Management of oral mucositis in patients who have cancer. Dent Clin North Am 2008, 52, 61–77. [CrossRef]
- Jensen, S.B.; Mouridsen, H.T.; Reibel, J.; Brünner, N.; Nauntofte, B. Adjuvant chemotherapy in breast cancer patients induces temporary salivary gland hypofunction. Oral Oncol 2008, 44, 162–173. [CrossRef]
- Katura, K. Manual for Xerostomia Management in Cancer Treatment; Foundation for Promotion of Cancer Research: Tokyo, 2019(in Japanese).
- Vissink, A.; Schaub, R.M.; van Rijn, L.J.; Gravenmade, E.J.; Panders, A.K.; Vermey, A. The efficacy of mucin-containing artificial saliva in alleviating symptoms of xerostomia. Gerodontology 1987, 6, 95–101. [CrossRef]
- Vissink, A.; Jansma, J.; Spijkervet, F.K.; Burlage, F.R.; Coppes, R.P. Oral sequelae of head and neck radiotherapy. Crit Rev Oral Biol Med 2003, 14, 199–212. [CrossRef]
- Jensen, S.B.; Pedersen, A.M.L.; Vissink, A.; Andersen, E.; Brown, C.G.; Davies, A.N.; Dutilh, J.; Fulton, J.S.; Jankovic, L.; Lopes, N.N.; et al. A systematic review of salivary gland hypofunction and xerostomia induced by cancer therapies: Prevalence, severity and impact on quality of life. Support Care Cancer 2010, 18, 1039–1060. [CrossRef]
- Honma, T.; Denpoya, A.; Narui, H. Team medical care for cancer outpatients on anticancer medication therapy: Reality and challenges. Aomori J Health Welf 2021, 3, 10–19.
- Filho, O.M.; Giobbie-Hurder, A.; Lin, N.U.; Faggen, M.; Come, S.; Openshaw, T.; Constantine, M.; Walsh, J.; Freedman, R.A.; Schneider, B.; et al. A dynamic portrait of adverse events for breast cancer patients: Results from a phase II clinical trial of eribulin in advanced HER2-negative breast cancer. Breast Cancer Res Treat 2021, 185, 135–144. [CrossRef]
- Atkinson, T.M.; Ryan, S.J.; Bennett, A.V.; Stover, A.M.; Saracino, R.M.; Rogak, L.J.; Jewell, S.T.; Matsoukas, K.; Li, Y.; Basch, E. The association between Clinician-Based Common Terminology Criteria for Adverse Events (CTCAE) and Patient-Reported Outcomes (PRO): A Systematic Review. Support Care Cancer 2016, 24, 3669–3676. [CrossRef]
- Falchook, A.D.; Green, R.; Knowles, M.E.; Amdur, R.J.; Mendenhall, W.; Hayes, D.N.; Grilley-Olson, J.E.; Weiss, J.; Reeve, B.B.; Mitchell, S.A.; et al. Comparison of Patient- and Practitioner-Reported Toxic Effects associated with chemoradiotherapy for head and neck cancer. JAMA Otolaryngol Head Neck Surg 2016, 142, 517–523. [CrossRef]
Figure 1.
Details of the adverse events. This figure shows the number of patients with oral adverse events, as determined using the questionnaire. The survey allowed for multiple answers.
Figure 1.
Details of the adverse events. This figure shows the number of patients with oral adverse events, as determined using the questionnaire. The survey allowed for multiple answers.
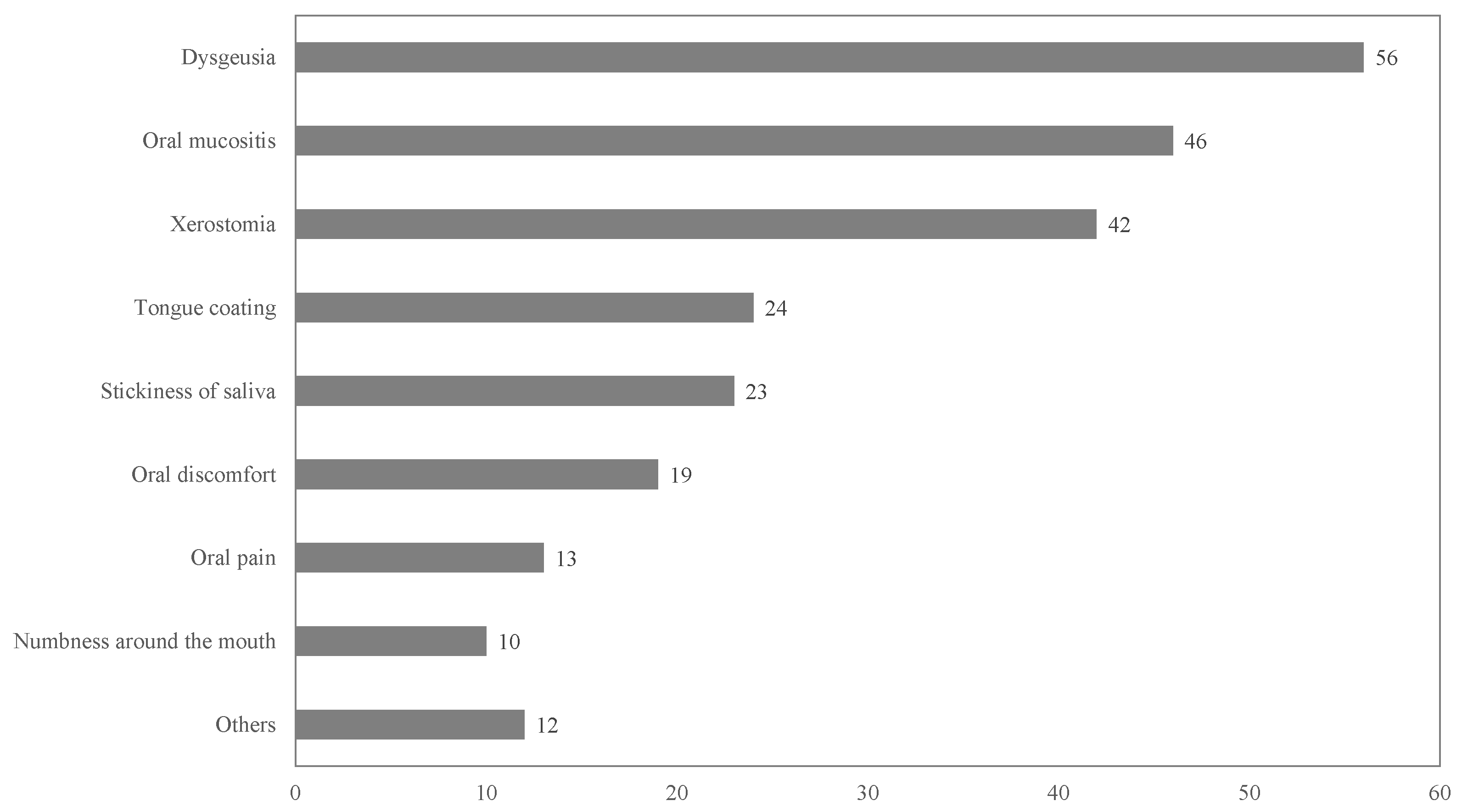

Table 1.
Items on the patient evaluation questionnaire used in this study.
| Q 1. | What type of oral adverse events do you have? |
| 1. Mucositis. 2. Tongue coating. 3. Dysgeusia. 4. Xerostomia. 5. Stickiness of saliva. 6. Numbness around the mouth 7. Oral pain 8. Oral discomfort. 8. None. | |
| Q 2. | Do you want to improve the oral adverse events? |
| 1. Yes. 2. No. | |
| Q 3. | Do the oral symptoms cause problems in your daily life? |
| 1. Yes. 2. No. | |
| Q 4. | What issues have become a problem in your daily life? |
| 1. Reduced food intake. 2. Increased food intake. 3. Drinking too much. 4. Drinking not much. 5. Difficulty swallowing. 6. Sleeplessness. 7. Impaired speech. 8. None. | |
| Q 5. | Do you want medication or a treatment method for oral adverse events? |
| 1. Yes. 2. No. | |
| Q 6. | Do you want dentist intervention to improve your oral adverse events? |
| 1. Yes. 2. No | |
| Q 7. | How severe are the oral adverse events compared with non-oral adverse events? |
| 1. More severe. 2. similar. 3. Not as severe. |
Table 2.
Patient characteristics (n = 216).
| Patient characteristics | n | % | ||
|---|---|---|---|---|
| Sex | Male | 108 | 50.0% | |
| Female | 108 | 50.0% | ||
| Age group (years old) | AYA (18–39) | 8 | 3.7% | |
| Middle aged (40–69) | 122 | 56.5% | ||
| Old aged (>70) | 86 | 39.8% | ||
| Cancer type | Breast cancer | 52 | 24.1% | |
| Lung cancer | 45 | 20.8% | ||
| Gastrointestinal cancer | 37 | 17.1% | ||
| Liver, biliary tract, pancreatic cancer | 18 | 8.3% | ||
| Urological cancer | 17 | 7.9% | ||
| Gynecological cancer | 14 | 6.5% | ||
| Hematological cancer | 12 | 5.6% | ||
| Head and neck cancer | 7 | 3.2% | ||
| Soft tissue sarcoma | 3 | 1.4% | ||
| Others | 11 | 5.1% | ||
| Cancer drug therapy | ICIs (Atezolizumab, Durvalumab, Pembrolizumab, Nivolumab, Avelumab) | 67 | 31.0% | |
| Taxane-based (DTX, PTX, nab-PTX, CBZ) | 49 | 22.7% | ||
| 5FU-based (5FU, TS-1, Cape) | 33 | 15.3% | ||
| Anthracycline-based | 8 | 3.7% | ||
| CDDP-based | 4 | 1.9% | ||
| EGFR antibodies (Cet, Pani) | 3 | 1.4% | ||
| Others | 52 | 24.1% | ||
| AYA, Adolescent and young adult; ICIs, Immune checkpoint inhibitors; DTX, Docetaxel; PTX, Paclitaxel; nab-PTX, nab-Paclitaxel; CBZ, Cabazitaxel acetonate; Cape, Capecitabine; CDDP, Cisplatin; EGFR, Epidermal growth factor receptor; Cet, Cetuximab; Pani, Panitumumab | ||||
Table 3.
The relationship between patient characteristics and oral adverse events.
| With | Without | Multivariate analysis | |||||
| n | n(%) | n(%) | OR | 95%CI | P-value | ||
| 216 | 127(58.8) | 89(41.2) | |||||
| Sex | Male | 109 | 54(49.5) | 55(50.5) | |||
| Female | 107 | 73(68.2) | 34(31.8) | 1.14 | 0.48-2.70 | 0.76 | |
| Age group (years) | AYA (18–39) | 8 | 4(50.0) | 4(50.0) | |||
| Middle-aged (40–69) | 122 | 77(63.1) | 45(36.9) | 3.21 | 0.59-17.70 | 0.18 | |
| Older (> 70) | 86 | 46(53.5) | 40(46.5) | 2.7 | 0.45-16.10 | 0.28 | |
| Cancer type | Others | 11 | 4(36.4) | 7(63.6) | |||
| Breast cancer | 51 | 38(74.5) | 13(25.5) | 6.38 | 1.05-38.90 | 0.04* | |
| Lung cancer | 46 | 18(39.1) | 28(60.9) | 1.45 | 0.31-6.73 | 0.64 | |
| Gastrointestinal cancer | 37 | 27(73.0) | 10(27.0) | 2.79 | 0.42-18.40 | 0.29 | |
| Liver, biliary tract, pancreatic cancer | 18 | 12(66.7) | 6(33.3) | 1.42 | 0.21-9.70 | 0.72 | |
| Urological cancer | 17 | 6(35.3) | 11(64.7) | 1.29 | 0.22-7.62 | 0.78 | |
| Gynecological cancer | 14 | 9(64.3) | 5(35.7) | 6 | 0.82-43.90 | 0.08 | |
| Hematological cancer | 12 | 7(58.3) | 5(41.7) | 5.61 | 0.76-41.70 | 0.09 | |
| Head and neck cancer | 7 | 5(71.4) | 2(28.6) | 5.25 | 0.57-48.10 | 0.14 | |
| Soft tissue sarcoma | 3 | 1(33.3) | 2(66.7) | 0.9 | 0.05-17.30 | 0.95 | |
| Cancer drug therapy | Others | 51 | 26(51.0) | 25(49.0) | |||
| 5FU-based (5FU, S1, Cape) | 33 | 27(81.8) | 6(18.2) | 9.37 | 1.74-50.40 | < 0.01* | |
| Taxanes-based (DTX, PTX, nab-PTX, CBZ) | 49 | 37(75.5) | 12(24.5) | 5.63 | 1.91-16.60 | < 0.01* | |
| Anthracyclines-based | 8 | 6(75.0) | 2(25.0) | 1.95 | 0.35-10.90 | 0.45 | |
| ICIs (Atezolizumab,Durvalumab,Pembrolizumab,Nivolumab,Avelumab) | 68 | 27(39.7) | 41(60.3) | 1.69 | 0.55-5.19 | 0.36 | |
| EGFR antibodies (Cet, Pani) | 3 | 1(33.3) | 2(66.7) | 0.84 | 0.05-14.50 | 0.91 | |
| CDDP | 4 | 3(75.0) | 1(25.0) | 11.1 | 0.80-156.00 | 0.07 | |
| †Significant association (p-value < 0.05 ) | |||||||
| OR:odds ratio | |||||||
| CI:confidence interval | |||||||
Table 3.
The relationship between cancer drug therapies and major oral adverse events.
| With | Without | Multivariate analysis | |||||
| n | n(%) | n(%) | OR | 95%CI | P-value | ||
| Dysgeusia | 216 | 56(25.9) | 160(74.1) | ||||
| Others | 51 | 9(17.6) | 42(82.4) | ||||
| 5FU-based (5FU, S1, Cape) | 33 | 12(36.4) | 21(63.6) | 1.36 | 0.23-8.19 | 0.74 | |
| Taxanes-based (DTX, PTX, nab-PTX, CBZ) | 49 | 22(44.9) | 27(55.1) | 4.76 | 1.61-14.10 | < 0.01* | |
| Anthracyclines-based | 8 | 4(50.0) | 4(50.0) | 3.50 | 0.71-17.30 | 0.13 | |
| ICIs (Atezolizumab,Durvalumab,Pembrolizumab,Nivolumab,Avelumab) | 68 | 7(10.3) | 61(89.7) | 0.74 | 0.19-2.89 | 0.66 | |
| EGFR antibodies (Cet, Pani) | 3 | 1(33.3) | 2(66.7) | 1.19 | 0.06-24.60 | 0.91 | |
| CDDP | 4 | 1(25.0) | 3(75.0) | 3.15 | 0.21-47.90 | 0.41 | |
| Oral mucositis | 216 | 46(21.3) | 170(78.7) | ||||
| Others | 51 | 13(25.5) | 38(74.5) | ||||
| 5FU-based (5FU, S1, Cape) | 33 | 13(39.4) | 20(60.6) | 2.70E+00 | 0.44-16.50 | 0.28 | |
| Taxanes-based (DTX, PTX, nab-PTX, CBZ) | 49 | 14(28.6) | 35(71.4) | 1.85E+00 | 0.65-5.25 | 0.25 | |
| Anthracyclines-based | 8 | 2(25.0) | 6(75.0) | 7.38E-01 | 0.13-4.21 | 0.73 | |
| ICIs (Atezolizumab,Durvalumab,Pembrolizumab,Nivolumab,Avelumab) | 68 | 4(5.9) | 64(94.1) | 4.48E-01 | 0.10-2.00 | 0.29 | |
| EGFR antibodies (Cet, Pani) | 3 | 0(0.0) | 3(100.0) | 7.68E-08 | 0-Inf | 0.99 | |
| CDDP | 4 | 0(0.0) | 4(100.0) | 1.50E-07 | 0-Inf | 0.99 | |
| Xerostomia | 216 | 42(19.4) | 174(80.6) | ||||
| Others | 51 | 6(11.8) | 45(88.2) | ||||
| 5FU-based (5FU, S1, Cape) | 33 | 11(33.3) | 22(66.7) | 1.65E+01 | 1.74-157.00 | 0.01* | |
| Taxanes-based (DTX, PTX, nab-PTX, CBZ) | 49 | 11(22.4) | 38(77.6) | 2.65E+00 | 0.80-8.79 | 0.11 | |
| Anthracyclines-based | 8 | 2(25.0) | 6(75.0) | 2.05E+00 | 0.32-13.10 | 0.45 | |
| ICIs (Atezolizumab,Durvalumab,Pembrolizumab,Nivolumab,Avelumab) | 68 | 11(16.2) | 57(83.8) | 2.29E+00 | 0.55-9.53 | 0.25 | |
| EGFR antibodies (Cet, Pani) | 3 | 0(0.0) | 3(100.0) | 8.49E-07 | 0-Inf | 1.00 | |
| CDDP | 4 | 1(25.0) | 3(75.0) | 7.63E+00 | 0.39-148.00 | 0.18 | |
| †Significant association (p-value < 0.05) |
|||||||
| OR:odds ratio | |||||||
| CI:confidence interval | |||||||
Table 4.
Responses to the question: Do you require management of oral adverse events by medical professionals?
Table 4.
Responses to the question: Do you require management of oral adverse events by medical professionals?
| Response | ||||
|---|---|---|---|---|
| Total | Yes | No | ||
| Item | n(%) | n(%) | n(%) | |
| Hope for improvement of oral adverse events | 115(90.6) | 68(53.5) | 47(37.0) | |
| Impact on their daily lives | 113(89.0) | 44(34.6) | 69(54.3) | |
| Hope for professional oral care (Well-Trained Dentist and Dental Hygienist) | 102(80.3) | 34(26.8) | 68(53.5) | |
| more severe | similar | not as severe | ||
| Comparison of the severity of oral adverse events and other adverse events | 113(89.0) | 5(3.9) | 27(21.3) | 81(63.8) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



