
Submitted:
31 December 2024
Posted:
03 January 2025
You are already at the latest version
Abstract
Background: To date, myocardial strain parameters have been poorly investigated in women with previous gestational diabetes mellitus (pGDM). No previous study provided a comprehensive evaluation of all biventricular and biatrial deformation indices in pGDM women. Accordingly, we aimed at investigating the structure and myocardial deformation properties of all cardiac chambers in a cohort of pGDM women, at 4 years post-partum.
Methods: A consecutive cohort of pGDM women was compared to a control group of healthy women with previous uncomplicated pregnancy, matched by age, ethnicity and gestational week, at 4 years postpartum. Both groups of women underwent a conventional transthoracic echocardiography (TTE) implemented with complete analysis of biventricular and biatrial myocardial deformation indices by speckle tracking echocar-diography (STE). The primary endpoint was subclinical myocardial dysfunction, defined as left ventricular (LV) global longitudinal strain (GLS) magnitude 27 Kg/m2 and third trimester glycosylated hemoglobin >33 mmol/mol showed the best sensitivity and specificity for predicting both endpoints. Conclusions: Pregnant women with previous history of GDM complicated by overweight/obesity and uncontrolled diabetes have a significantly in-creased risk of subclinical myocardial dysfunction and early carotid atherosclerosis at 4 years postpartum.
Keywords:
previous gestational diabetes mellitus
; subclinical myocardial dysfunction
; early carotid atherosclerosis
; body mass index
; glycosylated hemoglobin
1. Introduction
The global prevalence of gestational diabetes mellitus (GDM), defined as glucose intolerance with first onset during pregnancy, is approximately 15%, and prevalence rates are expected to continue rising [1]. During pregnancy, GDM is associated with increased risk of adverse maternal and neonatal outcomes, including pre-eclampsia, preterm birth, stillbirth, large for gestational age, and neonatal hyperinsulinaemia [2,3,4]. Although GDM usually resolves after birth, a growing number of long-term observational studies suggest that the impact persists over time. For example, women with previous history of gestational diabetes mellitus (pGDM) were reported to be at increased risks of developing type 2 diabetes mellitus, metabolic syndrome, and chronic kidney disease later in life [5,6,7,8]. Through meta-analyses, the size of this risk association has been estimated to be a relative risk of almost 10 for type 2 diabetes mellitus and almost 2 for cardiovascular (CV) disease in the first decade postpartum [5,9,10]. The magnitude of these risks highlights the importance of intervening to prevent the onset of T2DM and the occurrence of adverse CV events, particularly in the early years after pregnancy [5]. For this reason, it is important to recognize eventual abnormalities of cardiac structure and function in pGDM women at an early stage, prior the occurrence of adverse outcomes.
Transthoracic echocardiography (TTE) is the most widely used noninvasive imaging modality for maternal heart monitoring in pregnancy and postpartum. It allows to obtain a detailed evaluation of cardiac chamber size, to assess left ventricular (LV) diastolic function, and to quantify LV systolic function by estimating left ventricular ejection fraction (LVEF) [11]. Although LVEF is the most commonly used echocardiographic measure of systolic function, it has several limitations, including the geometric assumptions made in its calculation, its high load-dependence, and the significant intra-observer, inter-observer and test-retest variability [12,13]. Moreover, LVEF measures global LV systolic function only, and it does not identify intrinsic abnormalities of regional wall contractility [14]. In fact, LVEF can be normal in the early stages of cardiac diseases, and therefore it is a late marker of LV systolic dysfunction [15].
During the last decade, advances in cardiac imaging have led to the introduction of two-dimensional (2D) speckle tracking echocardiography (STE), which can allow early detection of subclinical myocardial dysfunction [16]. Global longitudinal strain (GLS), which is the most commonly used 2D-STE-derived deformation index of cardiac contractility, can detect systolic dysfunction much earlier than LVEF, thus identifying individuals with subclinical myocardial damage [17].
To date, several studies [18,19,20,21,22,23,24,25,26] have demonstrated that, despite normal TTE-derived LVEF, GLS in GDM women was significantly, even though modestly, reduced in comparison to healthy pregnant women. Conversely, subclinical myocardial dysfunction has been poorly investigated in women with previous history of GDM (pGDM women) [27,28]. Given that the risk of CV events in pGDM women is higher within the first decade after pregnancy [9], the present study was primarily designed to evaluate cardiac structure and function in a cohort of pGDM women in comparison to women with previous uncomplicated pregnancy, at 4 years postpartum.
2. Materials and Methods
2.1. Patient Selection
This observational case-control study analyzed a consecutive series of pGDM women compared to a control group of normotensive healthy women with previous uncomplicated pregnancy, matched by age, ethnicity and gestational week, between February 2024 and April 2024. The two groups of women underwent delivery at the Division of Gynecology and Obstetrics of San Giuseppe Multimedica Hospital (Milano), between March 2021 and June 2021.
Inclusion criteria were: women with previous history of GDM, defined according to the International Association of Diabetes and Pregnancy Study Groups (IADPSG) criteria [29] when any of the following criteria were met during the “one-step” 75-g oral glucose tolerance test (OGTT) between 24 and 28 gestational weeks: 1) fasting plasma glucose ≥92 mg/dl; 2) 1-h plasma glucose (1hPG) during OGTT ≥180 mg/dl; and 3) 2hPG during OGTT ≥153 mg/dl. Exclusion criteria were the following: previous evidence of any form of pregestational diabetes mellitus (Type 1 or Type 2), significant comorbidities (cardiovascular disorders, respiratory diseases and/or renal diseases), gestational or pre-existing hypertensive disorder, haemodynamic instability, poor or inadequate echocardiographic acoustic windows (not appropriate for adequate endocardial border definition of both ventricles and atria).
The following data were collected by accessing women’s medical records available in the hospital archive: anagraphic age, ethnicity, body surface area, body mass index (BMI), waist-to-hip ratio (WHR), prevalence of main cardiovascular risk factors, parity, relevant comorbidities, systolic (SBP) and diastolic (DBP) blood pressure values, gestational week at diagnosis of GDM, gestational age at delivery, the type of delivery, the neonatal birth weight, electrocardiographic data (cardiac rhythm and heart rate), blood tests comprehensive of complete blood count for determining hemoglobin concentration, red cell distribution width (RDW) and neutrophil-to-lymphocyte ratio (NLR), serum levels of creatinine and estimated glomerular filtration rate (eGFR) [30], total cholesterol, uric acid and finally glycosylated hemoglobin; finally, the third-trimester and current medical treatment.
During each clinical visit, each woman underwent an instantaneous blood pressure (BP) measurement, electrocardiogram (ECG), a conventional TTE implemented with complete STE analysis of both ventricles and atria and finally a carotid ultrasonography. All instrumental examinations were carried out by the same cardiologist (A.S.) on the same day.
All procedures were in accordance with the ethical standards of our Institutional Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. The study protocol was approved by the Comitato Etico Territoriale Lombardia 5 (Committee’s reference number 507/24, date of approval 22 October 2024).
2.2. Conventional Echocardiographic Examination
All echocardiograms were performed by using commercially available Philips Sparq ultrasound machine (Philips, Andover, Massachusetts, USA) with a 2.5 MHz transducer. All images were acquired with the woman in left lateral decubitus, and parameters measured according to the Recommendations of the American Society of Echocardiography and the European Association of Cardiovascular Imaging [31,32].
Following conventional echocardiographic parameters were recorded: the aortic root and ascending aorta diameters by using the “leading edge-to-leading edge” convention; the relative wall thickness (RWT), calculated with the formula RWT = 2 posterior wall thickness/LV internal diameter at end-diastole; the left ventricular mass index (LVMi), calculated by the Devereux’s formula; the left ventricular end-diastolic volume index (LVEDVi) and the left ventricular end-systolic volume indexed (LVESVi); the left ventricular ejection fraction (LVEF), estimated with the biplane modified Simpson’s method, as index of LV systolic function [31]; the left atrial volume index (LAVi); the right ventricular inflow tract (RVIT); the tricuspid annular plane systolic excursion (TAPSE), as index of right ventricular (RV) systolic function; finally, the inferior vena cava (IVC) diameter during normal respiration.
Doppler measurements included E/A ratio and E/average e’ ratio, as indices of LV diastolic function and left ventricular filling pressure (LVFP), respectively [32]. Systolic pulmonary artery pressure (sPAP) was derived by the modified Bernoulli equation, where sPAP = 4 × [tricuspid regurgitation velocity (TRV)]2 + right atrial pressure [33]. The latter was estimated from IVC diameter and collapsibility. Finally, TAPSE/sPAP ratio was measured as noninvasive index of RV/pulmonary artery (PA) coupling [34].
Degree of concomitant valvulopathy was assessed according to the AHA/ACC recommendations for the management of patients with valvular heart diseases [35].
2.3. Measurement of Epicardial Adipose Tissue Thickness
Epicardial adipose tissue (EAT) thickness was measured at the end of systole on the RV free wall from the parasternal long-axis view on standard TTE and was defined as an echo-free or hypoechoic area adjacent to the right ventricle [36].
2.4. Hemodynamic Indices
Following hemodynamic parameters were obtained: SBP, DBP and mean arterial pressure (MAP). The latter was assessed by the following formula: MAP = DBP + [(SBP-DBP/3)] [37].
Stroke volume (SV) was obtained from the product of the left ventricular outflow tract (LVOT) area and LVOT time velocity integral, using pulsed Doppler echocardiography; cardiac output (CO) was calculated by multiplying the SV by the heart rate [38].
Finally, total peripheral resistance (TPR) (dyne x sec/cm5) was calculated with the formula TPR = MAP (kPa)/CO (l/min) x 80 [39].
To assess LV-arterial coupling, following parameters were measured: 1) End-systolic pressure (ESP), estimated as 0.9 x brachial SBP [40]; 2) SV; 3) Effective arterial elastance index (EaI), calculated as EaI = ESP/SVindex ratio [41]; 4) End-systolic elastance index (EesI), estimated as EesI = ESP/(LVESVi − V0), assuming that V0 (LV hypothetical volume at zero pressure) is negligible compared with LVESVi [41]. Ventricular-arterial coupling (VAC) was calculated as the EaI/EesI ratio.
2.5. Speckle-Tracking Echocardiography
Immediately after conventional TTE, high-resolution speckle-tracking strain analyses were performed on 2D images in the following order: apical four-chamber, two-chamber and three-chamber views for LV longitudinal strain, and on basal, medial and apical short-axis views for LV circumferential strain, using the automated function imaging and the Q-Analysis module [42].
According to Philips QLAB software, LV wall was divided into seven segments in each apical view. LV peak systolic strain was defined as the point of maximal systolic shortening for longitudinal and circumferential strain. A single bull’s-eye summary for LV-GLS and LV-global circumferential strain (GCS) was obtained, presenting the analysis for each segment along with the assessment of global LV strain. Early peak diastolic strain rate was derived from longitudinal and circumferential measurements [42].
RV-GLS was measured from the apical four-chamber view by averaging local strains obtained from septal and lateral segments. Right ventricular free wall longitudinal strain (RV-FWLS) was calculated as the mean of RV lateral basal, mid and apical segments, with exclusion of septal segments [43].
To calculate left atrial (LA) strain, the software automatically divided the atrial wall into seven segments and a “biplane method” was employed. The following measurements were performed: the peak positive LA longitudinal strain corresponding to left atrial conduit strain (LAScd), the peak negative LA longitudinal strain corresponding to left atrial contractile strain (LASct); the sum of the two peaks corresponding to left atrial reservoir strain (LASr). Mean LAScd, LASct and LASr were calculated by averaging the four-chamber and two-chamber endocardial LA longitudinal strains. From the 2D atrial strain, following strain rate curves were derived: the first positive global strain rate, from the beginning of ventricular systole; global early-diastolic strain rate; global late-diastolic strain rate [44]. Moreover, we calculated an echocardiographic index of LA stiffness, that is the LASr/E/average e’ ratio [45].
Finally, for right atrial reservoir strain (RASr) assessment, markers were placed to the edges of the tricuspid annulus and the endocardial side of the superior right atrial region.
2.6. Carotid Ultrasonography
All carotid ultrasound examinations were performed by using the Philips Sparq ultrasound machine with a 12 MHz transducer. The carotid arteries were examined using a standardized Protocol [50]. With the woman in the supine position with slight hyperextension and rotation of the neck to the contralateral side in order to optimize image quality, ultrasonographic images were scanned at end-diastole (defined as the R wave of an electrocardiogram).
The following parameters were manually measured by a 2D technique: average intima-media thickness (IMT) values of the left and right common carotid arteries (CCAs), average values of the left and right CCA-end-diastolic internal diameter (EDD). Measurements were made in the distal CCA at 1 cm from the carotid bifurcation. Average value of the left and right carotid RWT was derived from the formula: 2 × average IMT/average CCA-EDD, while average value of the left and right CCA-cross-sectional area (CSA) (mm2) was calculated according to the formula: [π × (2 × average IMT + average CCA-EDD)/2)2 − π × (average CCA-EDD/2)2], as a surrogate for carotid arterial mass.
Considering that normal IMT values and reference ranges are age- and sex-dependent and that there is a significant steady increase in IMT with advancing age in all carotid segments [51], values for CCA-IMT were adapted to the age of our study population. Notably, given that the reference limit of IMT according to the age class 40-49 yrs is 0.67 mm [52], a CCA-IMT ≥0.7 mm was the cut-off employed to define CCA intima-media thickening in our study population.
2.7. Statistical Analysis
The primary endpoint of the study was to identify the parameters independently associated with subclinical myocardial dysfunction, defined as a LV-GLS value <20% in the presence of preserved LVEF (≥55%) [11], in pGDM women at 4 years postpartum. The secondary endpoint was to detect the independent predictors of increased CCA-IMT (≥0.7 mm) [52] in the same cohort of pGDM women.
A sample size calculation was performed for purpose of the study. A sample size of 30 women with previous history of GDM and 30 healthy controls reached 80% of statistical power to detect a two-point difference in the GLS magnitude (i.e. 20% vs 18%) measured at 4 yrs postpartum in the two groups of women with a standard deviation of 2.5 for each parameter, using a two-sided equal-variance t-test with a level of significance (alpha) of 5%.
Each continuous variable was checked through the Shapiro-Wilk test and all data were determined to be normally distributed. Accordingly, for the whole study population and for each group of HFpEF patients, continuous data were summarized as mean ± standard deviation, while categorical data were presented as number (percentage). Continuous variables were compared using a two-sample independent t test, whereas categorical parameters were compared using the Chi-squared test or the Fisher’s exact test.
Logistic regression analyses were performed to identify the independent predictors of subclinical myocardial dysfunction and intima-media thickening, in pGDM women, at the 4-year follow-up. According to the “one in ten rule” (one predictive variable for every ten outcome events), only the following variables were included in the logistic regression analysis: third trimester age (as demographic parameter), third trimester BMI (as anthropometric variable), third trimester glycosylated hemoglobin (as glycometabolic index), third trimester NLR (as systemic marker of inflammation) and third trimester MAP (as hemodynamic index). For each variable investigated, correspondent odds ratios with 95% confidence intervals (CIs) were calculated. Only the variables with statistically significant association on univariate analysis (p-value < 0.05) were thereafter included in the multivariate logistic regression model. The receiver operating characteristics (ROC) curve analysis was performed to establish the sensitivity and the specificity of the main statistically significant continuous variable for predicting both endpoints over follow-up period. Area under curve (AUC) was estimated. The optimal cutoff of each statistically significant continuous variable was calculated using the maximum value of the Youden Index (determined as sensitivity + [1-specificity]).
A detailed intra-observer and inter-observer variability analysis of LV-GLS assessment by 2D-STE was conducted in a subgroup of 15 randomly selected pGDM women. LV-GLS was remeasured by the same cardiologist who performed all echocardiographic examinations (A.S.) and by a second one (M.L.). The analyses were performed in a blinded manner. The intraclass correlation coefficient (ICC) with its 95% CI was used as a statistical method for assessing intra-observer and inter-observer measurement variability. An ICC of 0.70 or more was considered to indicate acceptable reliability.
Statistical analysis was performed with SPSS version 28 (SPSS Inc., Chicago, Illinois, USA), with two-tailed p-values below 0.05 deemed statistically significant.
3. Results
3.1. Clinical Findings
A total of 32 pGDM women and 30 age-, ethnicity- and gestational week-matched healthy controls without any comorbidity were analyzed at 4 yrs postpartum.
Main clinical, obstetrical, hemodynamic and laboratory parameters collected in the two study groups at the third trimester of pregnancy are summarized in Table 1.
Compared to controls, GDM women had a significantly higher third trimester BMI (≥30 Kg/m2 in 43.7% of women) and a significantly higher prevalence of dyslipidemia and family history of diabetes. BP measurements revealed significantly higher values in GDM women than controls, even in absence of arterial hypertension (BP ≥ 140/90 mmHg). On third trimester blood tests, GDM women were found with significantly higher inflammatory indices (RDW and NLR), serum total cholesterol and serum uric acid than controls. Overall, GDM women showed a good glycemic control (third trimester glycosylated hemoglobin 34.7 ± 4.1 mmol/mol). Approximately two-third of GDM cases (68.7% of total) were diagnosed after the 24 weeks of gestation, whereas one-third (31.3% of total) were diagnosed earlier in pregnancy. Among GDM participants, 18 (56.2% of total) were on diet and the remaining 14 (43.8% of total) on insulin. GDM women underwent delivery much earlier than controls, while the analysis of the other delivery parameters did not reveal any statistically significant difference between the two groups of women.
At the clinical visit performed at the 4-year follow-up, one-third of pGDM women resulted to be affected by type 2 diabetes mellitus, dyslipidemia, arterial hypertension and obesity. Considering the average WHR obtained in pGDM women (0.90 ± 0.16), the most prevalent obesity phenotype was the android one. Among pGDM women, 12.5% of total were treated with oral hypoglycemic agents and/or antihypertensive drugs (%), whereas only 6.2% of total made regular use of statins (Table 2).
3.2. Instrumental Findings
Table 3 lists all morphological, functional and hemodynamic parameters assessed by conventional TTE and carotid ultrasonography in the two groups of women at 4 yrs postpartum.
On TTE examination, biventricular and biatrial cavity sizes were similar in the two groups of women. Even in absence of manifest pathological LV remodeling, pGDM women were diagnosed with significantly greater RWT, LVMi and LA antero-posterior diameter than controls. LV systolic function, assessed by LVEF, was normal and similar in both groups of women. Analysis of LV diastolic function revealed a significantly higher E/average e’ ratio in pGDM women in comparison to controls. No significant valvulopathy was detected in both study groups. The assessment of pulmonary hemodynamics showed that both TAPSE and TAPSE/sPAP ratio were significantly reduced in women with previous GDM than controls. Finally, EAT thickness was significantly increased in pGDM women than controls.
The analysis of hemodynamic indices showed that SV and CO were significantly lower in pGDM women than controls, whereas the heart rate was similar in the two groups of woman. In addition, TPRi were significantly increased in pGDM women.
Concerning VAC parameters, pGDM women were found with significantly higher EaI than controls, while EesI was similar in the two groups of women; the resultant VAC (EaI/EesI ratio) was significant greater in pGDM women than controls.
On carotid ultrasonography, the average values of CCA-IMT, CCA-RWT and CCA-CSA were all significantly larger in pGDM women than controls.
Strain echocardiographic imaging revealed that most biventricular and biatrial myocardial strain and strain rate parameters were significantly reduced in pGDM women in comparison to healthy controls. Overall, more than half of pGDM women were diagnosed with lower biventricular and biatrial myocardial strain parameters in comparison to the accepted reference values [11,46,47,48,49]. Interestingly, approximately one-fifth of healthy controls were found with a mild attenuation of myocardial deformatin indices (Table 4).
Multipanel Figure 1 illustrates examples of biventricular and biatrial longitudinal strain parameters measured from the apical four-chamber view in a pGDM woman included in the present study.
3.3. Follow-Up Data
Mean follow-up period was 4.0 ± 1.9 yrs. During follow-up, no pGDM woman developed any symptoms and signs of cardiomyopathy. No major adverse CV event was recorded.
At the 4-year follow-up, approximately two-third of pGDM women (62.5% of total) developed subclinical myocardial dysfunction revealed by STE analysis and one-third of total were diagnosed with type 2 diabetes mellitus (31.2% of total) or arterial hypertension (31.2% of total). Moreover, 25 pGDM women (78.1% of total) were found with subclinical carotid atherosclerosis.
On logistic regression analysis performed for identifying the independent predictors of subclinical myocardial dysfunction, defined by a LV-GLS magnitude <20% [11], at the 4-year postpartum, third trimester BMI (OR 1.88, 95% CI 1.19-2.98, p = 0.03) and glycosylated hemoglobin (OR 2.34, 95% CI 1.08-5.04, p = 0.02) were independently associated with the primary endpoint (Table 5).
ROC curve analysis revealed that both third trimester BMI >27 Kg/m2 and third trimester glycosylated hemoglobin >33 mmol/mol had 95% sensitivity and 99% specificity for predicting GLS impairment in pGDM women at the 4-year follow-up (Figure 2, A and B, respectively).
Figure 3 illustrates examples of GLS bull's-eye plots obtained in a pGDM woman with third trimester BMI >27 Kg/m2 and third trimester glycosylated hemoglobin >33 mmol/mol (A) and in a woman with previous uncomplicated pregnancy (B), respectively.
Third trimester BMI (OR 1.35, 95% CI 1.02-1.79, p = 0.03) and third trimester glycosylated hemoglobin (OR 1.37, 95% CI 1.00-1.88, p = 0.02) were also independently associated with increased CCA-IMT (≥0.7 mm) in pGDM women, at 4 years postpartum (Table 6).
A third trimester BMI >27 Kg/m2 and third trimester glycosylated hemoglobin >33 mmol/mol showed the best sensitivity and specificity for predicting the secondary endpoint (Figure 4, A and B, respectively).
3.4. Measurement Variability
A detailed intra- and inter-observer variability analysis of LV-GLS assessment was conducted in a group of 15 randomly selected pGDM women. Intra- and inter-observer agreement between the raters, expressed as ICCs, was 0.92 (95% CI 0.78-0.97) and 0.82 (95% CI 0.55-0.94), respectively.
4. Discussion
4.1. Main Findings of the Present Study
This prospective case-control study demonstrated that, compared to healthy women with previous uncomplicated pregnancy, pGDM women showed: 1) a subtle LV remodeling characterized by greater RWT and LVMi, with no evidence of LV concentric remodeling or LV concentric hypertrophy on TTE; 2) a moderate increase in the E/average e’ ratio, falling the so-called “gray-zone” (between 8 and 13), with no evidence of pathological increase in LVFP; 3) lower TAPSE and TAPSE/sPAP ratio, without RV-PA uncoupling (defined as TAPSE/sPAP ratio <0.80) [26]; 4) higher arterial elastance and VAC; 5) early carotid artery remodeling with greater CCA-RWT and CCA-CSA. Despite normal LVEF on conventional TTE, 2D-STE analysis highlighted a modest, but significant, impairment in almost all biventricular and biatrial myocardial strain parameters in pGDM women vs. controls. No relevant CV event was recorded over follow-up period. However, approximately two-third of pGDM women showed subclinical myocardial dysfunction on strain echocardiographic imaging and one-third of total were found with type 2 diabetes mellitus or arterial hypertension, at the 4-year follow-up. Third trimester BMI and third trimester glycosylated hemoglobin were the main prognostic indicators of both primary and secondary endpoints. Notably, a third trimester BMI >27 Kg/m2 and a third trimester glycosylated hemoglobin >33 mmol/mol were the best cut-off values for predicting subclinical myocardial dysfunction and subclinical atherosclerosis in pGDM women, at 4 yrs postpartum.
4.2. Comparison with Previous Studies and Interpretation of Results
To the best of our knowledge, to date only two studies [27,28] have evaluated myocardial strain parameters in pGDM women. In the CARDIA study [27], 64 women with GDM and 545 with uncomplicated pregnancy were followed up with echocardiography 5 and 20 years after delivery. Compared with women with non-GDM pregnancies, pGDM women had significantly lower magnitude of GLS, lateral e' wave velocity, and septal e' wave velocity and a greater 20-year increase in LVMi. All these findings were independent of subsequent development of type 2 diabetes mellitus. Aguilera J et al. [28] studied 73 women with GDM and 73 controls with uncomplicated pregnancy both at the third trimester of pregnancy and in postpartum period. In their findings, GDM women had significantly higher LVMi and E/average e’ ratio and significantly lower E/A and LV-GLS than controls; there were no significant differences between the groups in LVEF, CO and TPR; at 6 months after delivery, most cardiac functional indices improved in both pGDM women and controls, but in the pGDM group, compared to controls, there was a lower degree of improvement in E/A ratio and LV-GLS.
Differently from the above-mentioned studies, the present study evaluated not only LV-GLS, but performed a comprehensive assessment of myocardial deformation properties of all cardiac chambers in the pGDM women included. The subclinical myocardial dysfunction involved both ventricles and atria. As far as we know, this is the first study that evaluated the structure and function of all cardiac chambers in pGDM women in the first decade postpartum. The results of the present study confirmed the superiority of strain echocardiographic imaging over conventional TTE in detecting a subclinical impairment in myocardial deformation indices, in absence of any signs and symptoms of cardiomyopathy and in the presence of a preserved LVEF (≥55%). Our findings are in agreement with the knowledge that that decline in diastolic function often precedes systolic dysfunction and that LVEF is a late marker of ventricular dysfunction, whereas changes in myocardial deformation are the first detectable preclinical functional alterations.
According to the most recent literature data, the occurrence of both subclinical myocardial dysfunction and carotid artery remodeling in pGDM women would exist even in the absence of type 2 diabetes [53,54,55]. It is not clear if the subclinical cardiovascular disease is the result of the hyperglycemic insult on the cardiovascular system during pregnancy or the consequence of a prolonged exposure to an adverse cardiovascular risk factor profile before, during and after pregnancy. It is known that obesity [56,57], dyslipidemia [58], arterial hypertension [59], insulin resistance and hyperinsulinemia [60] are all strong risk factors for an abnormal pattern of myocardial deformation on strain echocardiographic imaging. In light of our findings, even a brief period of exposure to the hemodynamic overload related to overweight/obesity together with hyperinsulinemia due to uncontrolled GDM might have contributed to the persistent impairment in all biventricular and biatrial myocardial strain indices, detected in pGDM women.
Given that obesity [61] and hyperinsulinemia [62] have been recognized as key determinants for the development of the heart failure with preserved ejection fraction, the results of the present study would suggest that pGDM women with obesity and uncontrolled diabetes could be candidates to a future development of this echocardiographic phenotype of heart failure.
Consistent with previous studies [63,64,65,66], the present study also confirmed the strong association between previous history of GDM and the subsequent occurrence of subclinical carotid atherosclerosis. This association is triggered by third trimester overweight/obesity and increased glycosylated hemoglobin, and accelerated by age, smoking, dyslipidemia and arterial hypertension, that may all synergically contribute to early carotid atherosclerosis [67].
The increase in VAC and the concomitant decrease in RV/PA coupling observed in our cohort of pGDM women was attributed by our study group to an increased stiffening involving both systemic and pulmonary circulation. It is likely that an increased LV and RV afterload might have favoured the attenuation of biventricular deformation properties, similarly to what observed in large cohorts of hypertensive individuals [68].
The attenuation of myocardial deformation indices detected in more than half of pGDM women and in approximately one-fifth of healthy controls may also be explained by the potential influence exerted by anthropometrics, such as a concave-shaped chest wall conformation, abdominal and/or thoracic adiposity on biventricular and biatrial mechanics [69,70]. Indeed, it is not possible to exclude that a “cardiac restriction” due to a narrow antero-posterior thoracic diameter and/or compressive phenomena may have contributed to reduce myocardial deformation indices, particularly at basal level, in some pGDM women and/or healthy controls. However, this methodological issue was not investigated in the present study.
4.3. Implications for Clinical Practice
The results of the present study revealed that cardiovascular functional changes that begin during the third trimester of pregnancy may persist long after delivery and may contribute to the future occurrence of subclinical myocardial dysfunction and early carotid atherosclerosis within the first decade postpartum. Considering the increased CV risk associated with GDM diagnosis, the most recent guidelines and scientific consensus documents recommend accurate screening of women at risk and application of CV prevention strategies. In particular, the American College of Obstetricians and Gynecologists (ACOG) [71] and the American Diabetes Association (ADA) [72] recommend an OGTT at 4 to 12 weeks postpartum as screening tool for diabetes for all patients with GDM. If the OGTT is abnormal, a referral for specialized management is recommended. If the OGTT is normal, a repeat screening, comprehensive of fasting plasma glucose and glycosylated hemoglobin every 1 to 3 years, is recommended by both organizations. A prevention stategy based on weight control and adequate glycemic control should be implemented in the clinical practice for GDM women earlier in pregnancy and continued in the postpartum period and throughout the pGDM woman's life. With this regard, physical activity before pregnancy and a lower initial weight may reduce the risk of developing GDM and cardiovascular complications in pregnancy [73]. In addition, any effort should be made to minimize modifiable cardiovascular risk factors, including hypertension, visceral adiposity, and dyslipidemia, for lowering cardiovascular risk in such women. Given that it has been reported that even early subclinical atherosclerosis may be reduced by cardioprotective drugs, such as statins and anti-hypertensive agents [74], these medications should be considered in pGDM women with concomitant arterial hypertension and dyslipidemia. In light of our findings, strain echocardiographic imaging should be considered for implementation in the clinical practice, particularly during pregnancies complicated by GDM and during the first decade postpartum. This innovative methodology may dectect subtle changes in myocardial deformation indices, providing incremental diagnostic and prognostic information on biventricular and biatrial mechanics, over conventional TTE examination.
4.4. Limitations of the Study
Main limitations of the present study were its monocentric nature and the limited number of pGDM women analyzed. However, the number of pGDM women included was justified by an accurate sample size calculation. Moreover, our study group was evaluated by TTE implemented with STE only at 4 years postpartum; therefore, it is not possible to establish whether the impairment in biventricular and biatrial deformation was already present during the previous pregnancy complicated by GDM. In addition, biventricular and biatrial myocardial deformation indices were obtained by using the same software employed for LV-GLS assessment, the only one available at our Institution. It is noteworthy that strain echocardiographic imaging suffers from a number of limitations, such as its dependence on good image quality, on frame rates (generally, no less than 40 fps), on the operator’s experience, on loading conditions, on the ultrasound system employed for the analysis and on chest wall conformation [75,76,77,78]. Finally, the pGDM women included in the present study did not perform blood tests, comprehensive of C-reactive protein, N-terminal pro-B-type natriuretic peptide (NT-proBNP) and Homeostatic Model Assessment for Insulin Resistance (HOMA-IR), not foreseen in the research protocol. These inflammatory, hemodynamic and metabolic markers would have contributed to better understand the pathophysiological mechanisms of both cardiac and carotid artery remodeling detected in pGDM women at 4 years postpartum.
5. Conclusions
Pregnant women with previous history of GDM complicated by overweight/obesity and uncontrolled diabetes have a significantly increased risk of subclinical myocardial dysfunction and early carotid atherosclerosis at 4 years postpartum.
Strain echocardiographic imaging should be considered for implementation in the clinical practice for early identifying, among pGDM women, those with subclinical myocardial dysfunction, who might benefit from a closer clinical follow-up and/or a more aggressive medical treatment, aimed at reducing the risk of CV complications later in life.
Author Contributions
Conceptualization, A.S. and G.L.N..; methodology, A.S. and F.C.; software, A.S.; validation, S.B.; formal analysis, A.S.; investigation, A.S.; resources, S.B.; data curation, A.S. and F.C.; writing—original draft preparation, A.S.; writing—review and editing, F.C. and G.L.N.; visualization, S.B. and M.L.; supervision, S.B. and M.L.; project administration, S.B.; funding acquisition, A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Italian Ministry of Health, Ricerca Corrente IRCCS MultiMedica.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Comitato Etico Territoriale Lombardia 5 (Committee’s reference number 507/24), date of approval 22 October 2024.
Informed Consent Statement
Informed consent was obtained from all individual participants included in the study.
Data Availability Statement
Data extracted from included studies will be publicly available on Zenodo (https://zenodo.org).
Acknowledgments
The authors wish to thank Monica Fumagalli for her graphical support.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Wang, H.; Li, N.; Chivese, T.; Werfalli, M.; Sun, H.; Yuen, L.; Hoegfeldt, C.A.; Elise Powe, C.; Immanuel, J.; Karuranga, S.; et al. IDF Diabetes Atlas: Estimation of Global and Regional Gestational Diabetes Mellitus Prevalence for 2021 by International Association of Diabetes in Pregnancy Study Group's Criteria. Diabetes Res. Clin. Pract. 2022, 183, 109050. [Google Scholar] [CrossRef] [PubMed]
- Ye, W.; Luo, C.; Huang, J.; Li, C.; Liu, Z.; Liu, F. Gestational diabetes mellitus and adverse pregnancy outcomes: systematic review and meta-analysis. BMJ. 2022, 377, e067946. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Cai, J.; Xu, Y.; Long, Y.; Deng, L.; Lin, S.; Zhang, J.; Yang, J.; Zhong, L.; Luo, Y.; et al. Early Diagnosed Gestational Diabetes Mellitus Is Associated With Adverse Pregnancy Outcomes: A Prospective Cohort Study. J. Clin. Endocrinol. Metab. 2020, 105, dgaa633. [Google Scholar] [CrossRef]
- Lowe, W.L. Jr; Scholtens, D.M.; Kuang, A.; Linder, B.; Lawrence, J.M.; Lebenthal, Y.; McCance, D.; Hamilton, J.; Nodzenski, M.; Talbot, O.; et al. Hyperglycemia and Adverse Pregnancy Outcome Follow-up Study (HAPO FUS): Maternal Gestational Diabetes Mellitus and Childhood Glucose Metabolism. Diabetes Care. 2019, 42, 372–380. [Google Scholar] [CrossRef]
- Vounzoulaki, E.; Khunti, K.; Abner, S.C.; Tan, B.K.; Davies, M.J.; Gillies, C.L. Progression to type 2 diabetes in women with a known history of gestational diabetes: systematic review and meta-analysis. BMJ. 2020, 369, 1361. [Google Scholar] [CrossRef] [PubMed]
- Retnakaran, R.; Shah, B.R. Role of Type 2 Diabetes in Determining Retinal, Renal, and Cardiovascular Outcomes in Women With Previous Gestational Diabetes Mellitus. Diabetes Care. 2017, 40, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Bomback, A.S.; Rekhtman, Y.; Whaley-Connell, A.T.; Kshirsagar, A.V.; Sowers, J.R.; Chen, S.C.; Li, S.; Chinnaiyan, K.M.; Bakris, G.L.; McCullough, P.A. Gestational diabetes mellitus alone in the absence of subsequent diabetes is associated with microalbuminuria: results from the Kidney Early Evaluation Program (KEEP). Diabetes Care. 2010, 33, 2586–91. [Google Scholar] [CrossRef]
- Kaiser, K.; Nielsen, M.F.; Kallfa, E.; Dubietyte, G.; Lauszus, F.F. Metabolic syndrome in women with previous gestational diabetes. Sci. Rep. 2021, 11, 11558. [Google Scholar] [CrossRef] [PubMed]
- Kramer, C.K.; Campbell, S.; Retnakaran, R. Gestational diabetes and the risk of cardiovascular disease in women: a systematic review and meta-analysis. Diabetologia. 2019, 62, 905–914. [Google Scholar] [CrossRef]
- Xie, W.; Wang, Y.; Xiao, S.; Qiu, L.; Yu, Y.; Zhang, Z. Association of gestational diabetes mellitus with overall and type specific cardiovascular and cerebrovascular diseases: systematic review and meta-analysis. BMJ. 2022, 378, e070244. [Google Scholar] [CrossRef] [PubMed]
- Galderisi, M.; Cosyns, B.; Edvardsen, T.; Cardim, N.; Delgado, V.; Di Salvo, G.; Donal, E.; Sade, L.E.; Ernande, L.; Garbi, M.; et al. Standardization of adult transthoracic echocardiography reporting in agreement with recent chamber quantification, diastolic function, and heart valve disease recommendations: an expert consensus document of the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging. 2017, 18, 1301–1310. [Google Scholar] [PubMed]
- Potter, E.; Marwick, T.H. Assessment of Left Ventricular Function by Echocardiography: The Case for Routinely Adding Global Longitudinal Strain to Ejection Fraction. JACC Cardiovasc. Imaging. 2018, 11, 260–274. [Google Scholar] [CrossRef] [PubMed]
- Otterstad, J.E.; Froeland, G.; St John Sutton, M.; Holme, I. Accuracy and reproducibility of biplane two-dimensional echocardiographic measurements of left ventricular dimensions and function. Eur. Heart J. 1997, 18, 507–13. [Google Scholar] [CrossRef]
- Marwick, T.H. Ejection Fraction Pros and Cons: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 2360–2379. [Google Scholar] [CrossRef]
- Hoit, B.D. Strain and strain rate echocardiography and coronary artery disease. Circ. Cardiovasc. Imaging. 2011, 4, 179–90. [Google Scholar] [CrossRef]
- Luis, S.A.; Chan, J.; Pellikka, P.A. Echocardiographic Assessment of Left Ventricular Systolic Function: An Overview of Contemporary Techniques, Including Speckle-Tracking Echocardiography. Mayo Clin. Proc. 2019, 94, 125–138. [Google Scholar] [CrossRef] [PubMed]
- Voigt, J.U.; Cvijic, M. 2- and 3-Dimensional Myocardial Strain in Cardiac Health and Disease. JACC Cardiovasc. Imaging. 2019, 12, 1849–1863. [Google Scholar] [CrossRef]
- Meera, S.J.; Ando, T.; Pu, D.; Manjappa, S.; Taub, C.C. Dynamic left ventricular changes in patients with gestational diabetes: A speckle tracking echocardiography study. J. Clin. Ultrasound. 2017, 45, 20–27. [Google Scholar] [CrossRef]
- Buddeberg, B.S.; Sharma, R.; O'Driscoll, J.M.; Kaelin Agten, A.; Khalil, A.; Thilaganathan, B. Impact of gestational diabetes mellitus on maternal cardiac adaptation to pregnancy. Ultrasound Obstet. Gynecol. 2020, 56, 240–246. [Google Scholar] [CrossRef]
- Ye, X.; Li, Z.; Li, Y.; Cai, Q.; Sun, L.; Zhu, W.; Ding, X.; Guo, D.; Qin, Y.; Lu, X. Reduced mechanical function of the left atrial predicts adverse outcome in pregnant women with clustering of metabolic risk factors. BMC Cardiovasc. Disord. 2021, 21, 265. [Google Scholar] [CrossRef] [PubMed]
- Company Calabuig, A.M.; Nunez, E.; Sánchez, A.; Nicolaides, K.H.; Charakida, M.; De Paco Matallana, C. Three-dimensional echocardiography and cardiac strain imaging in women with gestational diabetes mellitus. Ultrasound Obstet. Gynecol. 2021, 58, 278–284. [Google Scholar] [CrossRef]
- Gibbone, E.; Wright, A.; Campos, R.V.; Anzoategui, S.; Nicolaides, K.H.; Charakida, M. Maternal cardiac function at 19-23 weeks' gestation in prediction of gestational diabetes mellitus. Ultrasound Obstet. Gynecol. 2021, 58, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Li, Z.; Liu, W.; Zhao, P.; Che, G.; Wang, X.; Di, Z.; Tian, J.; Sun, L.; Wang, Z. Two-dimensional speckle tracking echocardiography in assessing the subclinical myocardial dysfunction in patients with gestational diabetes mellitus. Cardiovasc. Ultrasound. 2022, 20, 21. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Peng, Y.; Liu, L.; Jiao, R.; Zhang, Y.; Zhao, W.; Liu, Y.; Sun, C. Early Assessment of Cardiac Function by Echocardiography in Patients with Gestational Diabetes Mellitus. Comput. Math. Methods Med. 2022, 2022, 6565109. [Google Scholar] [CrossRef] [PubMed]
- Anzoategui, S.; Gibbone, E.; Wright, A.; Nicolaides, K.H.; Charakida, M. Midgestation cardiovascular phenotype in women who develop gestational diabetes and hypertensive disorders of pregnancy: comparative study. Ultrasound Obstet. Gynecol. 2022, 60, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Sonaglioni, A.; Barlocci, E.; Adda, G.; Esposito, V.; Ferrulli, A.; Nicolosi, G.L.; Bianchi, S.; Lombardo, M.; Luzi, L. The impact of short-term hyperglycemia and obesity on biventricular and biatrial myocardial function assessed by speckle tracking echocardiography in a population of women with gestational diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 456–468. [Google Scholar] [CrossRef] [PubMed]
- Appiah, D.; Schreiner, P.J.; Gunderson, E.P.; Konety, S.H.; Jacobs, D.R. Jr; Nwabuo, C.C.; Ebong, I.A.; Whitham, H.K.; Goff, D.C. Jr; Lima, J.A.; et al. Association of Gestational Diabetes Mellitus With Left Ventricular Structure and Function: The CARDIA Study. Diabetes Care. 2016, 39, 400–7. [Google Scholar] [CrossRef]
- Aguilera, J.; Sanchez Sierra, A.; Abdel Azim, S.; Georgiopoulos, G.; Nicolaides, K.H.; Charakida, M. Maternal cardiac function in gestational diabetes mellitus at 35-36 weeks' gestation and 6 months postpartum. Ultrasound Obstet. Gynecol. 2020, 56, 247–254. [Google Scholar] [CrossRef] [PubMed]
- Benhalima, K.; Lens, K.; Bosteels, J.; Chantal, M. The Risk for Glucose Intolerance after Gestational Diabetes Mellitus since the Introduction of the IADPSG Criteria: A Systematic Review and Meta-Analysis. J. Clin. Med. 2019, 8, 1431. [Google Scholar] [CrossRef]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–70. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39.e14. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F. 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef]
- Humbert, M.; Kovacs, G.; Hoeper, M.M.; Badagliacca, R.; Berger, R.M.F.; Brida, M.; Carlsen, J.; Coats, A.J.S.; Escribano-Subias, P.; Ferrari, P.; et al. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension. Eur. Respir. J. 2023, 61, 2200879. [Google Scholar] [CrossRef] [PubMed]
- Tello, K.; Wan, J.; Dalmer, A.; Vanderpool, R.; Ghofrani, H.A.; Naeije, R.; Roller, F.; Mohajerani, E.; Seeger, W.; Herberg, U.; et al. Validation of the Tricuspid Annular Plane Systolic Excursion/Systolic Pulmonary Artery Pressure Ratio for the Assessment of Right Ventricular-Arterial Coupling in Severe Pulmonary Hypertension. Circ. Cardiovasc. Imaging. 2019, 12, e009047. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, R.A.; Otto, C.M.; Bonow, R.O.; Carabello, B.A.; Erwin, J.P. 3rd; Fleisher, L.A.; Jneid, H.; Mack, M.J.; McLeod, C.J.; O'Gara, P.T.; et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2017, 135, e1159–e1195. [Google Scholar] [CrossRef] [PubMed]
- Iacobellis, G.; Willens, H.J.; Barbaro, G.; Sharma, A.M. Threshold values of high-risk echocardiographic epicardial fat thickness. Obesity (Silver Spring). 2008, 16, 887–92. [Google Scholar] [CrossRef]
- Zheng, L.; Sun, Z.; Li, J.; Zhang, R.; Zhang, X.; Liu, S.; Li, J.; Xu, C.; Hu, D.; Sun, Y. Pulse pressure and mean arterial pressure in relation to ischemic stroke among patients with uncontrolled hypertension in rural areas of China. Stroke. 2008, 39, 1932–7. [Google Scholar] [CrossRef] [PubMed]
- Sattin, M.; Burhani, Z.; Jaidka, A.; Millington, S.J.; Arntfield, R.T. Stroke Volume Determination by Echocardiography. Chest. 2022, 161, 1598–1605. [Google Scholar] [CrossRef] [PubMed]
- Hill, L.K.; Sollers Iii, J.J.; Thayer, J.F. Resistance reconstructed estimation of total peripheral resistance from computationally derived cardiac output - biomed 2013. Biomed. Sci. Instrum. 2013, 49, 216–23. [Google Scholar]
- Redfield, M.M.; Jacobsen, S.J.; Borlaug, B.A.; Rodeheffer, R.J.; Kass, D.A. Age- and gender-related ventricular-vascular stiffening: a community-based study. Circulation. 2005, 112, 2254–62. [Google Scholar] [CrossRef] [PubMed]
- Chantler, P.D.; Lakatta, E.G.; Najjar, S.S. Arterial-ventricular coupling: mechanistic insights into cardiovascular performance at rest and during exercise. J. Appl. Physiol. (1985). 2008, 105, 1342–51. [Google Scholar] [CrossRef]
- Voigt, J.U.; Pedrizzetti, G.; Lysyansky, P.; Marwick, T.H.; Houle, H.; Baumann, R.; Pedri, S.; Ito, Y.; Abe, Y.; Metz, S.; et al. Definitions for a common standard for 2D speckle tracking echocardiography: consensus document of the EACVI/ASE/Industry Task Force to standardize deformation imaging. Eur. Heart J. Cardiovasc. Imaging. 2015, 16, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Badano, L.P. , Muraru, D., Parati, G., Haugaa, K., Voigt, J.U. How to do right ventricular strain. Eur. Heart J. Cardiovasc. Imaging. 2020, 21, 825–827. [Google Scholar] [CrossRef] [PubMed]
- Voigt, J.U.; Mălăescu, G.G.; Haugaa, K.; Badano, L. How to do LA strain. Eur. Heart J. Cardiovasc. Imaging. 2020, 21, 715–717. [Google Scholar] [CrossRef] [PubMed]
- Sonaglioni, A.; Vincenti, A.; Baravelli, M.; Rigamonti, E.; Tagliabue, E.; Bassi, P.; Nicolosi, G.L.; Anzà, C.; Lombardo, M. Prognostic value of global left atrial peak strain in patients with acute ischemic stroke and no evidence of atrial fibrillation. Int. J. Cardiovasc. Imaging. 2019, 35, 603–613. [Google Scholar] [CrossRef] [PubMed]
- Yingchoncharoen, T.; Agarwal, S.; Popović, Z.B.; Marwick, T.H. Normal ranges of left ventricular strain: a meta-analysis. J. Am. Soc. Echocardiogr. 2013, 26, 185–91. [Google Scholar] [CrossRef]
- Muraru, D.; Onciul, S.; Peluso, D.; Soriani, N.; Cucchini, U.; Aruta, P.; Romeo, G.; Cavalli, G.; Iliceto, S.; Badano, L.P. Sex- and Method-Specific Reference Values for Right Ventricular Strain by 2-Dimensional Speckle-Tracking Echocardiography. Circ. Cardiovasc. Imaging. 2016, 9, e003866. [Google Scholar] [CrossRef] [PubMed]
- Pathan, F.; D'Elia, N.; Nolan, M.T.; Marwick, T.H.; Negishi, K. Normal Ranges of Left Atrial Strain by Speckle-Tracking Echocardiography: A Systematic Review and Meta-Analysis. J. Am. Soc. Echocardiogr. 2017, 30, 59–70.e8. [Google Scholar] [CrossRef] [PubMed]
- Krittanawong, C.; Maitra, N.S.; Hassan Virk, H.U.; Farrell, A.; Hamzeh, I.; Arya, B.; Pressman, G.S.; Wang, Z.; Marwick, T.H. Normal Ranges of Right Atrial Strain: A Systematic Review and Meta-Analysis. JACC Cardiovasc. Imaging. 2023, 16, 282–294. [Google Scholar] [CrossRef]
- Stein, J.H.; Korcarz, C.E.; Hurst, R.T.; Lonn, E.; Kendall, C.B.; Mohler, E.R.; Najjar, S.S.; Rembold, C.M.; Post, W.S.; American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: a consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J. Am. Soc. Echocardiogr. 2008, 21, 93–111, quiz 189-90. [Google Scholar]
- Lorenz, M.W.; von Kegler, S.; Steinmetz, H.; Markus, H.S.; Sitzer, M. Carotid intima-media thickening indicates a higher vascular risk across a wide age range: prospective data from the Carotid Atherosclerosis Progression Study (CAPS). Stroke. 2006, 37, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Randrianarisoa, E.; Rietig, R.; Jacob, S.; Blumenstock, G.; Haering, H.U.; Rittig, K.; Balletshofer, B. Normal values for intima-media thickness of the common carotid artery--an update following a novel risk factor profiling. Vasa. 2015, 44, 444–50. [Google Scholar] [CrossRef]
- Sullivan, S.D.; Umans, J.G.; Ratner, R. Gestational diabetes: implications for cardiovascular health. Curr. Diab. Rep. 2012, 12, 43–52. [Google Scholar] [CrossRef]
- Gunderson, E.P.; Chiang, V.; Pletcher, M.J.; Jacobs, D.R.; Quesenberry, C.P.; Sidney, S.; Lewis, C.E. History of gestational diabetes mellitus and future risk of atherosclerosis in mid-life: the Coronary Artery Risk Development in Young Adults study. J. Am. Heart Assoc. 2014, 3, e000490. [Google Scholar] [CrossRef] [PubMed]
- McKenzie-Sampson, S.; Paradis, G.; Healy-Profitós, J.; St-Pierre, F.; Auger, N. Gestational diabetes and risk of cardiovascular disease up to 25 years after pregnancy: a retrospective cohort study. Acta Diabetol. 2018, 55, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.J.; Kim, H.L.; Lim, W.H.; Seo, J.B.; Kim, S.H.; Zo, J.H.; Kim, M.A. Subclinical alterations in left ventricular structure and function according to obesity and metabolic health status. PLoS One. 2019, 14, e0222118. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Liang, J.; Zheng, S.; He, A.; Chen, C.; Zhao, X.; Hua, M.; Xu, J.; Zheng, Z.; Liu, M. Combined associations of obesity and metabolic health with subclinical left ventricular dysfunctions: Danyang study. ESC Heart Fail. 2021, 8, 3058–3069. [Google Scholar] [CrossRef]
- Vitarelli, A.; Martino, F.; Capotosto, L.; Martino, E.; Colantoni, C.; Ashurov, R.; Ricci, S.; Conde, Y.; Maramao, F.; Vitarelli, M.; et al. Early myocardial deformation changes in hypercholesterolemic and obese children and adolescents: a 2D and 3D speckle tracking echocardiography study. Medicine (Baltimore). 2014, 93, e71. [Google Scholar] [CrossRef]
- Kim, S.A.; Park, S.M.; Kim, M.N.; Shim, W.J. Assessment of Left Ventricular Function by Layer-Specific Strain and Its Relationship to Structural Remodelling in Patients With Hypertension. Can. J. Cardiol. 2016, 32, 211–6. [Google Scholar] [CrossRef]
- Kosmala, W.; Sanders, P.; Marwick, T.H. Subclinical Myocardial Impairment in Metabolic Diseases. JACC Cardiovasc. Imaging. 2017, 10, 692–703. [Google Scholar] [CrossRef]
- Pandey, A.; Patel, K.V.; Vaduganathan, M.; Sarma, S.; Haykowsky, M.J.; Berry, J.D.; Lavie, C.J. Physical Activity, Fitness, and Obesity in Heart Failure With Preserved Ejection Fraction. JACC Heart Fail. 2018, 6, 975–982. [Google Scholar] [CrossRef]
- Fazio, S.; Mercurio, V.; Fazio, V.; Ruvolo, A.; Affuso, F. Insulin Resistance/Hyperinsulinemia, Neglected Risk Factor for the Development and Worsening of Heart Failure with Preserved Ejection Fraction. Biomedicines. 2024, 12, 806. [Google Scholar] [CrossRef]
- Volpe, L.; Cuccuru, I.; Lencioni, C.; Napoli, V.; Ghio, A.; Fotino, C.; Bertolotto, A.; Penno, G.; Benzi, L.; Del Prato, S.; et al. Early subclinical atherosclerosis in women with previous gestational diabetes mellitus. Diabetes Care. 2008, 31, e32. [Google Scholar] [CrossRef] [PubMed]
- Freire, C.M.; Barbosa, F.B.; de Almeida, M.C.; Miranda, P.A.; Barbosa, M.M.; Nogueira, A.I.; Guimarães, M.M.; Nunes Mdo, C.; Ribeiro-Oliveira, A. Jr. Previous gestational diabetes is independently associated with increased carotid intima-media thickness, similarly to metabolic syndrome - a case control study. Cardiovasc. Diabetol. 2012, 11, 59. [Google Scholar] [CrossRef] [PubMed]
- Fakhrzadeh, H.; Alatab, S.; Sharifi, F.; Mirarefein, M.; Badamchizadeh, Z.; Ghaderpanahi, M.; Hashemi Taheri, A.P.; Larijani, B. Carotid intima media thickness, brachial flow mediated dilation and previous history of gestational diabetes mellitus. J. Obstet. Gynaecol. Res. 2012, 38, 1057–63. [Google Scholar] [CrossRef]
- Karoli, R.; Siddiqi, Z.; Fatima, J.; Shukla, V.; Mishra, P.P.; Khan, F.A. Assessment of noninvasive risk markers of subclinical atherosclerosis in premenopausal women with previous history of gestational diabetes mellitus. Heart Views. 2015, 16, 13–8. [Google Scholar] [CrossRef] [PubMed]
- Frigerio, B.; Werba, J.P.; Amato, M.; Ravani, A.; Sansaro, D.; Coggi, D.; Vigo, L.; Tremoli, E.; Baldassarre, D. Traditional Risk Factors are Causally Related to Carotid Intima-Media Thickness Progression: Inferences from Observational Cohort Studies and Interventional Trials. Curr. Pharm Des. 2020, 26, 11–24. [Google Scholar] [CrossRef] [PubMed]
- Kornev, M.; Caglayan, H.A.; Kudryavtsev, A.V.; Malyutina, S.; Ryabikov, A.; Schirmer, H.; Rösner, A. Influence of hypertension on systolic and diastolic left ventricular function including segmental strain and strain rate. Echocardiography. 2023, 40, 623–633. [Google Scholar] [CrossRef] [PubMed]
- Sonaglioni, A.; Esposito, V.; Caruso, C.; Nicolosi, G.L.; Bianchi, S.; Lombardo, M.; Gensini, G.F.; Ambrosio, G. Chest conformation spuriously influences strain parameters of myocardial contractile function in healthy pregnant women. J. Cardiovasc. Med. (Hagerstown). 2021, 22, 767–779. [Google Scholar] [CrossRef] [PubMed]
- Sonaglioni, A.; Ferrulli, A.; Nicolosi, G.L.; Lombardo, M.; Luzi, L. The Influence of Anthropometrics on Cardiac Mechanics in Healthy Women With Opposite Obesity Phenotypes (Android vs Gynoid). Cureus. 2024, 16, e51698. [Google Scholar] [CrossRef] [PubMed]
- ACOG Practice Bulletin, No. 190: Gestational Diabetes Mellitus. Obstet. Gynecol. 2018, 131, e49–e64. [Google Scholar]
- American Diabetes Association Professional Practice Committee. 15. Management of Diabetes in Pregnancy: Standards of Medical Care in Diabetes-2022. Diabetes Care. 2022, 45, S232–S243. [Google Scholar] [CrossRef] [PubMed]
- Sitzberger, C.; Oberhoffer-Fritz, R.; Meyle, K.; Wagner, M.; Lienert, N.; Graupner, O.; Ensenauer, R.; Lobmaier, S.M.; Wacker-Gußmann, A. Gestational Diabetes: Physical Activity Before Pregnancy and Its Influence on the Cardiovascular System. Front. Pediatr. 2020, 8, 465. [Google Scholar] [CrossRef]
- D'Ascenzo, F.; Agostoni, P.; Abbate, A.; Castagno, D.; Lipinski, M.J.; Vetrovec, G.W.; Frati, G.; Presutti, D.G.; Quadri, G.; Moretti, C.; et al. Atherosclerotic coronary plaque regression and the risk of adverse cardiovascular events: a meta-regression of randomized clinical trials. Atherosclerosis. 2013, 226, 178–85. [Google Scholar] [CrossRef]
- Negishi, T.; Negishi, K.; Thavendiranathan, P.; Cho, G.Y.; Popescu, B.A.; Vinereanu, D.; Kurosawa, K.; Penicka, M.; Marwick, T.H.; SUCCOUR Investigators. Effect of Experience and Training on the Concordance and Precision of Strain Measurements. JACC Cardiovasc. Imaging. 2017, 5, 518–522. [Google Scholar] [CrossRef]
- Rösner, A.; Barbosa, D.; Aarsæther, E.; Kjønås, D.; Schirmer, H.; D'hooge, J. The influence of frame rate on two-dimensional speckle-tracking strain measurements: a study on silico-simulated models and images recorded in patients. Eur. Heart J. Cardiovasc. Imaging. 2015, 16, 1137–47. [Google Scholar] [CrossRef] [PubMed]
- Mirea, O.; Pagourelias, E.D.; Duchenne, J.; Bogaert, J.; Thomas, J.D.; Badano, L.P.; Voigt, J.U.; EACVI-ASE-Industry Standardization Task Force. Intervendor Differences in the Accuracy of Detecting Regional Functional Abnormalities: A Report From the EACVI-ASE Strain Standardization Task Force. JACC Cardiovasc. Imaging. 2018, 11, 25–34. [Google Scholar] [CrossRef]
- Sonaglioni, A.; Nicolosi, G.L.; Granato, A.; Bonanomi, A.; Rigamonti, E.; Lombardo, M. Influence of chest wall conformation on reproducibility of main echocardiographic indices of left ventricular systolic function. Minerva Cardiol. Angiol. 2024, 72, 111–124. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Representative examples of biventricular and biatrial longitudinal strain parameters measured from the apical four-chamber view in a pGDM woman included in the present study. All myocardial strain parameters are reduced in comparison to the accepted reference ranges. GLS, global longitudinal strain; LASr, left atrial reservoir strain; LV, left ventricular; pGDM, previous gestational diabetes mellitus; RASr, right atrial reservoir strain; RV, right ventricular.
Figure 1.
Representative examples of biventricular and biatrial longitudinal strain parameters measured from the apical four-chamber view in a pGDM woman included in the present study. All myocardial strain parameters are reduced in comparison to the accepted reference ranges. GLS, global longitudinal strain; LASr, left atrial reservoir strain; LV, left ventricular; pGDM, previous gestational diabetes mellitus; RASr, right atrial reservoir strain; RV, right ventricular.
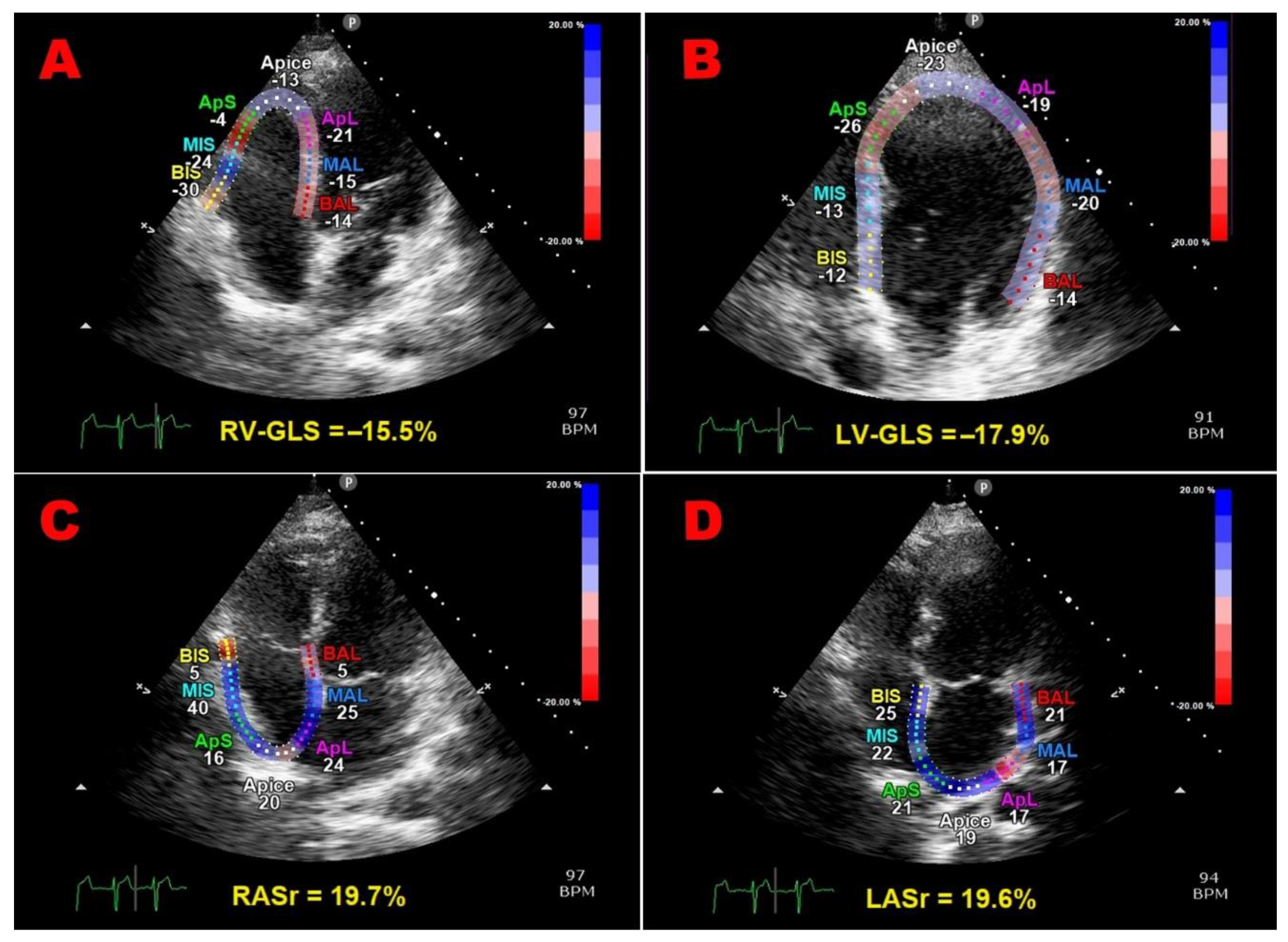
Figure 2.
ROC curve analysis performed to establish the sensitivity and the specificity of third trimester BMI (A) and third trimester glycosylated hemoglobin (B) for predicting the primary endpoint. AUC, area under curve; BMI, body mass index; ROC, receiver operating characteristics.
Figure 2.
ROC curve analysis performed to establish the sensitivity and the specificity of third trimester BMI (A) and third trimester glycosylated hemoglobin (B) for predicting the primary endpoint. AUC, area under curve; BMI, body mass index; ROC, receiver operating characteristics.

Figure 3.
Representative examples of LV-GLS bull's-eye plots obtained in a pGDM women with previous pregnancy complicated by obesity and uncontrolled diabetes (A) and in a woman with previous uncomplicated pregnancy (B), respectively. The pGDM woman (A) showed a moderate impairment of LV-GLS; the blue zones observed in the bull’s eye plot indicated the lowest magnitude of myocardial deformation. Conversely, in the woman with previous uncomplicated pregnancy (B), the uniformly red pattern of the bull’s eye plot suggested normal myocardial deformation properties. GLS, global longitudinal strain; LV, left ventricular; pGDM, previous gestational diabetes mellitus.
Figure 3.
Representative examples of LV-GLS bull's-eye plots obtained in a pGDM women with previous pregnancy complicated by obesity and uncontrolled diabetes (A) and in a woman with previous uncomplicated pregnancy (B), respectively. The pGDM woman (A) showed a moderate impairment of LV-GLS; the blue zones observed in the bull’s eye plot indicated the lowest magnitude of myocardial deformation. Conversely, in the woman with previous uncomplicated pregnancy (B), the uniformly red pattern of the bull’s eye plot suggested normal myocardial deformation properties. GLS, global longitudinal strain; LV, left ventricular; pGDM, previous gestational diabetes mellitus.
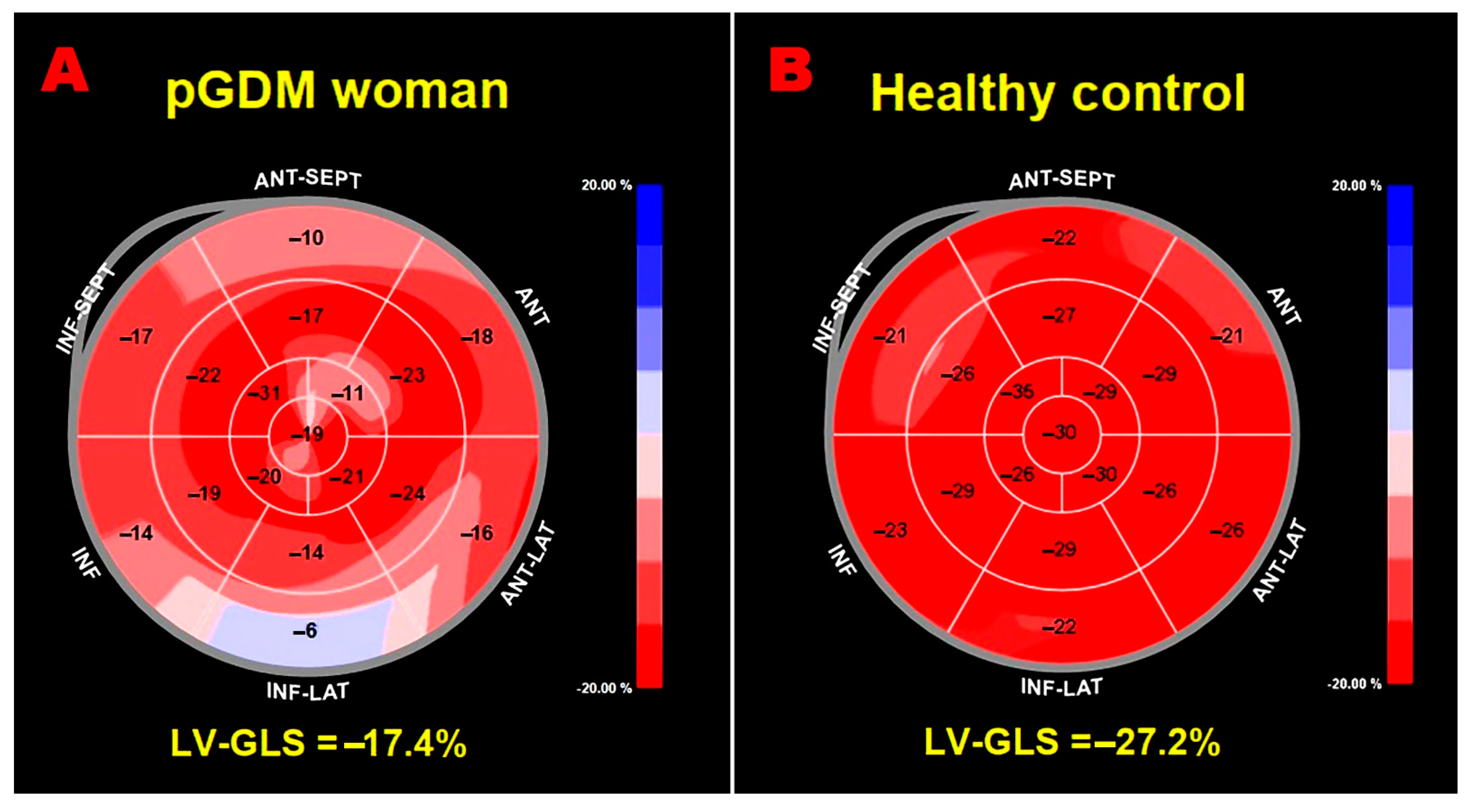
Figure 4.
ROC curve analysis performed to establish the sensitivity and the specificity of third trimester BMI (A) and third trimester glycosylated hemoglobin (B) for predicting the secondary endpoint. AUC, area under curve; BMI, body mass index; ROC, receiver operating characteristics.
Figure 4.
ROC curve analysis performed to establish the sensitivity and the specificity of third trimester BMI (A) and third trimester glycosylated hemoglobin (B) for predicting the secondary endpoint. AUC, area under curve; BMI, body mass index; ROC, receiver operating characteristics.
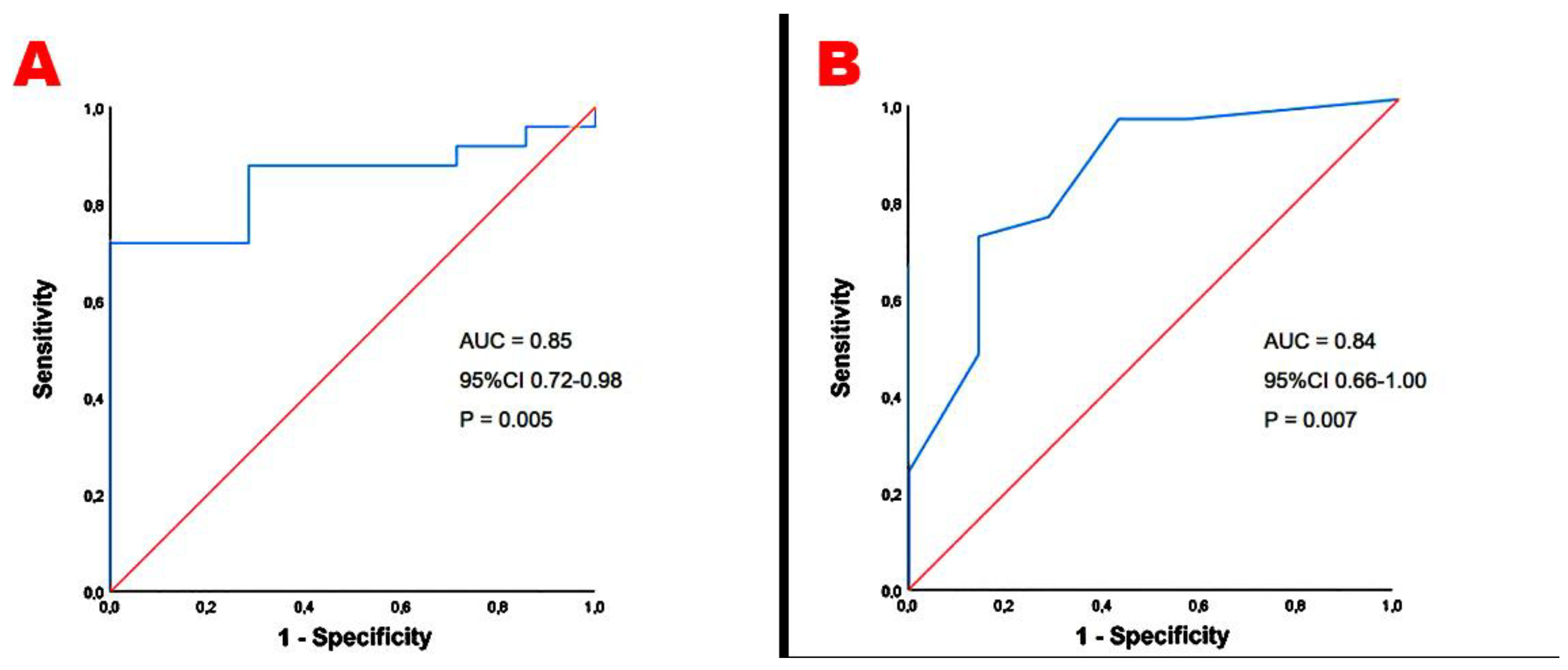

Table 1.
Clinical, obstetrical, hemodynamic and laboratory parameters collected in GDM women and controls at the third trimester of pregnancy. Data are expressed as mean ± SD or as number (percentage). Significant p-values are in bold. BMI, body mass index; BSA, body surface area; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; GDM, gestational diabetes mellitus; HR, heart rate; MAP, mean arterial pressure; NLR, neutrophil-to-lymphocyte ratio; PPH, postpartum hemorrhage; PROM, premature rupture of membranes; RDW, red blood cells distribution width; SBP, systolic blood pressure.
Table 1.
Clinical, obstetrical, hemodynamic and laboratory parameters collected in GDM women and controls at the third trimester of pregnancy. Data are expressed as mean ± SD or as number (percentage). Significant p-values are in bold. BMI, body mass index; BSA, body surface area; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; GDM, gestational diabetes mellitus; HR, heart rate; MAP, mean arterial pressure; NLR, neutrophil-to-lymphocyte ratio; PPH, postpartum hemorrhage; PROM, premature rupture of membranes; RDW, red blood cells distribution width; SBP, systolic blood pressure.
| GDM women (n = 32) | Controls (n = 30) | p-Value | |
|---|---|---|---|
| Demographics, anthropometrics and obstetrics | |||
| Age (yrs) | 34.1 ± 6.5 | 35.8 ± 5.0 | 0.26 |
| Caucasian ethnicity (%) | 16 (50.0) | 19 (63.3) | 0.29 |
| Third trimester BSA (m2) | 1.86 ± 0.19 | 1.77 ± 0.15 | 0.04 |
| Third trimester BMI (Kg/m2) | 29.5 ± 6.0 | 26.6 ± 3.8 | 0.03 |
| Obesity (BMI ≥30 Kg/m2) (%) | 14 (43.7) | 5 (16.7) | 0.02 |
| Pluriparous (%) | 16 (50.0) | 13 (43.3) | 0.59 |
| Gestational age (weeks) | 36.2 ± 1.8 | 36.6 ± 1.5 | 0.35 |
| Cardiovascular risk factors | |||
| Smoking (%) | 5 (15.6) | 6 (20.0) | 0.65 |
| Dyslipidemia (%) | 16 (50.0) | 5 (16.7) | 0.005 |
| Family history of diabetes (%) | 16 (50.0) | 3 (10.0) | <0.001 |
| Hemodynamics | |||
| HR (bpm) | 86.8 ± 14.9 | 88.3 ± 8.8 | 0.63 |
| SBP (mmHg) | 108.8 ± 11.3 | 92.5 ± 8.6 | <0.001 |
| DBP (mmHg) | 68.0 ± 7.0 | 59.3 ± 4.5 | <0.001 |
| MAP (mmHg) | 81.6 ± 7.1 | 70.4 ± 5.5 | <0.001 |
| Third trimester blood tests and glycometabolic parameters | |||
| Serum hemoglobin (g/dl) | 11.7 ± 1.1 | 11.3 ± 1.5 | 0.23 |
| RDW (%) | 15.3 ± 2.4 | 13.8 ± 2.1 | 0.01 |
| NLR | 4.4 ± 1.7 | 2.1 ± 0.5 | <0.001 |
| eGFR (ml/min/m2) | 128.3 ± 12.6 | 133.6 ± 28.9 | 0.35 |
| Serum total cholesterol (mg/dl) | 253.75 ± 36.6 | 171.0 ± 11.2 | <0.001 |
| Serum uric acid (mg/dl) | 4.9 ± 1.1 | 4.2 ± 0.6 | 0.003 |
| Gestational age at diagnosis of GDM (weeks) | 24.0 ± 5.8 | / | / |
| Glycosylated hemoglobin (mmol/mol) | 34.7 ± 4.1 | / | / |
| Antidiabetic treatment | |||
| Diet (%) | 18 (56.2) | / | / |
| Insulin (%) | 14 (43.8) | / | / |
| Delivery parameters | |||
| Gestational week at delivery (weeks) | 38.4 ± 0.9 | 39.1 ± 1.4 | 0.02 |
| PROM (%) | 3 (9.4) | 1 (3.3) | 0.33 |
| Cesarean delivery (%) | 8 (25.0) | 10 (33.3) | 0.47 |
| PPH (%) | 2 (6.2) | 3 (10.0) | 0.59 |
| Neonatal birth weight (g) | 3361.2 ± 292.6 | 3381.2 ± 480.5 | 0.84 |
Table 2.
Clinical characteristics of the two study groups at 4 years postpartum. Data are expressed as mean ± SD or as number (percentage). Significant p-values are in bold. BMI, body mass index; BP, blood pressure; BSA, body surface area; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; MAP, mean arterial pressure; pGDM, previous gestational diabetes mellitus; SBP, systolic blood pressure; WHR, waist to hip ratio.
Table 2.
Clinical characteristics of the two study groups at 4 years postpartum. Data are expressed as mean ± SD or as number (percentage). Significant p-values are in bold. BMI, body mass index; BP, blood pressure; BSA, body surface area; DBP, diastolic blood pressure; eGFR, estimated glomerular filtration rate; MAP, mean arterial pressure; pGDM, previous gestational diabetes mellitus; SBP, systolic blood pressure; WHR, waist to hip ratio.
| pGDM women (n = 32) | Controls (n = 30) | p-Value | |
|---|---|---|---|
| Demographics and anthropometrics | |||
| Age (yrs) | 39.1 ± 6.5 | 40.8 ± 5.0 | 0.26 |
| Caucasian ethnicity (%) | 16 (50.0) | 19 (63.3) | 0.29 |
| BSA (m2) | 1.76 ± 0.17 | 1.66 ± 0.14 | 0.01 |
| BMI (Kg/m2) | 27.9 ± 4.5 | 22.2 ± 2.8 | <0.001 |
| Obesity (BMI ≥30 Kg/m2) (%) | 11 (34.4) | 3 (10.0) | 0.02 |
| WHR | 0.90 ± 0.16 | 0.78 ± 0.15 | 0.003 |
| Cardiovascular risk factors | |||
| Smoking (%) | 5 (15.6) | 6 (20.0) | 0.65 |
| Type 2 diabetes mellitus (%) | 10 (31.2) | 1 (3.3) | 0.004 |
| Dyslipidemia (%) | 10 (31.2) | 2 (6.7) | 0.01 |
| Blood pressure parameters | |||
| SBP (mmHg) | 122.4 ± 13.2 | 113.2 ± 11.1 | 0.004 |
| DBP (mmHg) | 76.2 ± 9.1 | 70.4 ± 9.4 | 0.02 |
| MBP (mmHg) | 91.6 ± 9.6 | 84.6 ± 8.9 | 0.04 |
| BP ≥140/90 mmHg at clinical visit (%) | 10 (31.2) | 2 (6.7) | 0.01 |
| Comorbidities | |||
| Hypothyroidism (%) | 3 (9.4) | 8 (26.7) | 0.07 |
| Current medical treatment | |||
| Oral hypoglycemic agents (%) | 4 (12.5) | 1 (3.3) | 0.18 |
| Antihypertensive drugs (%) | 4 (12.5) | 1 (3.3) | 0.18 |
| Statins (%) | 2 (6.2) | 1 (3.3) | 0.59 |
Table 3.
Morphological, functional and hemodynamic parameters assessed by conventional transthoracxic echocardiography and carotid ultrasonography in the two groups of women at the 4-year postpartum. Data are expressed as mean ± SD or as number (percentage). Significant p-values are in bold. A-P, antero-posterior; CCA, common carotid artery; COi, cardiac output indexed; CSA, cross-sectional area; EAT, epicardial adipose tissue; EaI, arterial elastance indexed; EDD, end-diastolic diameter; EesI, end-systolic elastance indexed; ESP, end-systolic pressure; IMT, intima-media thickness; IVC, inferior vena cava; IVS, interventricular septum; LA, left atrial; LAVi, left atrial volume indexed; LV, left ventricular; LVEDD, left ventricular end-diastolic diameter; LVEDVi, left ventricular end-diastolic volume indexed; LVESVi, left ventricular end-systolic volume indexed; MR, mitral regurgitation; pGDM, previous gestational diabetes mellitus; PW, posterior wall; RVIT, right ventricular inflow tract; RWT, relative wall thickness; sPAP, systolic pulmonary artery pressure; SVi, stroke volume indexed; TAPSE, tricuspid annular plane systolic excursion; TPRi, total peripheral resistance index; TR, tricuspid regurgitation.
Table 3.
Morphological, functional and hemodynamic parameters assessed by conventional transthoracxic echocardiography and carotid ultrasonography in the two groups of women at the 4-year postpartum. Data are expressed as mean ± SD or as number (percentage). Significant p-values are in bold. A-P, antero-posterior; CCA, common carotid artery; COi, cardiac output indexed; CSA, cross-sectional area; EAT, epicardial adipose tissue; EaI, arterial elastance indexed; EDD, end-diastolic diameter; EesI, end-systolic elastance indexed; ESP, end-systolic pressure; IMT, intima-media thickness; IVC, inferior vena cava; IVS, interventricular septum; LA, left atrial; LAVi, left atrial volume indexed; LV, left ventricular; LVEDD, left ventricular end-diastolic diameter; LVEDVi, left ventricular end-diastolic volume indexed; LVESVi, left ventricular end-systolic volume indexed; MR, mitral regurgitation; pGDM, previous gestational diabetes mellitus; PW, posterior wall; RVIT, right ventricular inflow tract; RWT, relative wall thickness; sPAP, systolic pulmonary artery pressure; SVi, stroke volume indexed; TAPSE, tricuspid annular plane systolic excursion; TPRi, total peripheral resistance index; TR, tricuspid regurgitation.
| pGDM women (n = 32) | Controls (n = 30) | p-Value | |
|---|---|---|---|
| Yrs postpartum | 4.0 ± 1.9 | 4.1 ± 2.1 | 0.84 |
| Conventional echoDoppler parameters | |||
| IVS (mm) | 9.3 ± 1.8 | 7.6 ± 1.2 | <0.001 |
| LV-PW (mm) | 7.6 ± 0.9 | 6.6 ± 1.0 | <0.001 |
| LV-EDD (mm) | 44.0 ± 3.4 | 44.4 ± 2.7 | 0.61 |
| RWT | 0.34 ± 0.05 | 0.30 ± 0.05 | 0.003 |
| LVMi (g/m2) | 66.7 ± 10.9 | 57.7 ± 9.7 | 0.001 |
| Normal LV geometric pattern (%) | 29 (90.6) | 29 (96.7) | 0.33 |
| LV concentric remodeling (%) | 3 (9.4) | 1 (3.3) | 0.33 |
| LVEDVi (ml/m2) | 34.9 ± 6.15 | 35.3 ± 5.6 | 0.79 |
| LVESVi (ml/m2) | 11.8 ± 2.6 | 11.9 ± 2.5 | 0.88 |
| LVEF (%) | 65.8 ± 3.7 | 65.9 ± 4.8 | 0.93 |
| E/A ratio | 1.24 ± 0.31 | 1.34 ± 0.31 | 0.21 |
| E/average e’ ratio | 9.25 ± 3.01 | 5.14 ± 1.34 | <0.001 |
| LA A-P diameter (mm) | 36.2 ± 3.3 | 33.6 ± 4.1 | 0.008 |
| LAVi (ml/m2) | 29.0 ± 7.3 | 27.4 ± 7.3 | 0.39 |
| Mild MR (n, %) | 7 (21.9) | 9 (30.0) | 0.46 |
| Mild TR (n, %) | 8 (25) | 10 (33.3) | 0.47 |
| RVIT (mm) | 29.7 ± 2.6 | 29.5 ± 3.0 | 0.78 |
| TAPSE (mm) | 23.9 ± 3.7 | 26.4 ± 3.6 | 0.009 |
| IVC (mm) | 16.6 ± 3.6 | 17.0 ± 3.9 | 0.68 |
| sPAP (mmHg) | 25.0 ± 4.9 | 22.8 ± 2.2 | 0.03 |
| TAPSE/sPAP ratio | 0.97 ± 0.19 | 1.17 ± 0.18 | <0.001 |
| Aortic root (mm) | 29.0 ± 3.4 | 29.1 ± 2.6 | 0.89 |
| Ascending aorta (mm) | 28.9 ± 3.4 | 28.8 ± 3.1 | 0.90 |
| End-systolic EAT (mm) | 6.7 ± 1.3 | 4.1 ± 1.4 | <0.001 |
| Hemodynamic indices | |||
| HR (bpm) | 77.6 ± 11.1 | 75.5 ± 11.9 | 0.46 |
| ESP (mmHg) | 110.2 ± 11.9 | 101.9 ± 10.0 | 0.004 |
| SVi (ml/m2) | 32.2 ± 6.1 | 39.4 ± 9.1 | <0.001 |
| COi (l/min/m2) | 2.5 ± 0.4 | 2.9 ± 0.7 | 0.007 |
| TPRi (dyne.sec/cm5)/m2 | 3060.7 ± 669.6 | 2427.5 ± 620.6 | <0.001 |
| EaI (mmHg/ml/m2) | 1.24 ± 0.48 | 1.00 ± 0.26 | 0.02 |
| EesI (mmHg/ml/m2) | 3.25 ± 1.07 | 3.28 ± 0.89 | 0.91 |
| EaI/EesI ratio | 0.39 ± 0.10 | 0.31 ± 0.09 | 0.001 |
| Carotid parameters | |||
| Av. CCA-EDD (mm) | 6.76 ± 0.46 | 6.64 ± 0.44 | 0.29 |
| Av. CCA-IMT (mm) | 0.91 ± 0.26 | 0.62 ± 0.19 | <0.001 |
| Av. CCA-IMT ≥0.7 mm (%) | 25 (78.1) | 7 (23.3) | <0.001 |
| Av. CCA-RWT | 0.27 ± 0.08 | 0.19 ± 0.06 | <0.001 |
| Av. CCA-CSA (mm2) | 22.0 ± 7.4 | 14.2 ± 4.9 | <0.001 |
Table 4.
Biventricular and biatrial strain parameters measured by speckle tracking echocardiography in the two study groups at the 4-year postpartum. Data are expressed as mean ± SD or as number (percentage). Significant p-values are in bold. FWLS, free wall longitudinal strain; GCS, global circumferential strain; GCSR, global circumferential strain rate; GLS, global longitudinal strain; GLSR, global longitudinal strain rate; GSR+, positive global strain rate; GSRE, global early-diastolic strain rate; GSRL, global late-diastolic strain rate; LAScd, left atrial conduit strain; LASct, left atrial contractile strain; LASr, left atrial reservoir strain; LV, left ventricular; pGDM, previous gestational diabetes mellitus; RAScd, right atrial conduit strain; RASct, right atrial contractile strain; RASr, right atrial reservoir strain; RV, right ventricular.
Table 4.
Biventricular and biatrial strain parameters measured by speckle tracking echocardiography in the two study groups at the 4-year postpartum. Data are expressed as mean ± SD or as number (percentage). Significant p-values are in bold. FWLS, free wall longitudinal strain; GCS, global circumferential strain; GCSR, global circumferential strain rate; GLS, global longitudinal strain; GLSR, global longitudinal strain rate; GSR+, positive global strain rate; GSRE, global early-diastolic strain rate; GSRL, global late-diastolic strain rate; LAScd, left atrial conduit strain; LASct, left atrial contractile strain; LASr, left atrial reservoir strain; LV, left ventricular; pGDM, previous gestational diabetes mellitus; RAScd, right atrial conduit strain; RASct, right atrial contractile strain; RASr, right atrial reservoir strain; RV, right ventricular.
| STE VARIABLES | pGDM women (n = 32) | Controls (n = 30) | p-Value |
|---|---|---|---|
| LV-GLS (%) | 19.5 ± 2.6 | 22.3 ± 2.3 | <0.001 |
| LV-GLSR (s-1) | 1.1 ± 0.1 | 1.2 ± 0.1 | <0.001 |
| LV-GCS (%) | 22.8 ± 4.48 | 26.7 ± 4.4 | 0.001 |
| LV-GCSR (s-1) | 1.6 ± 0.3 | 1.7 ± 0.2 | 0.13 |
| LAScd (%) | 29.8 ± 8.9 | 36.3 ± 7.7 | 0.003 |
| LASct (%) | 7.3 ± 4.2 | 9.5 ± 4.1 | 0.04 |
| LASr (%) | 37.1 ± 9.2 | 45.7 ± 8,0 | <0.001 |
| LASr/E/e’ | 4.4 ± 1.8 | 9.5 ± 3.2 | <0.001 |
| LA-GSR (s-1) | 1.9 ± 0.5 | 2.3 ± 0.5 | 0.002 |
| LA-GSRE (s-1) | 2.4 ± 0.7 | 3.1 ± 0.8 | <0.001 |
| LA-GSRL (s-1) | 2.5 ± 0.6 | 2.8 ± 0.5 | 0.04 |
| RV-FWLS (%) | 19.9 ± 3.8 | 22.0 ± 3.5 | 0.03 |
| RV-GLS (%) | 18.8 ± 3.9 | 20.9 ± 3.4 | 0.03 |
| RV-GLSR (s-1) | 1.1 ± 0.2 | 1.3 ± 0.2 | <0.001 |
| RAScd (%) | 26.3 ± 11.7 | 34.6 ± 10.1 | 0.004 |
| RASct (%) | 6.1 ± 4.46 | 7.5 ± 5.4 | 0.27 |
| RASr (%) | 32.4 ± 11.0 | 42.1 ± 9.9 | <0.001 |
| RA-GSR (s-1) | 2.0 ± 0.9 | 2.5 ± 0.6 | 0.01 |
| RA-GSRE (s-1) | 1.9 ± 0.6 | 2.3 ± 0.7 | 0.02 |
| RA-GSRL (s-1) | 2.0 ± 0.6 | 2.5 ± 0.8 | 0.007 |
| PERCENTAGE OF WOMEN WITH IMPAIRED STE PARAMETERS IN COMPARISON TO THE ACCEPTED NORMAL VALUES | |||
| LV-GLS <20% (%) | 20 (62.5) | 4 (13.3) | <0.001 |
| LV-GCS <23.3% (%) | 16 (50.0) | 7 (23.3) | 0.03 |
| LASr <39% (%) | 18 (56.3) | 5 (16.7) | 0.001 |
| RV-GLS <20% (%) | 19 (59.4) | 7 (23.3) | 0.004 |
| RASr <35% (%) | 20 (62.5) | 8 (26.7) | 0.005 |
Table 5.
Univariate and multivariate logistic regression analyses performed for identifying the independent predictors of subclinical myocardial dysfunction in pGDM women, at 4 yrs postpartum. BMI, body mass index; MAP, mean arterial pressure; NLR, neutrophil-to-lymphocyte ratio; pGDM, previous gestational diabetes mellitus.
Table 5.
Univariate and multivariate logistic regression analyses performed for identifying the independent predictors of subclinical myocardial dysfunction in pGDM women, at 4 yrs postpartum. BMI, body mass index; MAP, mean arterial pressure; NLR, neutrophil-to-lymphocyte ratio; pGDM, previous gestational diabetes mellitus.
| UNIVARIATE LOGISTIC REGRESSION ANALYSIS |
MULTIVARIATE LOGISTIC REGRESSION ANALYSIS |
|||||
|---|---|---|---|---|---|---|
| VARIABLES | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
| Third trimester age (yrs) | 1.08 | 0.96-1.21 | 0.21 | |||
| Third trimester BMI (Kg/m2) | 1.87 | 1.24-2.83 | 0.003 | 1.88 | 1.19.2.98 | 0.03 |
| Third trimester glycosylated hemoglobin (mmol/mol) | 2.30 | 1.35-3.94 | 0.002 | 2.34 | 1.08-5.04 | 0.02 |
| Third trimester NLR | 1.89 | 1.08-3.33 | 0.03 | 1.69 | 0.64-4.45 | 0.28 |
| Third trimester MAP | 1.01 | 0.94-1.09 | 0.77 | |||
Table 6.
Univariate and multivariate logistic regression analyses performed for identifying the independent predictors of early carotid atherosclerosis in pGDM women, at 4 yrs postpartum. BMI, body mass index; MAP, mean arterial pressure; NLR, neutrophil-to-lymphocyte ratio; pGDM, previous gestational diabetes mellitus.
Table 6.
Univariate and multivariate logistic regression analyses performed for identifying the independent predictors of early carotid atherosclerosis in pGDM women, at 4 yrs postpartum. BMI, body mass index; MAP, mean arterial pressure; NLR, neutrophil-to-lymphocyte ratio; pGDM, previous gestational diabetes mellitus.
| UNIVARIATE LOGISTIC REGRESSION ANALYSIS |
MULTIVARIATE LOGISTIC REGRESSION ANALYSIS |
|||||
|---|---|---|---|---|---|---|
| VARIABLES | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
| Third trimester age (yrs) | 1.37 | 1.09-1.70 | 0.005 | 1.06 | 0.94-1.19 | 0.32 |
| Third trimester BMI (Kg/m2) | 1.40 | 1.09-1.82 | 0.01 | 1.35 | 1.02-1.79 | 0.03 |
| Third trimester glycosylated hemoglobin (mmol/mol) | 1.37 | 1.08-1.74 | 0.009 | 1.37 | 1.00-1.88 | 0.02 |
| Third trimester NLR | 1.34 | 0.81-2.22 | 0.25 | |||
| Third trimester MAP | 1.06 | 0.95-1.17 | 0.29 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



