
Submitted:
14 November 2024
Posted:
18 November 2024
You are already at the latest version
Abstract
Background:
Cervical cancer lymph node metastasis involves lymphovascular space invasion (LVSI), isolated tumor cells (ITC), and micro- and macro-metastases (MIC and MAC), all potential targets for prevention and treatment.
Purpose:
This study aimed to track cancer spread, identify risk factors for lymph node metastasis, and explore avenues for prevention.
Methods:
We conducted a retrospective analysis on 27 early cervical cancer patients (tumor size ≤ 4 cm) who underwent sentinel (SLN) and non-sentinel (nSLN) lymph node dissection and histopathological ultrastaging. Patient and tumor characteristics associated with lymph node events (LNE) and prevention efforts were analyzed, following STROBE guidelines.
Results:
Primary prevention steps were absent, secondary prevention was limited to opportunistic measures, and follow-up served as tertiary prevention. LNE occurred in 11 of 27 cases: 4 with ITC alone, 1 with MIC alone, 1 with both ITC and MIC, 1 with MAC alone, and 4 with both MIC and MAC. Obturator and external iliac lymph nodes were most commonly affected, and only LVSI was a significant predictor of LNE (p < 0.05). Among LNE cases, 9 patients were at FIGO stage 1b1 and 2 at stage 1b2. The smallest tumor with lymph node burden (ITC in both SLN and nSLN) was 2.0 cm, while MAC alone occurred in a single nSLN case.
Conclusions:
Limited prevention at all levels contributes to lymph node metastasis in about half of early-stage cervical cancer cases. FIGO stages do not adequately predict the extent, type, or distribution of lymph node invasion.
Keywords:
Cervical cancer
; Sentinel lymph node
; Metastases
; Ultrastaging
; Prevention
Introduction
The lymphatic system plays a crucial role in cancer spread, a process that can be traced through various tests [1,2,3]. This makes the lymphatic system critical in cancer management at all stages, such as prevention to local control of the disease [4]. The current standard of care for early cervical cancer (with no suspected lymph nodes on imaging) involves sentinel lymph node (SLN) dissection and histopathologic ultrastaging (serial sections and immunohistochemistry) of SLNs in the final specimen (with an optional intraoperative SLN examination), especially in the setup of fertility-sparing [5]. Lymph node staging is unnecessary in T1a1 stage without lymphovascular space invasion (LVSI), but SLN dissection (SLND) alone is recommended in T1a1 with positive LVSI and in T1a2 cancers, while systematic lymphadenectomy with optional SLND remains the standard for stages T1b1-3, T2a1 and some T2a2 [5,6]. Despite the good prognosis of early cervical cancer and significant improvements in survival rates over the past few decades, 5 to 26% of patients experience different kind of relapse after receiving appropriate primary treatment [7].
Although the risk factors for cervical cancer are well-established, it remains essential to determine risk factors associated with low-volume nodal metastasis, such as micrometastases (MICs) and isolated tumour cells (ITCs) [5,8,9]. There is an urgent need to determine whether the progression of cancer can be effectively halted. Several studies have examined various risk factors for developing and treatment of cervical cancer, highlighting the need for a targeted approach to prophylaxis that addresses these risks at the histopathological level [10,11].
In a previous study [12] involving 54 patients with FIGO IA2-IB1 cervical cancer (FIGO 2009-2018 classification system), we identified only one patient with a real false-negative result in non-SLN assessed through ultrastaging. This study was one of those that in analysing all lymph nodes subjected to histopathological ultrastaging, both SLNs and non-SLNs (nSLNs), regardless of one- or two-sided SLN colouring [13]. The case in question did not adhere to the expected stepwise progression through the lymphatic system, where all stages of lymphatic involvement—lymphovascular space invasion (LVSI), ITC, MIC, and macrometastasis (MAC)—should be present in a single case as a pathological continuum in lymph node involvement. This led us to reexamine the distribution of lymph node events at the individual patient level, along with evaluating preventive measures at primary, secondary, and tertiary levels for each patient.
Methods
We followed the STROBE Reporting Guidelines [14]. The inclusion criteria were patients >18 years-old undergoing Piver-Rutledge class III radical hysterectomy for CC FIGO stage IA2-IB1 (FIGO 2009-2018 staging system) who had SLND procedure along with subsequent lymphadenectomy and pathological ultrastaging performed between 1st January 2010 and 30th April 2014. Exclusion criteria included lack of SLND concept (regional lymphadenectomy without SLND). This subset of 27 patients with SLND from the original cohort of 54 patients in our prior study was selected for detailed re-evaluation in this ancillary analysis. All excised lymph nodes, including SLNs and non-SLNs (nSLNs), were subjected to histopathologic ultrastaging. Our ultrastaging method involved systematic sectioning of lymph nodes every 150 micrometres into 4-micrometre-thick slices. The specifics of our histopathologic processing are detailed in two prior publications [12,15].
We reviewed all 27 cases for the following parameters: patient age; primary, secondary, and tertiary prevention measures; initial cancer symptoms; histopathologic cancer subtype; FIGO stage (FIGO 2018 staging system) [16]; tumour size according to histopathological evaluation; depth of cancer invasion; presence of lymphovascular space invasion (LVSI) in cancer tissue as well as in paracervical/parametrium tissue; type and location of lymph node events within the pelvis (or/and paraaortic area); and lymph node burden. Nodal disease burden measured by the dimension of the largest lymph node event in each individual lymph node with the event. If they were ITCs, the value <0.2 mm per case was recorded. Study organisation is presented in Figure 1. This comprehensive approach enabled us to precisely track the metastatic progression in our patients and pinpoint critical intervention that could alter the disease’s course in a preventive manner. We expanded our analysis to determine the risk factors through these 27 patients, with similar treatment eligibility criteria. We did not re-assess of the status of lymph nodes since ultrastaging was already performed.
We analysed the type of prevention present in our group of patients. The aim of primary prevention is to prevent the disease from occurring in the first place - the worldwide known, most effective strategy in this category is vaccination against human papillomavirus (HPV), the virus virtually responsible for the most of cervical cancer cases. The HPV vaccine is designed to protect against the most common and high-risk types, significantly reducing the likelihood of developing cervical cancer. The primary prevention is also controlling other risk factors, like tobacco smoking.
Secondary prevention focuses on the early detection and treatment of precancerous conditions before they progress to cancer. Regular screening through Pap smears and HPV testing is critical in this regard. These screening methods can identify abnormal cervical cells early, allowing for timely interventions that can prevent the development of cervical cancer. It is essential for women to engage in routine screening and follow-up care.
Tertiary prevention is concerned with follow-up and rehabilitation procedures to reduce the impact of the disease on the patient’s life after main treatment. Follow-up options in cervical cancer may include regular gynaecological examinations, Pap smears, transvaginal ultrasound, and other imaging tests depending on the stage of cancer and symptoms occurring after treatment. Furthermore, providing psychological, social, and rehabilitative support is vital for enhancing the quality of life for survivors. Tertiary prevention aims not only to extend life but also to ensure that survivors can lead fulfilling lives after treatment.
This study received approval from the institutional review board (NKBBN/558/2014-2015).
Results
General Results
The characteristics of the study population are presented in Table 1. The average age of patients was 49.6 years. Of 27 individuals with FIGO 1a2 to 1b2 stage (FIGO classification system of cervical cancer 2018-), 7 patients (26%) had MIC alone or MIC and MAC, or MAC alone, and 4 (15%) ITC (Figure 1, Table 2). These 11 patients with LNE did not differ significantly in terms of all but one (LVSI) analysed pathology-related tumour factors from those who did not have LNE (Table 3).
None of the cases underwent primary prevention. Pap smear was used as a secondary prevention and as a tertiary prevention was follow-up. There is no data what were the first symptoms in most cases, but if they were, it was abnormal uterine bleeding (AUB). Most of patients had squamous cell carcinoma in FIGO (2018-) stage Ib2 (n = 14, 52%) with the average depth of invasion 10 mm (4 – 20 mm). In most cases there was no LVSI and the most common nodal pathology was macrometastasis (MAC).
Prevention
For primary prevention of cervical cancer, none of the 27 patients had received the vaccine against HR HPV. None of this whole group had received sex education at school.
In terms of secondary prevention, most patients came to the gynaecologist privately for a gynaecological check-up or as an opportunistic cervical cancer screening with conventional cytology on irregular basis (no population-based screening). Tertiary prevention consisted of follow-up, with attempts being made to transfer patients without lymph node events to care outside the centre (Table 2).
Lymphatic Tracts
Table 3 presents the relationship between tumour-related factors and potential lymph nodes involvement. All cancer lesions in the lymph nodes were considered together. Only LVSI (either intra- or/and extratumoural) showed a statistically significant relationship with events in lymph nodes (regardless of whether SLN or nSLN).
In Table 4, we presented the distribution of lymph node events in early cervical cancer. The type and size of LNE did not correlate with the FIGO stage. It should be noted that the subgroup without LNE (16/27) had similar FIGO stages (Figure 1). The most common pathology in the lymph nodes was MAC (6/11 cases) and it was the most common lesion type in external iliac and obturator lymph nodes. The same is true of ITC. However, MIC and ITC (but not MAC) were also remarkable events in the lymph nodes of the remaining anatomic locations (common iliac, parametrial). The possible levels and points of prophylactic interventions are depicted in Figure 2.
Discussion
Our study based on the analysis of 27 patients with FIGO stage 1a2 to 1b2 cervical cancer has shown that MIC and/or MAC were present in 7 of the patients, while 4 patients presented ITC.
The novelty of the current study is that the ultrastaging approach allows to trace the progression of metastases through the lymphatic route, and the reanalysis of cases allows for the analysis of the epidemiology of patients and for the further proposals of procedures that could change the course of the disease. Based on the above, we selected this group for in-depth analysis through the prism of prevention.
In a previous study of 52 patients, in which a cohort of 27 patients with ultrastaging was matched with 27 control patients without ultrastaging, LVSI was the only factor that differentiated both groups [12]. Our previous study showed that ultrastaging of all nodes did not change the Tumour-Node-Metastasis (TNM) system status nor have an impact on prognosis. We hypothesized that LVSI is a strong predictor of lymph node metastases, which may be independent of positive SLNs as was suggested by the results of SENTICOL I and II, and MICROCOL studies [17,18]. Our protocol corresponded with that of SENTICOL except on the use of lymphoscintigraphy [19]. However, although extensive study on LNE with ultrastaging in our study, we were unable to demonstrate the presence of LVSI, ITC, MIC and MAC in the lymph nodes (SLN or nSLN) even in one patient. This notion is in line with the fact that nodal spread is an uncommon phenomenon, which occurs via a more disseminated pathway, not only from an anatomical point of view (upper and lower pathway), but also from a typological one (MIC and MAC issues but not ITC) [20,21,22]. However, it must be clearly stated that the importance of ITC is not yet fully established and should not be completely dismissed in the treatment decision-making process [23].
Prevention of cervical cancer can be achieved through vaccination against HR HPV subtypes, sexuality education, quitting smoking tobacco, slow food (primary prevention), routine cervical screening and HR HPV testing for early detection and treatment (secondary prevention), and administering post-treatment controls timely and effectively (tertiary prevention) [4,23].
Anti-HR HPV vaccine was first introduced in Poland in November 2006. According to the international guidelines, introduced into Polish National Health Fund – financed system from 1 September 2024, children from 9 years of age up to 14 years of age for both, girls and boys, are eligible for anti HR-HPV vaccinations. Sexuality education, despite its long history in Poland, is far from the quality and universality recommended by World Health Organisation [24,25]. The law banning smoking in public spaces and in restaurant rooms was introduced in Poland in November 2010. It should be noted, however, that the availability of some preventive options permeates society slowly, and the latency period of cervical cancer in the average-risk population (i.e., non-HIV carriers, no immunocompromised patients) lasts even dozen years - this together means that cervical cancer in our group of patients was often detected at the moment of symptom onset (this is a real picture of the effectiveness of primary prevention in Poland at that time).
In nearly half of patients Pap smear was rather a confirmatory approach of symptoms than a form of organised screening. The screening was an opportunistic one although there was a systematic screening available in Poland in those times (started in 2006, for 25-59 aged women). The benefits of secondary prevention in terms of liquid-based cervical cytology (or conventional cytology as a secondary option) and HR-HPV testing with colposcopy as a diagnostic and treatment tools are well known.
The risk of cervical cancer lymph node recurrence is clearly associated with routinely recorded markers for adverse prognosis. Guidelines published by the European Society of Gynaecological Oncology (ESGO), European Society for Medical Oncology (ESMO), and National Comprehensive Cancer Network (NCCN) do not contain any individualisation of the surveillance, indicating a lack of agreement on the best post-treatment follow-up regarding lymph nodes events [26]. The annual recurrence risk model (ARRM) calculator (https://esgo.org/calculators/) has shown promise for tailored tertiary prevention of cervical cancer but not yet for lymph nodes [23]. As part of the tertiary prophylaxis, patients with cervical cancer who have undergone conization can be vaccinated against HPV [27].
In addition to preventive measures at different levels, it is worth mentioning the emerging possibilities of nanodiagnosis, which can mix prevention and treatment. Nanodiagnosis offers promising potential in the detection of metastatic lesions, with several approaches currently undergoing clinical trials. Besides improving tumour imaging contrast, nanoparticles have been utilized for locoregional imaging, early detection of metastases, and the identification of disseminated and circulating tumour cells, which are critical for therapeutic interventions [28].
A number of studies can be put forward to underlie the paradigm of qualitatively graded (LVSI, ITC, MIC, MAC) and quantitatively graded (SLN in different anatomical locations) spread of cervical cancer [9,20,29,30,31,32,33,34]. Since the risk of LNE (to the level of ultra-staging of nodes) does not reflect the FIGO stage in early cervical cancer, the best solution to avoid LNE, lymphatic morbidity and further dilemmas for the patients and healthcare systems is to prevent the disease at all [35,36,37]. Therefore, substantial efforts should be focused on prevention at all levels.
Strengths and Limitations of the Study
The main strength of this study is its demonstration that the lack of cervical cancer prevention leads to lymph node involvement, which can be documented through histopathological ultrastaging. This effect of insufficient prevention is independent of the FIGO stage. Another strength is that our study was an attempt to find out to what extent the presence of effective prevention could lead to decreased morbidity associated with LNE, suggesting that effective screening and adaptive follow-up strategies could be of value. We also sensitised how striking is the contrast between the real-world-based situation of prevention and the expenditure not only on the assessment of lymph nodes in ultrastaging, but also on the subsequent highly specialised treatment.
The main limitation is its design as a monocentric and retrospective single-cohort study. A decade ago, primary documentation, such as patient anamnesis, was often completed by residents and compared by the operator, but without supplementation, as the documentation was sometimes still paper-based at that time. Consequently, we were unable to answer why, among cases with similar characteristics, one group had LNE while the other did not. It’s just known in advance that this question cannot be answered.
The second limitation, resulting from the schedule of study, is the lack of a control arm. In response it must be said that more than 10 years after the first patient, there is currently no vaccinated group with cancers of the same size in which we could check the extent of (micro)metastatic disease. Hypothetically, we can only assume that in a matched, vaccinated group of women, cervical cancer prompting full lymphadenectomy will not occur at all. This does not rule out the possibility of very low-volume nodal disease, such as the presence of ITCs in the lymph nodes.
The third limitation is that we did not undertake OS/DFS re-evaluation in our study.
Recommendation for Prevention
In conclusion, the prevention approaches are hopefully the answer for the current dilemma of whether sentinel lymph node dissection is sufficient for staging and treatment purposes in early cervical cancer. All stages of prevention can finally replace treatment of cervical cancer patients, thus decreasing patients’ morbidity and mortality, and saving money for health systems as well.
Author Contributions
Marcin Śniadecki: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. Martyna Danielkiewicz: Conceptualization, Formal Analysis, Data curation, Writing – original draft, Writing – review & editing. Olga Piątek-Dalewska: Data curation, Formal Analysis, Resurces, Writing – review & editing. Paulina Jaworek: Resources, Software, Writing – review & editing. Vincent Balaya: Validation, Writing – review & editing. Zuzanna Kilińska: Resources, Writing – review & editing. Zuzanna Sijka: Data curation, Writing – review & editing. Anna Wściślak: Data curation, Writing – review & editing. Anna Gołąbiewska: Resources, Writing – review & editing. Marcin Liro: Writing – review & editing. Szymon Wojtylak: Writing – review & editing. Dariusz Wydra: Supervision, Writing – review & editing. All authors have read and agreed to the published version of the manuscript.
Funding
Not applicable.
Ethics Approval and Consent to Participate
The study was approved by institutional ethics committee. All patients consented to participate in this study in a written form.
Consent for Publication
Not applicable (included in the patient consent to participate).
Availability of Data and Materials
Raw data are contained in a database compiled from hospital records.
Acknowledgments
Authors thank Ms. Zuzanna Boyke for her assistance in preparation of Figure 2.
Competing Interests
The authors declare that they have no competing interests.
List of Abbreviations
| AJCC | American Joint Committee on Cancer |
| ARRM | Annual Recurrence Risk Model |
| AUB | Abnormal uterine bleeding |
| ESGO | European Society of Gynaecological Oncology |
| ESMO | European Society of Medical Oncology |
| ITCs | Isolated tumor cells |
| LND | Lymphadenectomy |
| LNE | Lymph node events |
| LVSI | Lymphovascular space invasion |
| MAC | Macrometastasis |
| MIC | Micrometastasis |
| NCCN | National Comprehensive Cancer Network |
| SLN | Sentinel lymph node |
| SLND | Sentinel lymph node dissection |
| STROBE | STrengthening the Reporting of OBservational studies in Epidemiology |
| TNM | Tumor-Node-Metastasis (system) |
| nSLN | Non-sentinel lymph node |
References
- Van Trappen, P.O.; Pepper, M.S. Lymphatic dissemination of tumour cells and the formation of micrometastases. Lancet Oncol. 2002, 3, 44–52. [Google Scholar] [CrossRef]
- Abati, A.; Liotta, L.A. Looking forward in diagnostic pathology: the molecular superhighway. Cancer 1996, 78, 1–3. [Google Scholar] [CrossRef]
- Benedetti-Panici, P.; Maneschi, F.; D’Andrea, G.; Cutillo, G.; Rabitti, C.; Congiu, M.; Coronetta, F.; Capelli, A. Early cervical carcinoma: the natural history of lymph node involvement redefined on the basis of thorough parametrectomy and giant section study. Cancer 2000, 88, 2267–2274. [Google Scholar] [CrossRef]
- Śniadecki, M.; Poniewierza, P.; Jaworek, P.; Szymańczyk, A.; Andersson, G.; Stasiak, M.; Brzeziński, M.; Bońkowska, M.; Krajewska, M.; Konarzewska, J.; Klasa-Mazurkiewicz, D.; Guzik, P.; Wydra, D.G. Thousands of Women’s Lives Depend on the Improvement of Poland’s Cervical Cancer Screening and Prevention Education as Well as Better Networking Strategies Amongst Cervical Cancer Facilities. Diagnostics (Basel) 2022, 12(8), 1807. [Google Scholar] [CrossRef] [PubMed]
- Morice, P.; Scambia, G.; Abu-Rustum, N.R.; Acien, M.; Arena, A.; Brucker, S.; Cheong, Y.; Collinet, P.; Fanfani, F.; Filippi, F.; Eriksson, A.G.Z.; Gouy, S.; Harter, P.; Matias-Guiu, X.; Pados, G.; Pakiz, M.; Querleu, D.; Rodolakis, A.; Rousset-Jablonski, C.; Stepanyan, A.; Testa, A.C.; Macklon, K.T.; Tsolakidis, D.; De Vos, M.; Planchamp, F.; Grynberg, M. Fertility-sparing treatment and follow-up in patients with cervical cancer, ovarian cancer, and borderline ovarian tumours: guidelines from ESGO, ESHRE, and ESGE. The Lancet Oncology 2024, 25(11), e602–e610. [Google Scholar] [CrossRef] [PubMed]
- Koh, W. J.; Abu-Rustum, N. R.; Bean, S.; Bradley, K.; Campos, S. M.; Cho, K. R.; Chon, H. S.; Chu, C.; Clark, R.; Cohn, D.; Crispens, M. A.; Damast, S.; Dorigo, O.; Eifel, P. J.; Fisher, C. M.; Frederick, P.; Gaffney, D. K.; Han, E.; Huh, W. K.; Lurain, J. R.; Mariani, A.; Mutch, D.; Nagel, C.; Nekhlyudov, L.; Fader, A.N.; Remmenga, S.W.; Reynolds, R.K.; Tillmanns, T.; Ueda, S.; Wyse, E.; Yashar, C.M.; McMillian, N.R.; Scavone, J. L. Cervical Cancer, Version 3.2019, NCCN Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw. 2019, 17(1), 64–84. [Google Scholar] [CrossRef]
- Cibula, D.; Dostálek, L.; Jarkovsky, J.; Mom, C. H.; Lopez, A.; Falconer, H.; Scambia, G.; Ayhan, A.; Kim, S. H.; Isla Ortiz, D.; Klat, J.; Obermair, A.; Di Martino, G.; Pareja, R.; Manchanda, R.; Kosťun, J.; Dos Reis, R.; Meydanli, M. M.; Odetto, D.; Laky, R.; Zapardiel, I.; Weinberger, V.; Benešová, K.; Borčinová, M.; Cardenas, F.; Wallin, E.; Pedone Anchora, L.; Akilli, H.; Abu-Rustum, N.R.; Barquet-Muñoz, S.A.; Javůrková, V.; Fischerová, D.; van Lonkhuijzen, L. R. C. W. Post-recurrence survival in patients with cervical cancer. Gynecol Oncol. 2022, 164(2), 362–369. [Google Scholar] [CrossRef] [PubMed]
- Olawaiye, A.B.; Baker, T.P.; Washington, M.K.; Mutch, D.G. The new (Version 9) American Joint Committee on Cancer tumor, node, metastasis staging for cervical cancer. CA Cancer J Clin. 2021, 71(4), 287–298. [Google Scholar] [CrossRef]
- Dostálek, L.; Benešová, K.; Klát, J.; Kim, S. H.; Falconer, H.; Kostun, J.; Dos Reis, R.; Zapardiel, I.; Landoni, F.; Ortiz, D. I.; van Lonkhuijzen, L. R. C. W.; Lopez, A.; Odetto, D.; Borčinová, M.; Jarkovsky, J.; Salehi, S.; Němejcová, K.; Bajsová, S.; Park, K. J.; Javůrková, V.; Abu-Rustum, N.R.; Dundr, P.; Cibula, D. Stratification of lymph node metastases as macrometastases, micrometastases, or isolated tumor cells has no clinical implication in patients with cervical cancer: Subgroup analysis of the SCCAN project. Gynecol Oncol. 2023, 168, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Derbie, A.; Amare, B.; Misgan, E.; Nibret, E.; Maier, M.; Woldeamanuel, Y.; Abebe, T. Histopathological profile of cervical punch biopsies and risk factors associated with high-grade cervical precancerous lesions and cancer in northwest Ethiopia. PLoS One 2022, 17(9), e0274466. [Google Scholar] [CrossRef]
- Shinohara, S.; Ochi, T.; Miyazaki, T.; Fujii, T.; Kawamura, M.; Mochizuki, T.; Ito, M. Histopathological prognostic factors in patients with cervical cancer treated with radical hysterectomy and postoperative radiotherapy. Int J Clin Oncol. 2004, 9(6), 503–509. [Google Scholar] [CrossRef] [PubMed]
- Sniadecki, M.; Wydra, D.G.; Wojtylak, S.; Wycinka, E.; Liro, M.; Sniadecka, N.; Mrozińska, A.; Sawicki, S. The impact of low volume lymph node metastases and stage migration after pathologic ultrastaging of non-sentinel lymph nodes in early-stage cervical cancer: a study of 54 patients with 4.2 years of follow up. Ginekol Pol. 2019, 90, 20–30. [Google Scholar] [CrossRef] [PubMed]
- Barranger, E.; Cortez, A.; Commo, F.; Marpeau, O.; Uzan, S.; Darai, E.; Callard, P. Histopathological validation of the sentinel node concept in cervical cancer. Ann Oncol. 2004, 15(6), 870–874. [Google Scholar] [CrossRef] [PubMed]
- von Elm, E.; Altman, D. G.; Egger, M.; Pocock, S. J.; Gøtzsche, P. C.; Vandenbroucke, J. P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007, 335(7624), 806–808, [Published simultaneously in eight journals; https://www.equator-network.org/reporting-guidelines/strobe/]. [Google Scholar] [CrossRef]
- Sniadecki, M.; Sawicki, S.; Wojtylak, S.; Liro, M.; Wydra, D. Clinical feasibility and diagnostic accuracy of detecting micrometastatic lymph node disease in sentinel and non-sentinel lymph nodes in cervical cancer: outcomes and implications. Ginekol Pol. 2014, 85(1), 10–13. [Google Scholar] [CrossRef] [PubMed]
- Bhatla, N.; Berek, J.S.; Cuello Fredes, M.; Denny, L.A.; Grenman, S.; Karunaratne, K.; Kehoe, S. T.; Konishi, I.; Olawaiye, A. B.; Prat, J.; Sankaranarayanan, R.; Brierley, J.; Mutch, D.; Querleu, D.; Cibula, D.; Quinn, M.; Botha, H.; Sigurd, L.; Rice, L.; Ryu, H. S.; Ngan, H.; Mäenpää, J.; Andrijono, A.; Purwoto, G.; Maheshwari, A.; Bafna, U.D.; Plante, M.; Natarajan, J. Revised FIGO staging for carcinoma of the cervix uteri. Int J Gynaecol Obstet. 2019, 145(1), 129–135, [published correction appears in Int J Gynaecol Obstet. 2019, 147(2), 279–280]. [Google Scholar] [CrossRef]
- Pache, B.; Tantari, M.; Guani, B.; Mathevet, P.; Magaud, L.; Lecuru, F.; Balaya, V.; SENTICOL Group. Predictors of Non-Sentinel Lymph Node Metastasis in Patients with Positive Sentinel Lymph Node in Early-Stage Cervical Cancer: A SENTICOL GROUP Study. Cancers (Basel) 2023, 15(19), 4737. [Google Scholar] [CrossRef]
- Tantari, M.; Bogliolo, S.; Morotti, M.; Balaya, V.; Bouttitie, F.; Buenerd, A. Lymph Node Involvement in Early-Stage Cervical Cancer: Is Lymphangiogenesis a Risk Factor? Results from the MICROCOL Study. Cancers (Basel) 2022, 14(1), 212. [Google Scholar] [CrossRef] [PubMed]
- Lécuru, F.; Mathevet, P.; Querleu, D.; Leblanc, E.; Morice, P.; Daraï, E.; Marret, H.; Magaud, L.; Gillaizeau, F.; Chatellier, G.; Dargent, D. Bilateral negative sentinel nodes accurately predict absence of lymph node metastasis in early cervical cancer: results of the SENTICOL study. J Clin Oncol. 2011, 29(13), 1686–1691. [Google Scholar] [CrossRef]
- Lührs, O.; Bollino, M.; Ekdahl, L.; Lönnerfors, C.; Geppert, B.; Persson, J. Similar distribution of pelvic sentinel lymph nodes and nodal metastases in cervical and endometrial cancer. A prospective study based on lymphatic anatomy. Gynecol Oncol. 2022, 165(3), 466–471. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; He, X.; Wang, H.; Dong, W.; Zhang, Y.; Zhao, J.; Willborn, K. C.; Huang, B.; Wang, Z.; Jiang, P. Topographic distribution of lymph node metastasis in patients with stage IB1 cervical cancer: an analysis of 8314 lymph nodes. Radiat Oncol. 2021, 16(1), 54. [Google Scholar] [CrossRef] [PubMed]
- Mathevet, P.; Guani, B.; Ciobanu, A.; Lamarche, E. M.; Boutitie, F.; Balaya, V.; Lecuru, F. Histopathologic Validation of the Sentinel Node Technique for Early-Stage Cervical Cancer Patients. Ann Surg Oncol. 2021, 28(7), 3629–3635. [Google Scholar] [CrossRef]
- Śniadecki, M.; Guani, B.; Jaworek, P.; Klasa-Mazurkiewicz, D.; Mahiou, K.; Mosakowska, K.; Buda, A.; Poniewierza, P.; Piątek, O.; Crestani, A.; Stasiak, M.; Balaya, V.; Musielak, O.; Piłat, L.; Maliszewska, K.; Aristei, C.; Guzik, P.; Wojtylak, S.; Liro, M.; Gaillard, T.; Kocian, R.; Gołąbiewska, A.; Chmielewska, Z.; Wydra, D. Tertiary prevention strategies for micrometastatic lymph node cervical cancer: A systematic review and a prototype of an adapted model of care. Crit Rev Oncol Hematol. 2024, 197, 104329. [Google Scholar] [CrossRef] [PubMed]
- Jóźwiak, W. Krótka historia edukacji seksualnej w Polsce. Available online: https://edukacjaseksualna.com/standardy-edukacji-seksualnej-na-swiecie-i-w-polsce/ (accessed on 9 September 2024).
- World Health Organisation. Comprehensive sexuality education. 2023. Available online: https://www.who.int/news-room/questions-and-answers/item/comprehensive-sexuality-education (accessed on 9 September 2024).
- Cibula, D.; Dostálek, L.; Jarkovsky, J.; Mom, C.H.; Lopez, A.; Falconer, H.; Fagotti, A.; Ayhan, A.; Kim, S. H.; Isla Ortiz, D.; Klat, J.; Obermair, A.; Landoni, F.; Rodriguez, J.; Manchanda, R.; Kosťun, J.; Dos Reis, R.; Meydanli, M. M.; Odetto, D.; Laky, R.; Zapardiel, I.; Weinberger, V.; Benešová, K.; Borčinová, M.; Pari, D.; Salehi, S.; Bizzarri, N.; Akilli, H.; Abu-Rustum, N.R.; Salcedo-Hernández, R.A.; Javůrková, V.; Sláma, J.; van Lonkhuijzen, L. R. C. W. The annual recurrence risk model for tailored surveillance strategy in patients with cervical cancer. Eur J Cancer. 2021, 158, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Kechagias, K. S.; Kalliala, I.; Bowden, S. J.; Athanasiou, A.; Paraskevaidi, M.; Paraskevaidis, E.; Dillner, J.; Nieminen, P.; Strander, B.; Sasieni, P.; Veroniki, A. A.; Kyrgiou, M. Role of human papillomavirus (HPV) vaccination on HPV infection and recurrence of HPV related disease after local surgical treatment: systematic review and meta-analysis. BMJ. 2022, 378, e070135. [Google Scholar] [CrossRef]
- Hegde, M.; Naliyadhara, N.; Unnikrishnan, J.; Alqahtani, M.S.; Abbas, M.; Girisa, S.; Sethi, G.; Kunnumakkara, A.B. Nanoparticles in the diagnosis and treatment of cancer metastases: Current and future perspectives. Cancer Lett. 2023, 556, 216066. [Google Scholar] [CrossRef] [PubMed]
- Creasman, W.T.; Kohler, M.F. Is lymph vascular space involvement an independent prognostic factor in early cervical cancer? Gynecol Oncol. 2004, 92(2), 525–529. [Google Scholar] [CrossRef]
- Slama, J.; Dundr, P.; Dusek, L.; Cibula, D. High false negative rate of frozen section examination of sentinel lymph nodes in patients with cervical cancer. Gynecol Oncol. 2013, 129(2), 384–388. [Google Scholar] [CrossRef] [PubMed]
- Cibula, D.; Abu-Rustum, N.R.; Dusek, L.; Zikán, M.; Zaal, A.; Sevcik, L. Prognostic significance of low volume sentinel lymph node disease in early-stage cervical cancer. Gynecol Oncol. 2004, 94(1), 175–180. [Google Scholar] [CrossRef] [PubMed]
- Cibula, D.; Abu-Rustum, N. R.; Dusek, L.; Slama, J.; Zikán, M.; Zaal, A.; Sevcik, L.; Kenter, G.; Querleu, D.; Jach, R.; Bats, A. S.; Dyduch, G.; Graf, P.; Klat, J.; Meijer, C. J.; Mery, E.; Verheijen, R.; Zweemer, R. P. Bilateral ultrastaging of sentinel lymph node in cervical cancer: Lowering the false-negative rate and improving the detection of micrometastasis. Gynecol Oncol. 2012, 127(3), 462–466. [Google Scholar] [CrossRef]
- Bats, A.S.; Frati, A.; Mathevet, P.; Orliaguet, I.; Querleu, D.; Zerdoud, S. Contribution of lymphoscintigraphy to intraoperative sentinel lymph node detection in early cervical cancer: Analysis of the prospective multicentre SENTICOL cohort. Gynecol Oncol. 2015, 137(2), 264–269. [Google Scholar] [CrossRef]
- Ouldamer, L.; Marret, H.; Acker, O.; Barillot, I.; Body, G. Unusual localizations of sentinel lymph nodes in early stage cervical cancer: a review. Surg Oncol. 2012, 21(3), e153–157. [Google Scholar] [CrossRef]
- Mathevet, P.; Lécuru, F.; Uzan, C.; Boutitie, F.; Magaud, L.; Guyon, F.; Querleu, D.; Fourchotte, V.; Baron, M.; Bats, A. S.; Senticol 2 group. Sentinel lymph node biopsy and morbidity outcomes in early cervical cancer: Results of a multicentre randomised trial (SENTICOL-2). Eur J Cancer. 2021, 148, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Cibula, D.; Dostalek, L.; Hillemanns, P.; Scambia, G.; Jarkovsky, J.; Persson, J.; Raspagliesi, F.; Novak, Z.; Jaeger, A.; Capilna, M. E.; Weinberger, V.; Klat, J.; Schmidt, R. L.; Lopez, A.; Scibilia, G.; Pareja, R.; Kucukmetin, A.; Kreitner, L.; El-Balat, A.; Pereira, G. J. R.; Laufhütte, S.; Isla-Ortiz, D.; Toptas, T.; Gil-Ibanez, B.; Vergote, I.; Runnenbaum, I. Completion of radical hysterectomy does not improve survival of patients with cervical cancer and intraoperatively detected lymph node involvement: ABRAX international retrospective cohort study. Eur J Cancer. 2021, 143, 88–100. [Google Scholar] [CrossRef] [PubMed]
- Plante, M.; Kwon, J. S.; Ferguson, S.; Samouëlian, V.; Ferron, G.; Maulard, A.; de Kroon, C.; Van Driel, W.; Tidy, J.; Williamson, K.; Mahner, S.; Kommoss, S.; Goffin, F.; Tamussino, K.; Eyjólfsdóttir, B.; Kim, J. W.; Gleeson, N.; Brotto, L.; Tu, D.; Shepherd, L.E.; CX.5 SHAPE Investigators. Simple versus Radical Hysterectomy in Women with Low-Risk Cervical Cancer. N Engl J Med. 2024, 390(9), 819–829. [Google Scholar] [CrossRef]
Figure 1.
Study flow.
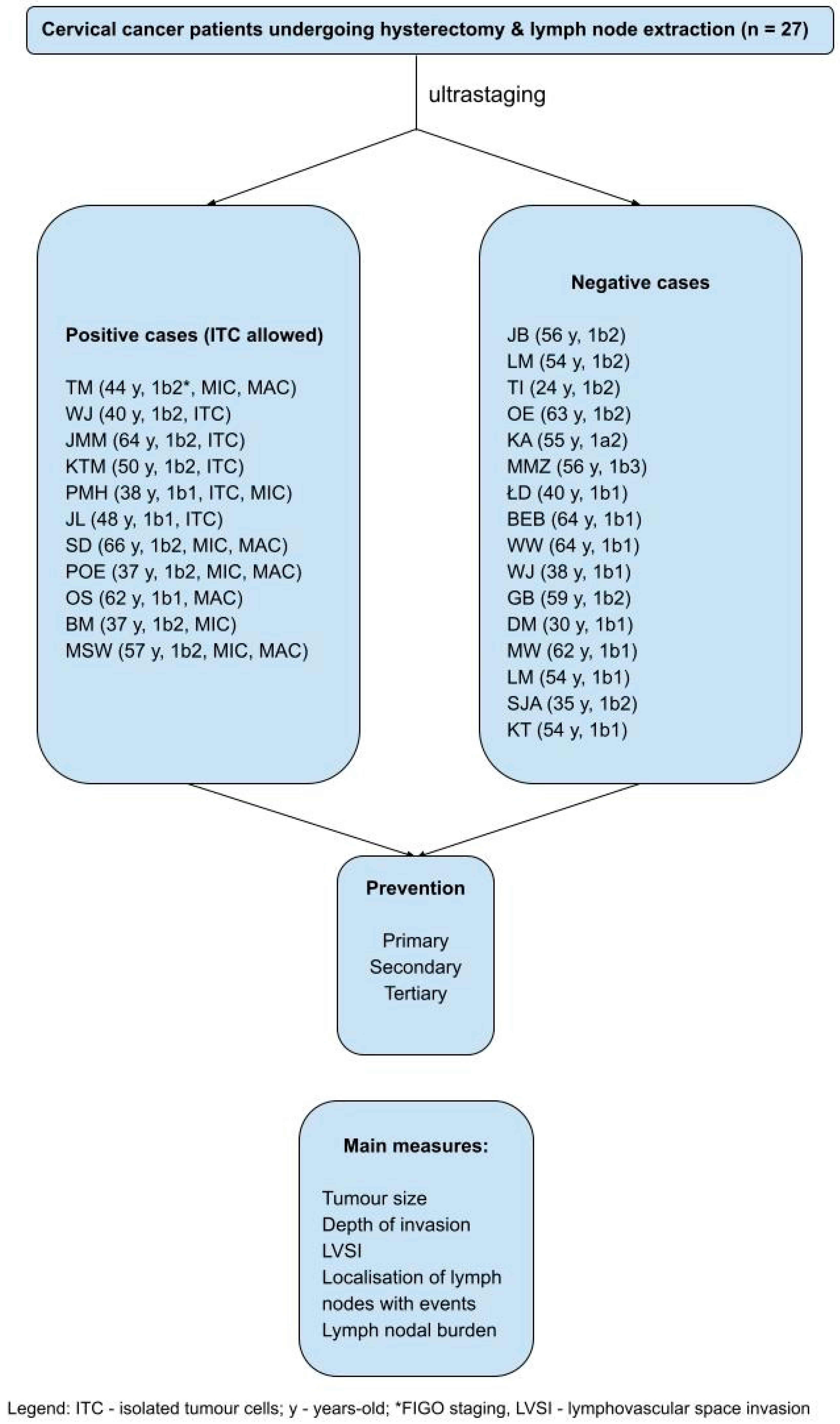
Figure 2.
Location of cervical cancer prevention types in the lymphatic system.
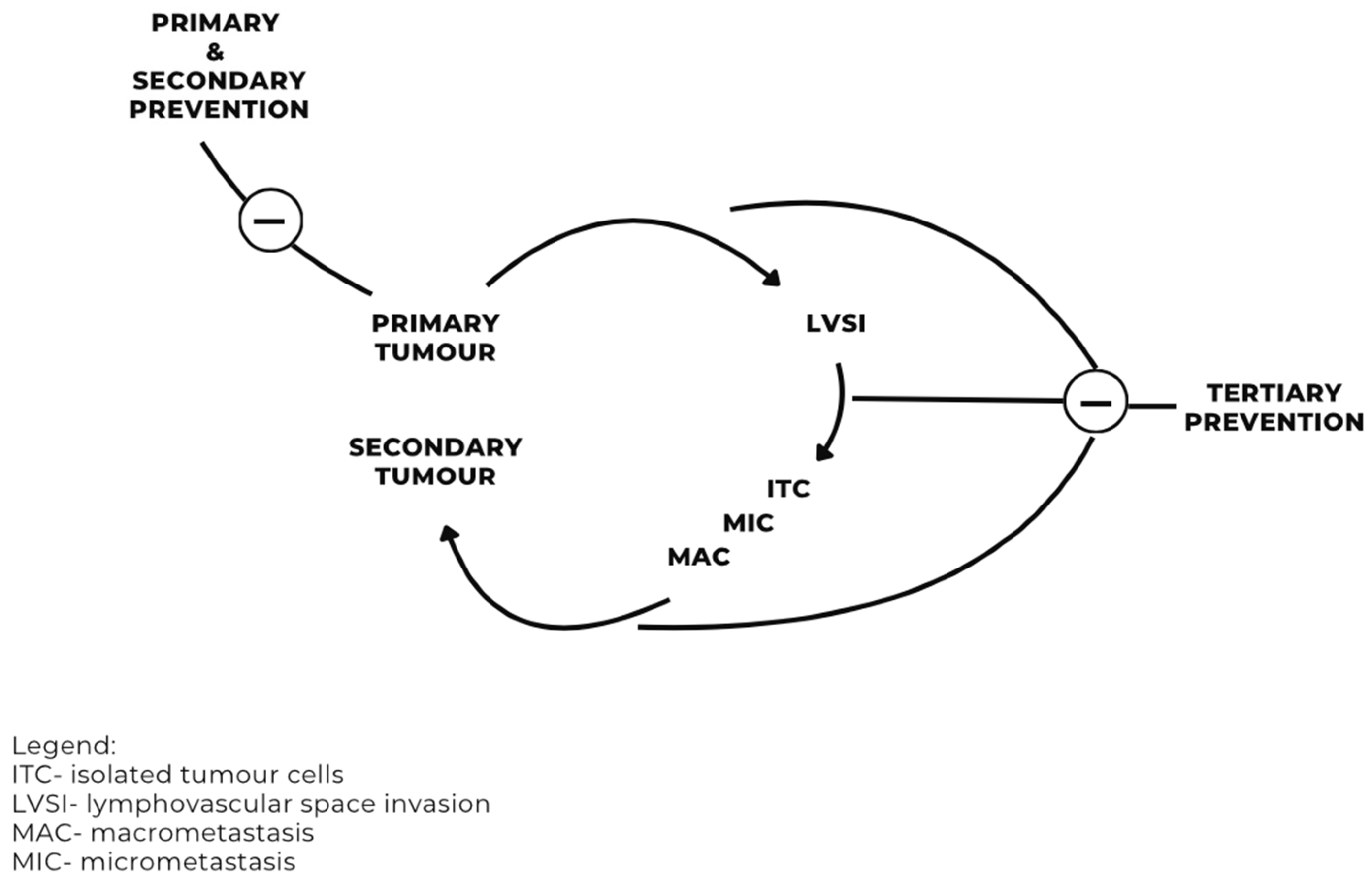

Table 1.
Characteristics of the study population (n=27 patients).
| Characteristic | Result |
|---|---|
| Age of a patient (average years) | 49.6 (24 - 66) |
| Primary prevention | No |
| Secondary prevention | Pap smear |
| Tertiary prevention | Follow up |
|
First symptoms attributed to cervical cancer (number of cases per cent) AUB Discharge Mixed No symptoms at all No data |
9 (33.5) 3 (11.0) 3 (11.0) 2 (7.5) 10 (37.0) |
| Time from the first symptoms to admission (average in months) | 1 - 6 (3.8) |
| Tumor size at histopathologic examination (average in millimetres) | 22.4 (6.0 - 55.0) |
|
FIGO stage (2018-) (number of cases) Ib1 Ib2 Ib3 |
11 14 1 |
| Depth of cancer invasion (average in millimetres) | 10.0 (4.0 - 20.0) |
|
Cancer type (number of cases) squamous cell carcinoma adenocarcinoma |
25 2 |
|
Tumor grade (number of cases) 1 2 3 |
2 14 11 |
|
LVSI (number of cases) intratumoral extratumoral intratumoral and extratumoral no |
10 2 2 13 |
|
ITC (number of cases) Per node*^ Per patient# |
12 4 |
|
MIC (number of cases) Per node*^ Per patient# |
24 2 |
|
MAC (number of cases) Per node*^ Per patient# |
30 5 |
Legend: FIGO - International Federation of Gynecology and Obstetrics, ITC - isolated tumor cells, MIC - micrometastasis, MAC - macrometastasis; *irrespective of SLN or nSLN; ^refers to one (dominant) lymph node event per lymph node;.
Table 2.
Detailed analysis of prevention in the study population (n=27 patients).
| Level of prevention | Main representative | Description | Result |
|---|---|---|---|
| Primary | Controlling risk factors | Education on cervical cancer risk factors and HR-HPV vaccines | 0 |
| Secondary | Cytology (Pap smear) | Pap 1 Pap 2 Pap 3 (ASCUS) Pap 4 (HSIL) Pap 5 (CA) No data |
1 3 2 4 2 15 |
| Tertiary | Follow up |
Subgroup with LNE (n1=11) On site Outside the centre Mixed Unknown* Subgroup without LNE (n2=16) On site Outside the centre Mixed Unknown* |
4 5 1 1 4 8 3 1 |
Table 3.
Differences between metastatic and ITC-positive vs. nodal event-free patients (total 27 patients).
Table 3.
Differences between metastatic and ITC-positive vs. nodal event-free patients (total 27 patients).
| Characteristic | Lymph nodal status (event-positive vs. -negative) |
|---|---|
| Histological tumor subtype | p=0.31344* (NS) |
| Grade | p=0.19669* (NS) |
| Tumor size | p=0.23763* (NS) |
| Depth of invasion | p=0.310^ (NS) |
| LVSI | p=0.02278* (S) |
Legend: LVSI - lymphovascular space invasion; NS - non-significant; S - significant (p<0.05): *chi-square test; ^t-student test; p - p value.
Table 4.
Lymph nodal burden and localisation of the event-positive (either MAC, MIC or ITC) lymph nodes.
Table 4.
Lymph nodal burden and localisation of the event-positive (either MAC, MIC or ITC) lymph nodes.
|
Patient |
FIGO stage (2018-) |
Maximal lesion type |
Total maximal lymph node burden (mm) |
Minimal lymph node burden (mm |
Maximal lymph node burden (mm) |
Localisation of lymph node events | |||||||
| Right external iliac nodes | Left external iliac nodes | Right obturator | Left obturator | Right common iliac | Left common iliac | Paraaortic | Parametrial | ||||||
| TM | 1b2 | MAC | 18.3 | 0.3 | 7.0 | MAC, MIC | MAC, MIC | 0 | 0 | 0 | 0 | 0 | MAC, MIC |
| WJ | 1b2 | ITC | <0.2 | N/A | N/A | 0 | ITC | 0 | ITC | 0 | 0 | 0 | 0 |
| JMM | 1b2 | ITC | <0.2 | N/A | N/A | ITC | 0 | ITC | 0 | 0 | 0 | 0 | 0 |
| KTM | 1b2 | ITC | <0.2 | N/A | N/A | ITC | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| PMH | 1b1 | MIC | 2.8 | N/A | 1.6 | 0 | 0 | 0 | MIC | 0 | MIC, ITC | 0 | 0 |
| JL | 1b1 | ITC | <0.2 | N/A | N/A | 0 | ITC | 0 | ITC | 0 | ITC | 0 | ITC |
| SD | 1b2 | MAC | 34.0 | 2.0 | 13.0 | MAC, MIC | MAC | MAC, MIC | MAC | 0 | 0 | 0 | 0 |
| P-OE | 1b2 | MAC | 106.0 | 2.0 | 17.0 | 0 | MAC, MIC | MAC, MIC | MAC | MIC | MAC | 0 | 0 |
| OS | 1b1 | MAC | 2.5 | 2.5 | 2.5 | 0 | 0 | MAC | 0 | 0 | 0 | 0 | 0 |
| BM | 1b2 | MIC | 0.25 | 0.25 | 0.25 | MIC | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| MSW | 1b2 | MAC | 12.5 | 0.3 | 10.0 | MIC | MAC, MIC | 0 | 0 | 0 | MIC | MIC | 0 |
Legend: ITC - isolated tumor cells; MAC - macrometastasis; MIC - micrometastasis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



