
Submitted:
11 December 2025
Posted:
12 December 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
The COVID-19 pandemic created a natural experiment to assess air quality responses to emission reductions, yet evidence from Latin American coastal industrial cities remains scarce. This study examined how meteorological variability modulated the effects of COVID-19 restrictions on air quality in Ilo, a medium-sized coastal industrial city in southern Peru (~67,000 inhabitants). We analyzed daily concentrations of PM10, PM2.5, NO2, O3, and SO2 across six pandemic phases (January–December 2020) using multiple linear regression, variance decomposition, and Random Forest models. A health impact assessment translated PM2.5 changes into cardiovascular mortality estimates using Global Burden of Disease 2021 coefficients. Despite reduced anthropogenic activity, PM2.5 increased by 34% during early reopening (May–June: 16.9 vs. 12.6 µg/m³ baseline), whereas NO2 decreased consistently (13–19%), SO2 declined up to 65%, and O3 more than doubled (+108%) in austral winter. Variance decomposition revealed that O₃ variability was almost entirely meteorology-driven (98%), while PM2.5 and NO2 showed balanced contributions from meteorology and restrictions (~50% each). The PM2.5 increase corresponded to approximately 3 additional cardiovascular deaths per 100,000 population annually. Coastal meteorology can counteract emission reductions, generating counterintuitive air quality responses and underscoring the need for meteorological normalization in policy evaluation.

Keywords:
COVID-19
; air quality
; PM2.5
; ozone
; meteorological normalization
; Random Forest
; health impact assessment
; cardiovascular mortality
; coastal city
; Peru
1. Introduction
Atmospheric pollution by fine particulate matter (PM2.5) is one of the leading environmental risk factors for global public health. Recent estimates from the Global Burden of Disease (GBD) 2021 indicate that ambient PM2.5 exposure was responsible for around 7.8 million deaths and over 230 million disability-adjusted life years (DALYs) worldwide, with the greatest burdens occurring in settings with lower socio-demographic development indices [1,2]. In the Latin America and Caribbean (LAC) region, cardiovascular diseases (CVD) remain the primary cause of mortality and disability; in 2021, an estimated 22.2 million CVD DALYs were reported, of which about 12% were attributable to particulate matter pollution [3]. Despite this growing evidence base, comprehensive policy frameworks targeting urban transport related air pollution in LAC are still less developed than in other regions [4].
The COVID-19 pandemic, declared a global health emergency by the World Health Organization on 11 March 2020, triggered unprecedented public health interventions affecting approximately 3.9 billion people across 157 countries through mobility restrictions and economic lockdowns [5,6]. These measures imposed substantial socioeconomic costs including deep economic contraction, unemployment, and disruptions in healthcare services but simultaneously created a unique natural experiment to assess air-quality responses to rapid, large-scale emission reductions across multiple anthropogenic sectors [7,8]. By late March 2020, global daily CO₂ emissions had declined by about 17% relative to 2019 baselines, and many cities reported marked decreases in PM2.5, PM₁₀, nitrogen dioxide (NO₂), sulfur dioxide (SO₂), and carbon monoxide (CO) [9,10]. Systematic reviews and multi-city assessments consistently document substantial reductions in NO₂ (typically 20–70%) and moderate decreases in PM2.5 and PM₁₀ (7–60%), with particularly strong responses in some Asian and European cities [11,12,13,14,15,16,17]. In several locations, SO₂ and CO levels also fell sharply [18,19]. Modelling studies suggest that short-term air-quality improvements during lockdowns likely prevented tens of thousands of premature deaths, particularly in regions with high baseline pollution [20,21,22,23].
However, emerging evidence shows that air-quality responses to COVID-19 measures were highly heterogeneous in space and time, challenging the assumption that emission reductions automatically translate into proportional concentration decreases [24,25,26,27,28,29,30,31]. Meteorology strongly modulates urban air pollution, and comparative studies using meteorologically normalized baselines have demonstrated that crude lockdown-related improvements were often overestimated by 30–50% [23,24,25,32]. Approaches such as multiple linear regression, generalized additive models, and machine-learning methods (e.g., Random Forest) have been widely applied to separate meteorological from anthropogenic influences, highlighting that failing to account for weather can substantially bias estimates of intervention effects [23,24,25,26,33,34,35,36].
Ozone (O₃) provides a clear illustration of atmospheric chemical complexity under changing emissions. Many cities reported 10–50% O₃ increases during lockdowns despite large reductions in NOₓ and other precursors [37,38]. This counterintuitive behaviour reflects non-linear photochemistry in NOₓ-saturated, volatile organic compound (VOC)-limited regimes, where reduced NO emissions weaken the NO + O₃ → NO₂ + O₂ titration pathway and allow ozone to accumulate [37,38,39]. Secondary PM2.5 formation can also respond non-linearly to changes in NOₓ, SO₂, and VOC emissions, leading to episodes of severe haze even when primary emissions decline [40,41,42]. Overall, the COVID-19 period underscored the need for integrated, multi-pollutant strategies and for analytical frameworks that explicitly account for both atmospheric chemistry and meteorology [39,40,41,42].
In South America, lockdown-related air-quality changes have been less extensively documented than in Asia or Europe but show similarly complex patterns. In Lima, Peru, strict lockdown measures in March–April 2020 reduced PM₁₀ and PM2.5 concentrations by roughly 40–58% and 31–43%, respectively, and lowered NO₂ by nearly 50%, while O₃ increased by 11–170%, consistent with a VOC-limited regime in a dense urban environment [43]. In Santiago, Chile, lockdowns produced significant reductions in PM₁₀, PM2.5, and NOₓ yet were accompanied by a 63% increase in O₃ [44]. A satellite-based analysis of tropospheric NO₂ in 17 Latin American cities reported substantial declines in columns over Lima (−47.5%), Santiago (−36.1%), São Paulo (−27%), Rio de Janeiro (−23%), Quito (−18.6%), and Bogotá (−17.5%) [45]. Beyond the pandemic, an Andean case study in municipalities near Bogotá showed that urbanization and industrial pressures can sustain elevated PM₁₀ levels and hazardous trace-metal concentrations even during periods of reduced activity, with health-risk metrics for metals such as Cr(VI), As, and Co exceeding safety thresholds [46].
Despite the rapid expansion of COVID-19 air-quality literature over 2,000 articles published in 2020–2021, largely concentrated in journals such as Science of the Total Environment, Aerosol and Air Quality Research, and Air Quality, Atmosphere & Health [14] several important knowledge gaps remain. First, geographic coverage is strongly biased toward Asian (≈65%) and European (≈18%) megacities, whereas medium-sized cities in developing regions, particularly in Latin America and Africa, remain underrepresented (≈5% and 3%, respectively) [14,47,48]. This imbalance raises questions about the generalizability of findings from well-studied megacities to smaller urban centres with distinct emission profiles, meteorological regimes, and socioeconomic contexts. [29,30,31]Second, coastal industrial cities constitute an understudied urban typology: marine boundary layer processes, sea-breeze circulations, port and shipping emissions, and hygroscopic sea-salt aerosols create air-quality dynamics that differ substantially from those in continental settings [32,49,50,51,52,53,54]. Conventional source-apportionment techniques can misattribute sea-salt contributions if they do not adequately distinguish marine sodium and chloride from anthropogenic sources [55,56]. Third, comparatively few COVID-19 air-quality studies translate observed concentration changes into explicit public-health metrics such as attributable mortality or morbidity despite a robust epidemiological literature showing that PM2.5 health effects extend below current WHO guideline values and that seemingly modest changes of 2–5 μg/m³ can yield measurable cardiovascular and respiratory impacts at the population level [57,58,59,60,61,62,63]. Finally, understanding how air pollution evolves during the post-lockdown recovery period is critical for policy design: analyses in China suggest that although PM2.5 levels rebounded when economic activity resumed, they remained below pre-pandemic baselines in cities that achieved a “green recovery” combining economic growth with improved air quality [64].
This study addresses these gaps by analysing air-quality responses to COVID-19 restrictions in Ilo, a medium-sized (≈67,000 inhabitants) coastal industrial city in southern Peru. Ilo hosts a large copper-smelting complex, port operations, and fishing activities, resulting in a mixed emission landscape combining industrial point sources, traffic, and marine aerosols [65]. Peru implemented one of the strictest national lockdowns globally, beginning on 16 March 2020 and followed by successive phases of mobility restrictions and partial reopening throughout the remainder of 2020 [6,66]. In Ilo, continuous monitoring at two stations (urban-industrial and residential) provides hourly measurements of PM₁₀, PM2.5, NO₂, O₃, and SO₂, together with meteorological variables, enabling an integrated assessment of anthropogenic and meteorological drivers.
The primary objective of this study is to quantify the relative contributions of COVID-19 restriction measures and meteorological variability to observed air-quality changes in Ilo during 2020. Specifically, we (1) characterize pollutant distributions and temporal patterns across six pandemic phases (Pre-Pandemic, Strict Lockdown, Phases 1–4); (2) examine meteorological controls and phase-stratified dispersion relationships; (3) partition explained variance between meteorological predictors (temperature, wind speed, relative humidity) and COVID-19 phases using variance decomposition via nested multiple regression and ANOVA F-tests; (4) evaluate non-linear relationships and variable importance using Random Forest models that relax linearity assumptions; and (5) translate PM2.5 changes into cardiovascular mortality estimates using concentration–response functions from Latin American and global cohorts [51,52,58,59,60,61,62,67,68,69,70].
We hypothesize that: (H1) meteorological variability explains a substantial fraction of pollutant variance—especially for O₃ and other secondary pollutants—making meteorological normalization essential for interpreting intervention effects; (H2) coastal meteorology and marine aerosols can lead to muted or counterintuitive particulate responses, including potential PM2.5 increases during lockdown; (H3) traffic-related NO₂ exhibits robust decreases consistent with global observations, whereas SO₂ shows marked reductions linked to smelter operations; and (H4) even moderate PM2.5 changes during lockdown periods translate into measurable cardiovascular mortality impacts at the population level.
This work makes four main contributions to the COVID-19 air-quality and environmental-health literature. First, it provides one of the first comprehensive analyses from a Latin American coastal industrial city, helping to address the geographic underrepresentation of medium-sized urban centres in global COVID-19 air-quality research [4,14,47,67]. Second, it applies a variance-decomposition framework combining nested multiple regression, ANOVA F-tests, and Random Forest models to disentangle meteorological and anthropogenic drivers of pollutant variability, building on recent advances in meteorological normalization techniques [24,34,35,36,71]. Third, it explicitly translates PM2.5 changes into cardiovascular mortality estimates, responding to the relative scarcity of studies that quantify epidemiological consequences of COVID-19-related air-quality changes [57,58,59,60,61,62,63]. Fourth, by analysing six pandemic phases over the full calendar year 2020, it moves beyond simple pre-/during-lockdown contrasts and captures the dynamic evolution of air quality as restrictions tightened and progressively relaxed [20,23,52].
2. Materials and Methods
2.1. Study Area
The study was conducted in the city of Ilo, located in Ilo Province, Moquegua Region, in southwestern Peru (17°38′40″ S, 71°20′43″ W). Ilo is a medium-sized coastal city with approximately 66,000 inhabitants and an arid coastal-desert climate, characterized by very low annual rainfall (~3.4 mm) and a mean annual temperature of about 19 °C [72]. The local economy is dominated by copper smelting and refining, port operations related to mineral exports, and industrial-scale fishing, together with associated urban activities, resulting in a complex mixture of industrial and urban emission sources [73]. This coastal industrial setting shares characteristics with other port cities where marine boundary-layer dynamics, sea-breeze circulations, and shipping emissions create distinct air quality conditions [32,53,54].
2.2. Study Period and COVID-19 Phase Definition
The COVID-19 pandemic began in December 2019 and the Peruvian government adopted the first restrictions in March 2020. The study period covers January 1 to December 31, 2020, encompassing the full spectrum of COVID-19 restriction phases. Data from 2019 were used exclusively for instrument stability verification and seasonal consistency checks. The pandemic period was divided into six phases based on official government decrees [66]:
- Pre-Pandemic (January 1 to March 15, 2020), representing baseline conditions before mobility restrictions;
- Strict Lockdown (March 16 to May 3, 2020), characterized by mandatory home confinement, suspension of non-essential activities, and curfew enforcement;
- Phase 1 (May 4 to June 4, 2020), initial economic reactivation with limited activities;
- Phase 2 (June 5 to June 30, 2020), progressive reopening of additional sectors;
- Phase 3 (July 1 to September 26, 2020), broader economic reactivation; and
- Phase 4 (September 27 to December 31, 2020), advanced reopening with most sectors operational.
2.3. Data Sampling and Measurement
Hourly concentrations (µg/m³) of PM₁₀, PM2.5, NO₂, SO₂ and O₃ were measured from January 1, 2019 to December 31, 2020 at the fixed air-quality monitoring station of the National University of Moquegua (17°36′6.2″ S, 71°20′25.0″ W; Figure 1). Instrument types and reference methods for each pollutant are summarized in Table S5 (Supplementary Material). Concurrent meteorological variables—air temperature (°C), wind speed (m s⁻¹), wind direction (°) and relative humidity (%) were recorded using a compact automatic weather station (Campbell Scientific®). The site is located in an open area, free from nearby direct emission sources and major obstructions such as tall buildings or trees.
2.4. Data Preprocessing and Quality Control
Hourly concentrations of PM₁₀, PM2.5, NO₂, O₃, SO₂ and meteorological variables were retrieved from the UNAM monitoring station, focusing on the year 2020 (covering all COVID-19 restriction phases), while 2019 data were used only to verify instrument stability and seasonal consistency. Raw records had already undergone routine quality assurance by the network operator (calibration and range checks); we applied additional harmonized quality control, aggregating hourly values to daily means only when at least 18 valid hours (≥75% completeness) were available, and excluding days below this threshold for the corresponding variable. This threshold is consistent with WHO recommendations for daily averaging [74] and has been applied in similar COVID-19 air quality studies [24,34,75]. The COVID-19 calendar was encoded as a six-level factor according to the phases defined in Section 2.2, and continuous meteorological predictors were mean-centered and standardized prior to modelling to improve numerical stability and comparability of regression coefficients. The overall analytical framework integrating data preprocessing, statistical modeling, and health impact assessment is summarized in Figure 2. This methodological workflow illustrates the sequential stages from raw data inputs through variance decomposition to final health impact quantification, providing a roadmap for the analyses described in the following sections.
2.5. Statistical Analysis Framework
All statistical analyses were performed in R version 4.5.1 [76] using RStudio as the integrated development environment. The analytical framework combined descriptive statistics, multiple linear regression with variance decomposition, Random Forest models, and sensitivity analyses to disentangle the relative contributions of COVID-19 restriction periods and meteorological variability to air pollutant concentrations. This approach follows methodological advances in meteorological normalization demonstrated in recent COVID-19 air quality studies [24,34,35,36,71].
2.5.1. Descriptive Statistics
Descriptive statistics (mean, standard deviation, median, range) were calculated for each pollutant by pandemic phase. Distribution normality was assessed using Shapiro–Wilk tests and Q–Q plots. Differences in pollutant concentrations across phases were evaluated with Kruskal–Wallis tests, followed by Dunn's post-hoc tests with Benjamini–Hochberg correction when appropriate (α = 0.05). Temporal trends were visualized using locally weighted scatterplot smoothing (LOESS, span = 0.3) to capture non-linear patterns while limiting overfitting [77]. Spearman rank correlation coefficients (ρ) were computed to characterize associations between pollutants and meteorological variables, accounting for non-linear relationships and outliers.
Observed concentrations were compared against the 2021 World Health Organization Air Quality Guidelines [74]: PM₁₀ = 45 µg/m³ (24-hour), PM2.5= 15 µg/m³ (24-hour), NO₂ = 25 µg/m³ (24-hour), O₃ = 100 µg/m³ (8-hour peak), and SO₂ = 40 µg/m³ (24-hour). Exceedance frequencies were calculated for each pollutant and phase.
2.5.2. Multiple Linear Regression Models
To quantify the independent effects of COVID-19 restrictions on air quality while controlling for meteorological confounders, we fitted nested multiple linear regression models for each pollutant, allowing explicit partitioning of variance between competing explanatory factors [78]. This nested model approach enables formal statistical testing of whether COVID-19 restriction periods explain additional variance beyond meteorological variability, as recommended by recent comparative methodological studies [35,36].
- Model 1 (Meteorology-Only)Y = β₀ + β₁(Temperature) + β₂(WindSpeed) + β₃(Humidity) + ε
- Model 2 (Full Model with COVID-19 Periods)where Y denotes daily pollutant concentration, Temperature (°C), Wind Speed (m s⁻¹) and Humidity (%) are continuous meteorological predictors, and Period₂–₆ are binary indicators for pandemic phases (reference: Pre-Pandemic). The error term ε is assumed normally distributed with constant variance. Meteorological predictors were selected based on their established roles in dispersion and atmospheric chemistry: temperature modulates photochemical reaction rates and boundary layer stability, wind speed controls dilution and transport, and humidity influences gas-to-particle conversion and wet deposition [39]. These meteorological variables have been identified as key predictors in Random Forest-based meteorological normalization studies across diverse urban settings [34,36,54,71].Y = β₀ + β₁(Temperature) + β₂(WindSpeed) + β₃(Humidity) + Σβᵢ(Periodi) + ε
Model assumptions were checked using standard diagnostics: residuals versus fitted values (linearity and homoscedasticity), normal Q–Q plots (residual normality), scale–location plots (variance homogeneity) and residuals versus leverage (influential observations). Variance inflation factors (VIF < 5) confirmed absence of problematic multicollinearity among predictors [79].
2.5.3. Variance Decomposition and Effect Quantification
The relative contributions of COVID-19 restrictions versus meteorological variability were quantified through incremental R² comparison between nested models. The coefficient of determination (R²) represents the proportion of variance in pollutant concentrations explained by predictor variables [80]. This variance decomposition approach has been validated against more complex machine learning methods and shown to provide robust estimates of meteorological versus anthropogenic contributions [35].
- Meteorological contributionR² Meteo = R² Model1
- COVID-19 contributionR² COVID = R² Model2 - R² Model1
- Relative percentage contributions%Meteo = (R² Meteo / R² Model2) × 100%COVID = (R² COVID / R² Model2) × 100
The statistical significance of COVID-19 effects beyond meteorological variability was assessed using ANOVA F-tests comparing nested models [81]. The null hypothesis that COVID-19 periods provide no additional explanatory power beyond meteorology was tested at α = 0.05. Heteroscedasticity-robust standard errors [82] were computed to ensure valid inference when variance homogeneity assumptions were violated. Percentage changes in pollutant concentrations relative to the Pre-Pandemic baseline were calculated with 95% confidence intervals derived from standard errors of the mean, providing uncertainty estimates for observed reductions [83]:
- Percentage change%Changei = [(Meani – Mean PrePandemic) / Mean PrePandemic] × 100 ± 1.96 × SE diff
2.5.4. Random Forest Analysis
To complement parametric regression and assess non-linear relationships, Random Forest (RF) models were implemented for each pollutant using the randomForest package [84,85]. RF is an ensemble machine learning technique that constructs multiple decision trees through bootstrap aggregation and provides robust variable importance measures [86]. RF-based meteorological normalization has been shown to outperform linear methods in capturing synoptic-scale variations, particularly when meteorological changes dominate pollutant variability [35]. Recent studies have demonstrated the utility of RF for COVID-19 air quality assessments in cities ranging from megacities to medium-sized urban areas [34,36,75].
RF models included the same predictors as linear models (temperature, wind speed, humidity, and pandemic period as categorical factor). Each model was trained with 500 trees (ntree = 500), with mtry set to the default value of p/3 for regression (where p = number of predictors), and minimum node size of 5 observations. A random seed (set.seed = 123) was used to ensure reproducibility [87].
Out-of-bag (OOB) error rates quantified prediction accuracy without requiring separate validation sets, as each tree is trained on a bootstrap sample (~63% of data) and validated on remaining observations [85]. Variable importance was assessed using two metrics: (1) percent increase in mean squared error (%IncMSE) when a variable is randomly permuted, indicating prediction degradation when that variable is unavailable, and (2) total decrease in node impurities (IncNodePurity) from splits on each variable, measuring contribution to model accuracy [88]. Higher values indicate greater importance.
2.5.5. Sensitivity Analyses
Several sensitivity analyses were performed to assess the robustness of the results: (1) alternative temporal aggregation, by repeating the analyses with different minimum hourly data thresholds for daily averages (≥12, ≥18 and ≥20 valid hours); (2) seasonal stratification, by re-fitting the models separately for austral summer (December–February) and winter (June–August); (3) outlier treatment, by excluding observations exceeding 3 standard deviations from the mean; and (4) alternative meteorological controls, by extending the models to include atmospheric pressure and solar radiation to check that meteorological confounding was adequately controlled. These sensitivity approaches follow recommendations from recent methodological comparisons of COVID-19 air quality studies [24,35,75].
2.6. Health Impact Assessment
To quantify the public health implications of PM2.5 variations observed during different epidemiological periods, we applied the concentration-response function (CRF) model recommended by the World Health Organization [74]. This methodological approach allows estimation of changes in attributable mortality associated with modifications in atmospheric pollutant concentrations [58,62]. Similar health impact assessments have been conducted for COVID-19 air quality changes in multiple countries, demonstrating the applicability of this approach to pandemic-related exposure variations [63,64].
2.6.1. Concentration-Response Model
We implemented the standard log-linear model without threshold [74], expressed as:
- Relative Riskwhere RR represents relative risk, β is the risk coefficient per unit increase (1 μg/m³) in PM2.5, and ΔPM2.5 corresponds to the change in mean concentration relative to the pre-pandemic reference period [89]. The attributable fraction (AF) was calculated as:RR = exp(β × Δ PM2.5)
- Attributable FractionAF = (RR - 1) / RR
Annual attributable deaths were estimated as:
- Attributable Deathsfollowing established methods in environmental health impact assessment [90].Deaths = Population × Baseline_Mortality_Rate × AF
2.6.2. Epidemiological Parameters
We adopted a concentration–response coefficient of β = 0.00072 per 1 µg/m³ increase in PM₂.₅ (95% CI: 0.00059–0.00085) for cardiovascular mortality in adults, as reported by the Global Burden of Disease 2021 systematic analysis [2]. The GBD 2021 coefficient was selected as the primary estimate for three reasons: (1) it represents the most current meta-analytic synthesis, incorporating data through 2021 and methodological refinements in exposure assessment; (2) it has been validated for application across diverse regions, including Latin America, where recent analyses have employed this coefficient to estimate PM₂.₅-attributable cardiovascular burden [3,4]; and (3) it provides a conservative estimate compared to alternative sources (e.g., Pope et al. [93]: β = 0.00080; WHO 2021 [74]: β = 0.00076), reducing the risk of overestimating health impacts. The GBD 2021 coefficient represents a ~5% reduction from the GBD 2019 estimate (β = 0.00076), reflecting refinements in exposure assessment and outcome ascertainment [2]. To evaluate the sensitivity of our results to this choice, we repeated the health impact calculations using alternative β values from Burnett et al. [58], Pope et al. [93], and the WHO Air Quality Guidelines [74] (see Supplementary Figure S5). The baseline cardiovascular mortality rate was set at 120 deaths per 100,000 inhabitants per year, based on official statistics for the Moquegua region from the Peruvian Ministry of Health [91].
2.6.3. Population Estimation
The exposed population was estimated at 67,167 inhabitants based on the 2017 National Census [72], updated using demographic projections for 2019–2020. A homogeneous exposure of this population to ambient PM2.5 concentrations measured at the monitoring station was assumed, acknowledging this as a standard limitation of ecological exposure–response studies [92]. Although cardiovascular mortality risk is predominantly concentrated in adults aged ≥30 years (approximately 68% of the population), we applied the concentration–response function to the total population, consistent with the GBD 2021 comparative risk assessment methodology that estimates population-level attributable burden [2].
2.6.4. Comparative Periods
The health impact analysis was conducted across six COVID-19 periods: Pre-Pandemic (January 1 – March 15, 2020), Strict Lockdown (March 16 – May 3, 2020), and four progressive reopening phases (Phase 1: May 4 – June 4; Phase 2: June 5–30; Phase 3: July 1 – September 26; Phase 4: September 27 – December 31, 2020). For each period, the change in mean PM2.5 (ΔPM2.5) was calculated relative to the pre-pandemic baseline, enabling estimation of period-specific changes in attributable mortality linked to mobility restrictions and economic reactivation [23,68].
2.6.5. Uncertainty Analysis
Uncertainty associated with the estimates was evaluated using three complementary approaches: (1) analytical error propagation incorporating the variance of the β coefficient, (2) Monte Carlo simulations (n = 10,000) with probability distributions assigned to β and baseline mortality rates, and (3) sensitivity analyses varying β across its 95% confidence interval bounds and using alternative sources (Burnett et al. [58], GBD 2019 study [60], Pope et al. [93], WHO Air Quality Guidelines [74]) [94,95]. Final confidence intervals reflect the combined uncertainty of all model parameters.
2.6.6. Model Assumptions and Limitations
The health impact assessment relies on several key assumptions: (a) a log-linear, no-threshold relationship between PM2.5 and mortality, (b) applicability of β coefficients derived from international cohort studies to the local population, (c) uniform population exposure represented by ambient concentrations at the monitoring station, and (d) no major residual confounding from socioeconomic or behavioral factors not explicitly controlled [74,93]. These assumptions, common in environmental health impact assessments, may introduce exposure misclassification and residual confounding; their implications are considered in the interpretation of results. Recent studies have noted that lockdown-related PM2.5 changes in some regions did not translate to expected mortality reductions due to complex interactions between meteorology, secondary aerosol formation, and population exposure patterns [63].
2.7. Data Visualization
All figures were generated in R using ggplot2 [96]. Boxplots summarized pollutant distributions by pandemic phase with WHO 2021 guideline lines as references. Time series were plotted with LOESS smoothing and 95% confidence bands. Scatterplots showed pollutant–meteorology relationships, using viridis color scales for temperature coding [97]. Variance decomposition results were displayed as stacked bar charts, and percentage changes included 95% confidence intervals. Concentration-response curves were plotted following visualization approaches from global burden of disease assessments [51,58]. All graphics were exported at 600 dpi as TIFF (with embedded fonts) and PDF for publication-quality output.
2.8. Software and Reproducibility
All analyses were conducted in R version 4.5.1 [76] using RStudio as the integrated development environment. Data handling and visualization were performed with tidyverse [98] and related packages (lubridate for date manipulation [99], ggplot2 for graphics [96]). Random Forest models were implemented with the randomForest package [85]. The openair package was used for wind rose and polar plot analyses [100]. Fully annotated code for data preprocessing, statistical modeling, and figure generation is provided in the Supplementary Materials to ensure reproducibility [87]. Statistical significance was set at α = 0.05, and effect sizes (e.g., R²) are reported alongside p-values where relevant [101].
3. Results
3.1. Air Pollutant Concentrations Across COVID-19 Pandemic Phases
Table 1 summarizes descriptive statistics for daily concentrations of PM₁₀, PM2.5, NO₂, O₃, and SO₂ across the six study phases. During the pre-pandemic baseline, median PM₁₀ (48.1 µg/m³) already exceeded the WHO 2021 24-h guideline (45 µg/m³), while SO₂ exhibited high variability (range: 7.9–129.9 µg/m³), reflecting episodic emissions from the copper smelter. Contrary to global trends of improved air quality during lockdowns, particulate matter concentrations increased during restriction phases. PM2.5 peaked in Phase 1 (16.9 ± 6.1 µg/m³), representing a 34% increase relative to pre-pandemic levels, before declining below baseline in Phase 3 (10.9 ± 3.4 µg/m³). PM₁₀ showed similar patterns, with the highest median during Strict Lockdown (51.4 µg/m³) and the lowest in Phase 3 (33.6 µg/m³). In contrast, gaseous pollutants followed expected patterns of reduced concentrations. NO₂ decreased consistently across all phases, ranging from 4.7–5.1 µg/m³ compared to the pre-pandemic mean of 5.8 µg/m³. SO₂ showed the most pronounced decline, with Phase 4 concentrations (8.9 ± 0.8 µg/m³) representing a 65% reduction from baseline. O₃ exhibited a marked mid-year increase, with Phase 3 concentrations (30.3 ± 5.5 µg/m³) more than doubling pre-pandemic levels.
Of note, SO₂ and O₃ data availability was substantially reduced during Phase 4 due to instrument maintenance issues: SO₂ measurements were limited to nine consecutive days at the beginning of the phase (27 September–5 October 2020; n = 9), and O₃ data were available for only 19 days. The very low variability in SO₂ during this limited period (SD = 0.83 µg/m³) suggests consistently low emissions from the smelter complex; however, the reduced sample sizes should be considered when interpreting Phase 4 trends for these pollutants.
Figure 3 visualizes the distributional characteristics of pollutant concentrations across phases. PM₁₀ distributions consistently exceeded the WHO 24-h guideline (45 µg/m³), with median values above the threshold in all phases except Phase 3. For PM2.5, the guideline (15 µg/m³) was exceeded primarily during Phase 1, which also exhibited the widest interquartile range and highest outliers, indicating substantial day-to-day variability during early reopening. NO₂, O₃, and SO₂ remained below their respective WHO thresholds throughout the study period. Notably, SO₂ showed progressively narrower distributions from pre-pandemic to Phase 4, with reduced outlier frequency, suggesting more consistent (and lower) emissions from the smelter complex during later phases. O₃ displayed an opposite pattern, with expanding IQR and increasing medians from Strict Lockdown through Phase 3, consistent with enhanced photochemical production during winter months.
Figure 4 shows the temporal evolution of daily pollutant concentrations throughout 2020. LOESS-smoothed trends reveal distinct patterns for each pollutant class. PM₁₀ and PM2.5 exhibited similar trajectories: relatively stable during pre-pandemic and Strict Lockdown, peaking during Phases 1–2 (May–June), and declining to annual minima during Phase 3 (July–September) before partial recovery in Phase 4. Gaseous pollutants displayed contrasting temporal dynamics. NO₂ showed an immediate step-decrease at lockdown onset (mid-March) that persisted throughout the year, with day-to-day variability substantially reduced compared to the pre-pandemic period. SO₂ exhibited the most dramatic temporal pattern: high and erratic concentrations during pre-pandemic (reflecting episodic smelter emissions), followed by progressive decline and stabilization at low levels from Phase 2 onward. O₃ displayed a pronounced seasonal cycle, with concentrations increasing steadily from April through September (Phases 1–3) before declining in Phase 4, consistent with enhanced photochemical production during austral winter when reduced NOₓ favored ozone accumulation.
Figure 5 quantifies percentage changes in pollutant concentrations relative to the pre-pandemic baseline. The five pollutants exhibited markedly different response patterns to COVID-19 restrictions. NO₂ showed consistent reductions across all phases (−13% to −19%), with overlapping confidence intervals indicating sustained decreases regardless of restriction intensity. SO₂ displayed the largest and most progressive decline, exceeding −60% by Phases 3–4, reflecting reduced smelter operations. In contrast, O₃ increased substantially throughout the restriction period, peaking at +108% during Phase 3; this counterintuitive response is consistent with reduced NO titration in a NOₓ-saturated regime, where lower NO emissions allow ozone to accumulate. Particulate matter showed divergent patterns between phases. PM2.5 increased during Strict Lockdown (+15%) and Phase 1 (+34%), then declined below baseline in Phases 3–4 (−5% to −13%). PM₁₀ exhibited greater variability, with modest increases during Strict Lockdown (+4%) and Phase 2 (−2%), but substantial reductions during Phase 3 (−31%). The wide confidence intervals for PM₁₀ reflect high day-to-day variability influenced by meteorological conditions. Detailed percentage and absolute changes for all pollutants are provided in Supplementary Table S4.
3.2. Meteorological Conditions and Pollutant–Meteorology Relationships
Meteorological conditions varied systematically across phases, reflecting the austral seasonal transition from summer to winter (Figure 6). Temperature showed a clear declining trend from pre-pandemic (median ~25°C) through Phase 3 (median ~17°C), with Phase 3 exhibiting both the lowest values and narrowest distribution, before partial recovery in Phase 4. Relative humidity displayed an inverse pattern, increasing from pre-pandemic levels (~66%) to peak values during Phases 1–3 (>73%), consistent with the intensification of the coastal marine layer during cooler months. Solar radiation followed the expected seasonal cycle, with substantially reduced values and compressed distributions during Phases 1–3 (winter) compared to pre-pandemic and Phase 4 (summer). Wind speed showed less pronounced seasonality, though Phases 1–2 exhibited lower medians and occasional very low outliers that may have contributed to reduced pollutant dispersion during these periods. These systematic meteorological changes coincide temporally with the observed pollutant variations (Section 3.1), underscoring the need to account for weather-related confounding when attributing concentration changes to COVID-19 restrictions.
Correlation analysis (Supplementary Figure S2) revealed coherent relationships among meteorological variables and pollutants. PM₁₀ and PM2.5 were positively associated with temperature and negatively with wind speed, while O₃ showed strong negative correlations with NO₂ and humidity, consistent with photochemical suppression under cloudy conditions. These correlation structures supported the selection of temperature, wind speed, and humidity as covariates in subsequent regression models. Day-of-week patterns (Supplementary Figure S1) indicated that NO₂ exhibited a pronounced weekday–weekend contrast during pre-pandemic and Strict Lockdown periods, which largely disappeared during Phases 2–4, suggesting sustained reductions in vehicular activity beyond the initial lockdown. Phase-specific relationships between PM₁₀ and wind speed are shown in Figure 7. The wind–PM₁₀ association was not temporally stationary: during Pre-Pandemic (β = 3.69, ns) and Phase 3 (β = 0.52, ns), relationships were weak and non-significant, whereas Phases 1–2 exhibited strong negative slopes (β = −16.5 to −23.8, p < 0.05), indicating enhanced dispersion effects. This phase-dependent heterogeneity coincided with temperature differences visible in the color gradient—cooler conditions (purple points) dominated Phases 1–3, while warmer days (yellow points) characterized Pre-Pandemic and Phase 4. The reversal of the wind–PM₁₀ relationship underscores that meteorological effects on pollutant dispersion vary seasonally and cannot be assumed constant across the study period.
3.3. Relative Contributions of COVID-19 Restrictions and Meteorology
To disentangle meteorological from anthropogenic influences, we fitted nested multiple linear regression models: a meteorology-only model (temperature, wind speed, humidity) and a full model adding COVID-19 phase indicators. Variance decomposition and ANOVA results are summarized in Table 2 and visualized in Figure 8. The five pollutants exhibited distinct variance structures (Figure 8a). O₃ was almost entirely meteorology-driven, with 98.5% of explained variance attributable to weather variables; the marginal COVID-19 contribution (1.5%) was statistically significant (p = 0.005) but negligible in magnitude.
This pattern reflects the strong coupling between ozone photochemistry and seasonal meteorological cycles. PM2.5 showed the most balanced partitioning (52% meteorology, 48% COVID-19), indicating that both weather conditions and restriction phases contributed substantially to observed variability. NO₂ displayed a similar pattern, though slightly more meteorology-influenced (57% vs 43%). PM₁₀ was predominantly meteorology-controlled (85%), with restriction phases contributing only 15% of explained variance. For SO₂, the full model explained only about 23% of the total variance, with the majority of the explained component attributed to meteorology. The non-significant incremental contribution of COVID-19 periods (p = 0.44) and the large unexplained variance suggest that episodic smelter-related emissions and unmeasured synoptic factors dominate SO₂ variability beyond the resolution of our phase-based approach. This reflects high day-to-day variability driven by episodic smelter emissions not captured by either meteorological variPre-Pandemicables or phase definitions, resulting in limited statistical power despite large observed concentration changes. Model performance varied considerably across pollutants (Figure 8b). The full model explained 81% of O₃ variance but only 19–26% for other pollutants, indicating substantial unexplained variability likely driven by factors not included in the models (e.g., boundary layer height, synoptic patterns, source-specific emissions). ANOVA F-tests (Table 2) confirmed that COVID-19 phases added significant explanatory power beyond meteorology for four of five pollutants (PM₁₀: p = 0.045; PM2.5: p = 0.001; NO₂: p = 0.001; O₃: p = 0.005), with SO₂ being the exception. Full regression coefficients are provided in Supplementary Table S3; notably, all phases showed negative NO₂ coefficients (sustained reductions) and positive PM2.5 coefficients (elevated concentrations relative to baseline despite lockdowns). Random Forest models provided a complementary non-parametric assessment (Supplementary Figure S3, Table S1). Variable importance rankings were broadly consistent with regression-based decomposition: meteorological variables dominated for O₃ (>60% combined importance), while COVID-19 period and meteorology contributed comparably for PM2.5 and NO₂. This agreement between parametric and non-parametric approaches supports the robustness of our variance partitioning conclusions. Model fit and diagnostic statistics are summarized in Supplementary Table S2, and residual diagnostics (Supplementary Figure S4) confirmed that model assumptions were reasonably satisfied for all pollutants.
3.4. Health Impact Assessment of PM2.5 Changes
Given its well-established cardiovascular effects and the availability of robust concentration-response functions, PM2.5 was selected for health impact assessment. Figure 9 displays phase-specific PM2.5 concentrations, while Table 3 presents the corresponding relative risks and attributable mortality estimates for the population of Ilo.
The Pre-Pandemic mean PM2.5 concentration (12.6 ± 4.36 µg/m³) served as the reference baseline. This value already exceeded the WHO 2021 annual guideline (5 µg/m³) by more than two-fold, indicating that the population was exposed to health-relevant PM2.5 levels even before the pandemic. During the restriction phases, PM2.5 followed a biphasic pattern: concentrations increased during Strict Lockdown and Phases 1–2, peaking in Phase 1 (16.91 ± 6.14 µg/m³), before declining below baseline during Phases 3–4 (Figure 9). Notably, even the lowest phase mean (Phase 3: 10.91 µg/m³) remained above the WHO guideline, underscoring persistent exposure to potentially harmful PM2.5 levels throughout the study period.
Applying the GBD 2021 concentration-response coefficient (β = 0.00072 per 1 µg/m³), these concentration changes translated into quantifiable mortality impacts (Table 3, Figure 10). The elevated PM2.5 during Phase 1 yielded the highest relative risk (RR = 1.003) and an estimated 0.23 additional cardiovascular deaths per year—the largest attributable burden observed. The position of phase-specific PM2.5 concentrations along the integrated exposure–response curve (Supplementary Figure S6) illustrates how relatively small changes in the 10–20 µg/m³ range translate into measurable differences in cardiovascular risk.
Strict Lockdown and Phase 2 produced smaller but still positive attributable mortality (0.09 and 0.11 deaths, respectively). Conversely, the reduced PM2.5 concentrations during Phases 3 and 4 were associated with avoided mortality (−0.12 and −0.06 deaths, respectively), representing a protective effect relative to baseline conditions.
Although these absolute numbers appear small for a city of ~67,000 inhabitants, they reflect the epidemiological reality that PM2.5 health effects operate across entire populations and accumulate over time. When extrapolated to larger urban areas with similar exposure patterns, such increments could translate into dozens to hundreds of attributable deaths annually. Moreover, the confidence intervals around our estimates (Table 3) indicate that the true mortality burden during Phase 1 could have ranged from 0.15 to 0.34 additional deaths per year, representing meaningful uncertainty that should inform precautionary approaches to air quality management.
The net health impact across the full pandemic period was approximately neutral: the additional mortality attributable to elevated PM2.5 during early restriction phases was largely offset by avoided deaths during later phases when concentrations declined. However, this aggregate balance masks the temporal heterogeneity of health burdens and underscores that meteorologically-driven PM2.5 increases, even during periods of reduced anthropogenic emissions, can generate measurable public health consequences.
4. Discussion
4.1. Air Quality Responses to COVID-19 Measures in a Coastal Latin American City
The multi-pollutant response observed in Ilo only partially fits the global narrative of “cleaner air” during COVID-19 lockdowns. Most multi-city syntheses report sharp and widespread reductions in NO₂ (about 20–60%) and more modest, heterogeneous changes in particulate matter, with small decreases or even increases depending on local sources and meteorology [10,21,37,102]. In Ilo, we also detected persistent NO₂ reductions and substantial SO₂ declines consistent with traffic and industrial curtailment. Daily mean NO₂ decreased by 13–19% across all pandemic phases relative to the pre-pandemic baseline, while SO₂ concentrations fell by roughly 65% by Phase 4, with a marked tightening of the distribution and disappearance of high-emission episodes. In contrast, both PM₁₀ and PM2.5 increased during the early restriction phases—most notably during Phase 1, when PM2.5 rose from 12.6 ± 4.4 µg/m³ in the Pre-Pandemic period to 16.9 ± 6.1 µg/m³ (+34%) and PM₁₀ remained above the WHO 24-hour guideline in most days—despite reduced mobility and industrial activity. Similar counterintuitive PM responses have been reported in some European and Asian cities once meteorological confounding is accounted for, with increases attributed to changes in boundary-layer height, secondary formation, and non-traffic sources rather than to policy failure [12,24,38,102]. Our findings therefore reinforce that lockdowns acted as a “natural experiment” in which emissions, atmospheric chemistry, and meteorology interacted in complex, context-specific ways rather than producing uniform improvements.
The magnitude and persistence of NO₂ reductions in Ilo are comparable to those reported for other traffic-dominated urban areas, where mobility restrictions, teleworking, and behavioural changes produced large and sustained decreases in near-roadway NO₂ even beyond strict lockdown periods [21,37,102,103]. The progressive SO₂ decline, by contrast, is more typical of settings dominated by a small number of industrial point sources, where operational decisions at smelters or power plants drive most temporal variability [104]. Together, these patterns place Ilo within the broader Latin American experience, where studies in megacities such as Mexico City, São Paulo, and Lima have documented sharp NO₂ decreases, more moderate and spatially heterogeneous PM responses, and strong contrasts linked to local source mixes and meteorological regimes [43,44,103,104,105,106]. In our case, the combination of increased PM2.5 during early phases and large mid-year ozone increases (+108% in Phase 3 relative to Pre-Pandemic) underscores how coastal meteorology and photochemistry can partially offset or even reverse the air-quality benefits of short-term emission reductions.
4.2. Disentangling Restriction Measures and Meteorology: Pollutant-Specific Patterns
A central contribution of this work is the explicit variance decomposition of meteorological versus COVID-19 period effects. The nested regression results show that PM2.5 and NO₂ are controlled by a balance between emission changes and meteorology, whereas O₃ is overwhelmingly meteorologically driven and SO₂ is dominated by anthropogenic changes linked to smelter operation. Specifically, for PM2.5 the full model explained about one quarter of the total variance (R² ≈ 0.23), with approximately 52% of the explained variance attributable to meteorology and 48% to COVID-19 phases. For NO₂, the full model explained roughly 25.7% of variance, partitioned into ≈57% meteorological and 43% COVID-19 contributions. PM₁₀ was predominantly meteorology-controlled, with around 85% of explained variance attributable to weather and only 15% to restriction phases, consistent with a strong contribution from natural coarse-mode sources.
Ozone exhibited a different behaviour: the full model accounted for 81.2% of O₃ variance, of which 98.5% was explained by meteorology and only 1.5% by COVID-19 phases. Although this marginal COVID-19 contribution was statistically significant (p = 0.005), its magnitude was negligible compared with the dominant seasonal and meteorological controls. This hierarchy is consistent with process-based understanding: ozone production and loss are tightly coupled to temperature, solar radiation, humidity, and mixing depth, while NO₂ responds rapidly to changes in traffic and atmospheric dispersion; PM2.5 reflects a mixture of primary and secondary sources with both natural and anthropogenic components [24,38,42,102].
The strong meteorological control on O₃, combined with only a small but significant COVID-19 contribution, mirrors findings from regional and global analyses showing that ozone responses to lockdowns were modest and often opposite in sign to NO₂, with increases linked to reduced NO titration in VOC-limited regimes [21,37,38,102]. In Ilo, the U-shaped seasonal pattern higher O₃ in winter despite lower solar radiation—together with strong negative O₃–NO₂ correlations suggests a NOₓ-saturated coastal environment where reductions in NOₓ emissions favour ozone accumulation, particularly under stable, humid conditions. This behaviour underscores that NOₓ control strategies may increase O₃ in some coastal or port cities unless accompanied by VOC reductions, a phenomenon widely discussed in the COVID-19 literature [37,38,42].
For PM2.5, the nearly balanced partition between meteorology and COVID-19 periods is noteworthy. It implies that emission changes associated with mobility and industrial restrictions were large enough to be detectable even after controlling for seasonal meteorology, but that unfavourable conditions during austral autumn–winter (cooler temperatures, weaker winds, higher humidity) offset part of these benefits. The phase-dependent wind–PM₁₀ relationships, with strong negative slopes during Phases 1–2 and weak or non-significant associations in Pre-Pandemic and Phase 3, further highlight that dispersion effects varied across the year and cannot be assumed stationary. Similar behaviour has been reported in other coastal or port-influenced cities, where sea-salt aerosols, crustal dust, and secondary formation contribute importantly to PM loadings and are strongly modulated by boundary-layer dynamics [12,24,55,107,108].
The Random Forest analysis provides an important robustness check. Despite relaxing linearity assumptions and allowing for interactions, the non-parametric models yielded variable-importance rankings broadly consistent with the regression-based variance decomposition: meteorological variables dominated for O₃ (with temperature and humidity jointly accounting for more than 60% of RF importance), while meteorology and COVID-19 phase had comparable importance for PM2.5 and NO₂. COVID-19 period remained a key predictor across pollutants, even when non-linear effects were allowed. Together, these complementary approaches support the conclusion that, in Ilo, the air-quality impacts of COVID-19 restrictions cannot be interpreted without explicit consideration of meteorological variability [34,35,36,54,75].
4.3. Health Relevance and Implications for Air Quality Management
The health impact assessment translates the modest concentration changes observed for PM2.5 into concrete public-health metrics. Using concentration–response functions from the Global Burden of Disease framework [2] and large cohort studies, long-term exposure to PM2.5 in the 10–20 µg/m³ range typical of Ilo is associated with small but non-negligible increases in cardiovascular mortality risk [1,58,62,109]. In our data, the pre-pandemic mean PM2.5 concentration (12.6 ± 4.4 µg/m³) already exceeded the WHO 2021 annual guideline (5 µg/m³) by more than a factor of two, indicating that the population was exposed to health-relevant levels even before COVID-19.
During the restriction phases, PM2.5 followed a biphasic pattern: concentrations increased during Strict Lockdown and Phase 1, peaking in Phase 1 (16.9 ± 6.1 µg/m³), before declining below baseline during Phases 3 (10.9 ± 3.4 µg/m³) and 4 (12.0 ± 4.4 µg/m³). Applying the GBD 2021 coefficient (β = 0.00072 per 1 µg/m³), these concentration changes translated into an estimated 0.23 additional cardiovascular deaths per year during Phase 1 and smaller positive burdens during Strict Lockdown (0.09) and Phase 2 (0.11). Conversely, reduced PM2.5 concentrations during Phases 3 and 4 were associated with avoided deaths (−0.12 and −0.06 per year, respectively). While these absolute numbers are modest for a city of about 67,000 inhabitants, they illustrate that even apparently small concentration shifts of 3–5 µg/m³ can yield detectable changes in attributable mortality when applied to entire populations [62,63,90,110]. Scaling these patterns to larger coastal urban corridors would translate into tens to hundreds of additional or avoided deaths annually.
These findings reinforce three key points for air-quality and health policy. First, meteorologically driven increases in PM2.5 during periods of emission reduction can still generate measurable health burdens; evaluating interventions based solely on emissions or raw concentrations without meteorological normalization risks misinterpretation, including underestimation of risks associated with “unfavourable” weather. Second, the coexistence of clear benefits for gaseous pollutants (NO₂, SO₂) with ambiguous or adverse responses for PM underscores the need for multi-pollutant, source-specific strategies rather than single-pollutant approaches. In Ilo, complementary control of industrial SO₂, traffic-related NO₂, and sources contributing to PM2.5 (including secondary formation and marine-influenced components) will be needed to achieve meaningful health benefits. Third, the fact that all pandemic phases remained well above the WHO 2021 guideline for annual PM2.5, even in the “cleanest” period, underscores that substantial additional emission reductions—beyond those induced by temporary lockdowns—are required to align with health-protective targets [58,62,74,110].
4.4. Strengths, Limitations, and Future Directions
This study has several strengths. Methodologically, the combination of nested regression models, variance decomposition, and machine-learning variable-importance analysis provides a transparent and robust framework to quantify the relative roles of meteorology and policy interventions, complementing more traditional “before–after” comparisons that may be biased by weather conditions [12,24,34,35,36,102]. Substantively, the work adds evidence from a coastal, industrial Latin American city—a setting under-represented in the COVID-19 air-quality literature relative to Asia, Europe, and North America [103,106,110,113]. To our knowledge, this is one of the first studies in a medium-sized Latin American coastal industrial city that jointly (i) decomposes meteorological and COVID-19 phase contributions to multi-pollutant variability using both regression-based and Random Forest approaches, and (ii) translates phase-specific PM2.5 changes into cardiovascular mortality estimates. This dual focus on mechanistic drivers and health implications enhances the policy relevance of the findings.
At the same time, important limitations should be acknowledged. First, the analysis relies on a single urban monitoring site located at the National University of Moquegua, which may not capture intra-urban gradients near major roads, the port, or the smelter complex. Given that our health impact assessment assumes homogeneous population exposure, this spatial limitation warrants consideration. However, several factors support the representativeness of this site for Ilo's population (~67,000 inhabitants): (i) the city's compact urban area (~15 km²) and relatively flat coastal topography favor well-mixed atmospheric conditions; (ii) the monitoring station is situated in an open area free from local emission sources, representing background urban concentrations; and (iii) the dominant sea-breeze circulation promotes relatively uniform pollutant dispersion across the urban core [107,108]. Nevertheless, residents living near the smelter or port facilities may experience higher exposures than those captured by this central monitoring site. Future work combining fixed monitoring, mobile campaigns, and low-cost sensor networks could resolve spatial contrasts and identify micro-environments with disproportionate health risks [111]. Second, the meteorological characterization is constrained to standard surface variables; explicit treatment of boundary-layer height, synoptic circulation, and marine stratocumulus regimes using radiosonde, ceilometer, or reanalysis data—would refine attribution of seasonal patterns, particularly for ozone and PM [24,42,107]. Third, the health-impact assessment focuses on cardiovascular mortality and long-term concentration–response functions applied to relatively short phases; broader outcome spectra (respiratory mortality, hospital admissions, morbidity) and alternative short-term coefficients would provide a more complete picture of health burden [1,62,94,109].
Finally, the observational nature of the COVID-19 “experiment” limits causal inference: restrictions co-occurred with behavioural, economic, and climatic changes that cannot be fully disentangled. Integrating these empirical findings with source-apportionment (e.g., receptor models, chemical speciation), chemical-transport modelling, and remote sensing would allow more mechanistic attribution of pollutant responses to specific source categories and processes. Such work is particularly relevant for coastal industrial cities like Ilo, where port activities, shipping, smelting, traffic, and natural marine aerosols interact within a narrow coastal boundary layer [55,107,108,112].
Taken together, our results highlight that (i) meteorological normalization is indispensable for evaluating air-quality interventions, (ii) PM2.5, NO₂, and SO₂ respond differently to the same policy shock because of their distinct source and process controls, and (iii) even modest concentration changes around relatively low baselines can have non-trivial health implications. For Peru and other coastal cities in the global South, these lessons suggest that temporary mobility restrictions are insufficient to approach WHO PM2.5 guidelines; instead, sustained structural measures targeting industrial point sources, port emissions, traffic, and regional background pollution designed and evaluated within a meteorologically normalized, multi-pollutant framework will be required to achieve durable public-health benefits [4,106,113].
5. Conclusions
This study analysed air-quality responses to COVID-19 restrictions in Ilo, a medium-sized coastal industrial city in southern Peru, a setting underrepresented in global COVID-19 air-pollution research. Using multiple linear regression, variance decomposition, Random Forest models and a health impact assessment, we quantified how meteorology modulated the effects of mobility restrictions and industrial shutdowns on PM₁₀, PM2.5, NO₂, O₃ and SO₂ during six pandemic phases in 2020. Our results show pollutant-specific responses that challenge the notion of uniformly improved air quality during lockdowns. NO₂ decreased consistently by 13–19% and SO₂ by up to 65% under reduced smelter activity, yet PM2.5 increased by 34% during the early reopening phase (Phase 1) despite substantial reductions in traffic and industry. O₃ concentrations more than doubled (+108%) in austral winter, reflecting NOₓ-saturated coastal photochemistry. Variance decomposition indicated that O₃ was almost entirely meteorology-driven (≈98% of explained variance), whereas PM2.5 and NO₂ were jointly controlled by meteorology and COVID-19 phases (≈50% each), and SO₂ remained predominantly influenced by smelter emissions. Random Forest results were consistent with these control hierarchies. Translating PM2.5 changes into health metrics using Global Burden of Disease functions showed that a ≈4 µg/m³ increase in Phase 1 produced a small but measurable excess in cardiovascular mortality, while later decreases were associated with avoided deaths. However, PM2.5 levels in all phases remained above WHO 2021 guideline values, indicating that larger and more sustained emission reductions are needed to meet health-protective targets. Overall, our findings highlight that meteorological normalization, multi-pollutant strategies and coastal-specific management approaches are essential for designing and evaluating effective emission-control policies in Peru and other coastal cities of the global South.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Author Contributions: Conceptualization, J.A.V.Z. and M.R.F.R.; methodology, J.A.V.Z. and M.R.F.R.; formal analysis, J.A.V.Z. and L.A.P.S.; investigation, J.A.V.Z., L.A.P.S., D.A.T. and A.H.D.C.; data curation, L.A.P.S. and J.A.V.Z.; resources, M.R.F.R., D.A.T. and A.H.D.C.; health impact assessment and epidemiological framing, Y.M.C.C. and J.A.V.Z.; visualization, J.A.V.Z. and L.A.P.S.; writing—original draft preparation, J.A.V.Z.; writing—review and editing, J.A.V.Z., M.R.F.R., L.A.P.S., Y.M.C.C., D.A.T. and A.H.D.C.; supervision, M.R.F.R.; project administration, J.A.V.Z. and M.R.F.R.; funding acquisition, J.A.V.Z. and M.R.F.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Universidad Nacional de Moquegua (UNAM), Peru, through the research project “Variación espacio-temporal, composición química de los aerosoles atmosféricos y su impacto en el balance energético terrestre de la provincia de Ilo (zona costera del sur del Perú)” (Resolution R.C.O. N° 328-2024-UNAM-CO). The APC was funded by the Universidad Nacional de Moquegua (UNAM) via Canon Minero resources (“Peruvian mining canon funds”).
Institutional Review Board Statement
Institutional Review Board Statement: Not applicable. The study used aggregated environmental monitoring and mortality data with no individual-level identifiers, and therefore did not require ethical approval.
Informed Consent Statement
Informed Consent Statement: Not applicable.
Data Availability Statement
Data Availability Statement: The air quality and meteorological datasets analysed in this study were obtained from the environmental monitoring network operated by the Universidad Nacional de Moquegua (UNAM) in Ilo and are not publicly available due to institutional data-sharing agreements, but are available from the corresponding author on reasonable request. Population and cause-specific mortality data were derived from national statistics and the Global Burden of Disease 2021 study, which are publicly accessible from the respective data providers.
Acknowledgments
Acknowledgments: The authors thank the Universidad Nacional de Moquegua (UNAM) for logistical support and access to the air quality monitoring infrastructure in Ilo. We are also grateful to the local authorities of Ilo for facilitating site access and to the Global Burden of Disease and Oxford COVID-19 Government Response Tracker teams for making their datasets publicly available.
Conflicts of Interest
Conflicts of Interest: The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Fang, T.; Di, Y.; Xu, Y.; Shen, N.; Fan, H.; Hou, S.; et al. Temporal trends of particulate matter pollution and its health burden, 1990–2021, with projections to 2036: a systematic analysis for the global burden of disease study 2021. Front Public Health 2025, 13. [Google Scholar] [CrossRef] [PubMed]
- Brauer, M.; Roth, G.A.; Aravkin, A.Y.; Zheng, P.; Abate, K.H.; Abate, Y.H.; et al. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: a systematic analysis for the Global Burden of Disease Study 2021. The Lancet [Internet] 2024, 403, 2162–2203. Available online: https://linkinghub.elsevier.com/retrieve/pii/S0140673624009334. [CrossRef] [PubMed]
- Mendoza-Cano, O.; Vázquez-Yañez, A.; Trujillo, X.; Huerta, M.; Ríos-Silva, M.; Lugo-Radillo, A.; et al. Cardiovascular disease burden linked to particulate matter pollution in Latin America and the Caribbean: Insights from GBD 2021 and socio-demographic index analysis. Public Health 2025, 238, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Mangones, S.C.; Cuéllar-Álvarez, Y.; Rojas-Roa, N.Y.; Osses, M. Addressing urban transport-related air pollution in Latin America: Insights and policy directions. Latin American Transport Studies 2025, 3, 100033. [Google Scholar] [CrossRef]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020 [Internet]. 2020. Available online: https://www.who.int/es/news-room/speeches/item/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 28 October 2025).
- Hale, T.; Angrist, N.; Goldszmidt, R.; Kira, B.; Petherick, A.; Phillips, T.; et al. A global panel database of pandemic policies (Oxford COVID-19 Government Response Tracker). Nat Hum Behav. 2021, 5, 529–538. [Google Scholar] [CrossRef]
- Nicola, M.; Alsafi, Z.; Sohrabi, C.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; et al. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. In International Journal of Surgery; Elsevier Ltd, 2020; Vol. 78, pp. 185–193. [Google Scholar]
- International Monetary Fund. World Economic Outlook, April 2020: The Great Lockdown [Internet]. Washington, DC, USA. 2020. Available online: https://www.imf.org/en/publications/weo/issues/2020/04/14/weo-april-2020 (accessed on 28 August 2025).
- Le Quéré, C.; Jackson, R.B.; Jones, M.W.; Smith, A.J.P.; Abernethy, S.; Andrew, R.M.; et al. Temporary reduction in daily global CO2 emissions during the COVID-19 forced confinement. Nat Clim Chang. 2020, 10, 647–653. [Google Scholar] [CrossRef]
- Venter, Z.S.; Aunan, K.; Chowdhury, S.; Lelieveld, J. COVID-19 lockdowns cause global air pollution declines. The Proceedings of the National Academy of Sciences [Internet] 2020, 117. Available online: https://www.pnas.org. [CrossRef]
- Ravindra, K.; Singh, T.; Vardhan, S.; Shrivastava, A.; Singh, S.; Kumar, P.; et al. COVID-19 pandemic: What can we learn for better air quality and human health? In Journal of Infection and Public Health; Elsevier Ltd, 2022; Vol. 15, pp. 187–198. [Google Scholar]
- Beloconi, A.; Probst-Hensch, N.M.; Vounatsou, P. Spatio-temporal modelling of changes in air pollution exposure associated to the COVID-19 lockdown measures across Europe. Science of the Total Environment 2021, 787. [Google Scholar] [CrossRef]
- Addas, A.; Maghrabi, A. The impact of covid-19 lockdowns on air quality —a global review. Sustainability (Switzerland) 2021, 13. [Google Scholar] [CrossRef]
- Mehmood, K.; Mushtaq, S.; Bao, Y.; Saifullah Bibi, S.; Yaseen, M.; et al. The impact of COVID-19 pandemic on air pollution: a global research framework, challenges, and future perspectives. Environmental Science and Pollution Research 2022, 29, 52618–52634. [Google Scholar] [CrossRef]
- Gama, C.; Relvas, H.; Lopes, M.; Monteiro, A. The impact of COVID-19 on air quality levels in Portugal: A way to assess traffic contribution. Environ Res. 2021, 193. [Google Scholar] [CrossRef]
- Kumari, P.; Toshniwal, D. Impact of lockdown on air quality over major cities across the globe during COVID-19 pandemic. Urban Clim. 2020, 34. [Google Scholar] [CrossRef]
- Berman, J.D.; Ebisu, K. Changes in U.S. air pollution during the COVID-19 pandemic. Science of the Total Environment 2020, 739. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Tartarini, F. Changes in air quality during the COVID-19 lockdown in singapore and associations with human mobility trends. Aerosol Air Qual Res. 2020, 20, 1748–1758. [Google Scholar] [CrossRef]
- Siciliano, B.; Dantas, G.; da Silva, C.M.; Arbilla, G. Increased ozone levels during the COVID-19 lockdown: Analysis for the city of Rio de Janeiro, Brazil. Science of the Total Environment 2020, 737. [Google Scholar] [CrossRef] [PubMed]
- He, G.; Pan, Y.; Tanaka, T. The short-term impacts of COVID-19 lockdown on urban air pollution in China. Nat Sustain. 2020, 3, 1005–1011. [Google Scholar] [CrossRef]
- Liu, F.; Wang, M.; Zheng, M. Effects of COVID-19 lockdown on global air quality and health. Science of the Total Environment 2021, 755. [Google Scholar] [CrossRef]
- Mahato, S.; Pal, S.; Ghosh, K.G. Effect of lockdown amid COVID-19 pandemic on air quality of the megacity Delhi, India. Science of the Total Environment 2020, 730. [Google Scholar] [CrossRef]
- Venter, Z.S.; Aunan, K.; Chowdhury, S.; Lelieveld, J. Air pollution declines during COVID-19 lockdowns mitigate the global health burden. Environ Res. 2021, 192. [Google Scholar] [CrossRef]
- Shi, Z.; Song, C.; Liu, B.; Lu, G.; Xu, J.; Van Vu, T.; et al. Abrupt but smaller than expected changes in surface air quality attributable to COVID-19 lockdowns [Internet]. Sci. Adv. 2021, 7. Available online: https://www.science.org. [CrossRef]
- Petetin, H.; Bowdalo, D.; Soret, A.; Guevara, M.; Jorba, O.; Serradell, K.; et al. Meteorology-normalized impact of the COVID-19 lockdown upon NO2 pollution in Spain. Atmos Chem Phys. 2020, 20, 11119–11141. [Google Scholar] [CrossRef]
- Huang, X.; Ding, A.; Gao, J.; Zheng, B.; Zhou, D.; Qi, X.; et al. Enhanced secondary pollution offset reduction of primary emissions during COVID-19 lockdown in China. Natl Sci Rev. 2021, 8. [Google Scholar] [CrossRef] [PubMed]
- Collivignarelli, M.C.; Abbà, A.; Bertanza, G.; Pedrazzani, R.; Ricciardi, P.; Carnevale Miino, M. Lockdown for CoViD-2019 in Milan: What are the effects on air quality? Science of the Total Environment 2020, 732. [Google Scholar] [CrossRef]
- Wang, P.; Chen, K.; Zhu, S.; Wang, P.; Zhang, H. Severe air pollution events not avoided by reduced anthropogenic activities during COVID-19 outbreak. Resour Conserv Recycl. 2020, 158. [Google Scholar] [CrossRef]
- Chen, L.W.A.; Chien, L.C.; Li, Y.; Lin, G. Nonuniform impacts of COVID-19 lockdown on air quality over the United States. Science of the Total Environment 2020, 745. [Google Scholar] [CrossRef]
- Shakoor, A.; Chen, X.; Farooq, T.H.; Shahzad, U.; Ashraf, F.; Rehman, A.; et al. Fluctuations in environmental pollutants and air quality during the lockdown in the USA and China: two sides of COVID-19 pandemic. Air Qual Atmos Health 2020, 13, 1335–1342. [Google Scholar] [CrossRef]
- Guevara, M.; Jorba, O.; Soret, A.; Petetin, H.; Bowdalo, D.; Serradell, K.; et al. Time-resolved emission reductions for atmospheric chemistry modelling in Europe during the COVID-19 lockdowns. Atmos Chem Phys. 2021, 21, 773–797. [Google Scholar] [CrossRef]
- Huang, X.; Wang, Y.; Shang, Y.; Song, X.; Zhang, R.; Wang, Y.; et al. Contrasting the effect of aerosol properties on the planetary boundary layer height in Beijing and Nanjing. Atmos Environ. 2023, 308. [Google Scholar] [CrossRef]
- Wu, B.; Zhao, S.; Liu, Y.; Zhang, C. Do meteorological variables impact air quality differently across urbanization gradients? A case study of Kaohsiung, Taiwan, China. Heliyon 2025, 11. [Google Scholar] [CrossRef]
- Lv, Y.; Tian, H.; Luo, L.; Liu, S.; Bai, X.; Zhao, H.; et al. Meteorology-normalized variations of air quality during the COVID-19 lockdown in three Chinese megacities. Atmos Pollut Res. 2022, 13. [Google Scholar] [CrossRef]
- Qi, L.; Zheng, H.; Ding, D.; Wang, S. A comparison of meteorological normalization of PM2.5 by multiple linear regression, general additive model, and random forest methods. Atmos Environ. 2024, 338. [Google Scholar] [CrossRef]
- Wong, Y.J.; Yeganeh, A.; Chia, M.Y.; Shiu, H.Y.; Ooi, M.C.G.; Chang, J.H.W.; et al. Quantification of COVID-19 impacts on NO2 and O3: Systematic model selection and hyperparameter optimization on AI-based meteorological-normalization methods. Atmos Environ. 2023, 301. [Google Scholar] [CrossRef]
- Sicard, P.; De Marco, A.; Agathokleous, E.; Feng, Z.; Xu, X.; Paoletti, E.; et al. Amplified ozone pollution in cities during the COVID-19 lockdown. Science of the Total Environment 2020, 735. [Google Scholar] [CrossRef] [PubMed]
- Grange, S.K.; Lee, J.D.; Drysdale, W.S.; Lewis, A.C.; Hueglin, C.; Emmenegger, L.; et al. COVID-19 lockdowns highlight a risk of increasing ozone pollution in European urban areas. Atmos Chem Phys. 2021, 21, 4169–4185. [Google Scholar] [CrossRef]
- Seinfeld, J.H.; Pandis, S.N. Atmospheric Chemistry and Physics: From Air Pollution to Climate Change, 3rd ed.; Wiley (John Wiley & Sons): Hoboken, NJ, USA, 2016. [Google Scholar]
- Le, T.; Wang, Y.; Liu, L.; Yang, J.; Yung, Y.L.; Li, G.; et al. Unexpected air pollution with marked emission reductions during the COVID-19 outbreak in China. Science (1979) [Internet] 2020, 702–706. Available online: https://www.science.org. [CrossRef] [PubMed]
- Zhao, N.; Wang, G.; Li, G.; Lang, J.; Zhang, H. Air pollution episodes during the COVID-19 outbreak in the Beijing–Tianjin–Hebei region of China: An insight into the transport pathways and source distribution. Environmental Pollution 2020, 267. [Google Scholar] [CrossRef]
- Kroll, J.H.; Heald, C.L.; Cappa, C.D.; Farmer, D.K.; Fry, J.L.; Murphy, J.G.; et al. The complex chemical effects of COVID-19 shutdowns on air quality. In Nature Chemistry; Nature Research, 2020; Vol. 12, pp. 777–779. [Google Scholar]
- Rojas, J.P.; Urdanivia, F.R.; Garay, R.A.; García, A.J.; Enciso, C.; Medina, E.A.; et al. Effects of COVID-19 pandemic control measures on air pollution in Lima metropolitan area, Peru in South America. Air Qual Atmos Health 2021, 14, 925–933. [Google Scholar] [CrossRef]
- Toro, A. R; Catalán, F; Urdanivia, FR; Rojas, JP; Manzano, CA; Seguel, R.; et al. Air pollution and COVID-19 lockdown in a large South American city: Santiago Metropolitan Area, Chile. Urban Clim. 2021, 36. [Google Scholar] [CrossRef]
- Volke, M.I.; Abarca-del-Rio, R.; Ulloa-Tesser, C. Impact of mobility restrictions on NO2 concentrations in key Latin American cities during the first wave of the COVID-19 pandemic. Urban Clim. 2023, 48. [Google Scholar] [CrossRef]
- Ramírez-Melgarejo, M.; Reyes-Figueroa, A.D.; Gassó-Domingo, S.; Güereca, L.P. Analysis of empirical methods for the quantification of N2O emissions in wastewater treatment plants: Comparison of emission results obtained from the IPCC Tier 1 methodology and the methodologies that integrate operational data. Science of the Total Environment 2020, 747. [Google Scholar] [CrossRef]
- Rodríguez-Urrego, D.; Rodríguez-Urrego, L. Air quality during the COVID-19: PM2.5 analysis in the 50 most polluted capital cities in the world. In Environmental Pollution; Elsevier Ltd, 2020; Vol. 266. [Google Scholar]
- Otmani, A.; Benchrif, A.; Tahri, M.; Bounakhla, M.; Chakir, E.M.; El Bouch, M.; et al. Impact of Covid-19 lockdown on PM10, SO2 and NO2 concentrations in Salé City (Morocco). Science of the Total Environment 2020, 735. [Google Scholar] [CrossRef] [PubMed]
- Quinn, P.K.; Collins, D.B.; Grassian, V.H.; Prather, K.A.; Bates, T.S. Chemistry and Related Properties of Freshly Emitted Sea Spray Aerosol. In Chemical Reviews; American Chemical Society, 2015; Vol. 115, pp. 4383–4399. [Google Scholar]
- O’Dowd, C.D.; De Leeuw, G. Marine aerosol production: A review of the current knowledge. Vol. 365, Philosophical Transactions of the Royal Society A: Mathematical, Physical and Engineering Sciences. Royal Society; 2007. p. 1753–1774.
- Duan, Y.; Wang, M.; Shen, Y.; Yi, M.; Fu, Q.; Chen, J.; et al. Influence of ship emissions on PM2.5 in Shanghai: From COVID19 to OMICRON22 lockdown episodes. Atmos Environ. 2023, 315. [Google Scholar] [CrossRef]
- Aas, W.; Fagerli, H.; Alastuey, A.; Cavalli, F.; Degorska, A.; Feigenspan, S.; et al. Trends in Air Pollution in Europe, 2000–2019. Aerosol Air Qual Res. 2024, 24. [Google Scholar] [CrossRef]
- Hong, Y.; Xu, X.; Liao, D.; Zheng, R.; Ji, X.; Chen, Y.; et al. Source apportionment of PM2.5 and sulfate formation during the COVID-19 lockdown in a coastal city of southeast China. Environmental Pollution 2021, 286. [Google Scholar] [CrossRef]
- Antonio Durán, R.E.; Cortez-Huerta, M.; Sosa Echeverría, R.; Fuentes García, G.; César Valdez, E.; Kahl, J.D.W. Random Forest approach to air quality assessment for port emissions in a coastal area in the Gulf of Mexico. Mar Pollut Bull. 2026, 222. [Google Scholar] [CrossRef]
- Wu, X.; Kong, Q.; Lan, Y.; Sng, J.; Yu, L.E. Refined Sea Salt Markers for Coastal Cities Facilitating Quantification of Aerosol Aging and PM2.5 Apportionment. Environ Sci Technol. 2024, 58, 8432–8443. [Google Scholar] [CrossRef]
- Ravindra, K.; Stranger, M.; Van Grieken, R. Chemical characterization and multivariate analysis of atmospheric PM 2.5 particles. J Atmos Chem. 2008, 59, 199–218. [Google Scholar] [CrossRef]
- Bashir, M.F.; Ma, B.; Bilal Komal, B.; Bashir, M.A.; Tan, D.; et al. Correlation between climate indicators and COVID-19 pandemic in New York, USA. Science of the Total Environment 2020, 728. [Google Scholar] [CrossRef]
- Burnett, R.; Chen, H.; Szyszkowicz, M.; Fann, N.; Hubbell, B.; Pope, C.A.; et al. Global estimates of mortality associated with longterm exposure to outdoor fine particulate matter. Proc Natl Acad Sci U S A 2018, 115, 9592–9597. [Google Scholar] [CrossRef]
- Di, Q.; Wang, Y.; Zanobetti, A.; Wang, Y.; Koutrakis, P.; Choirat, C.; et al. Air Pollution and Mortality in the Medicare Population. New England Journal of Medicine 2017, 376, 2513–2522. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Risk Factors Collaborators. Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet [Internet] 2020, 396, 1135–1159. Available online: www.thelancet.com.
- Fann, N.; Lamson, A.D.; Anenberg, S.C.; Wesson, K.; Risley, D.; Hubbell, B.J. Estimating the National Public Health Burden Associated with Exposure to Ambient PM2.5 and Ozone. Risk Analysis 2012, 32, 81–95. [Google Scholar] [CrossRef]
- Cohen, A.J.; Brauer, M.; Burnett, R.; Anderson, H.R.; Frostad, J.; Estep, K.; et al. Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. The Lancet 2017, 389, 1907–1918. [Google Scholar] [CrossRef]
- Ma, Y.; Nobile, F.; Marb, A.; Dubrow, R.; Kinney, P.L.; Peters, A.; et al. Air pollution changes due to COVID-19 lockdowns and attributable mortality changes in four countries. Environ Int. 2024, 187. [Google Scholar] [CrossRef]
- Feng, T.; Du, H.; Lin, Z.; Chen, X.; Chen, Z.; Tu, Q. Green recovery or pollution rebound? Evidence from air pollution of China in the post-COVID-19 era. J Environ Manage 2022, 324. [Google Scholar] [CrossRef] [PubMed]
- Olson, E.; Michalski, G.; Welp, L.; Larrea Valdivia, A.E.; Reyes Larico, J.; Salcedo Peña, J.; et al. Mineral dust and fossil fuel combustion dominate sources of aerosol sulfate in urban Peru identified by sulfur stable isotopes and water-soluble ions. Atmos Environ. 2021, 260. [Google Scholar] [CrossRef]
- Presidencia del Consejo de Ministros. Decreto Supremo N° 044-2020-PCM que declara Estado de Emergencia Nacional por las graves circunstancias que afectan la vida de la Nación a consecuencia del brote del COVID-19 [Internet]. Lima, Peru, 2020. Available online: https://cdn.www.gob.pe/uploads/document/file/566448/DS044-PCM_1864948-2.pdf?v=1584330685 (accessed on 4 June 2025).
- Bauwens, M.; Compernolle, S.; Stavrakou, T.; Müller, J.F.; van Gent, J.; Eskes, H.; et al. Impact of Coronavirus Outbreak on NO2 Pollution Assessed Using TROPOMI and OMI Observations. Geophys Res Lett. 2020, 47. [Google Scholar] [CrossRef]
- Tobías, A.; Carnerero, C.; Reche, C.; Massagué, J.; Via, M.; Minguillón, M.C.; et al. Changes in air quality during the lockdown in Barcelona (Spain) one month into the SARS-CoV-2 epidemic. Science of the Total Environment 2020, 726. [Google Scholar] [CrossRef]
- Singh, J.; Tyagi, B. Transformation of air quality over a coastal tropical station chennai during covid-19 lockdown in India. Aerosol Air Qual Res. 2021, 21. [Google Scholar] [CrossRef]
- Hopke, P.K. Review of receptor modeling methods for source apportionment. Vol. 66, Journal of the Air and Waste Management Association. Taylor and Francis Inc.; 2016. p. 237–259.
- Wu, Q.; Li, T.; Zhang, S.; Fu, J.; Seyler, B.C.; Zhou, Z.; et al. Evaluation of NOx emissions before, during, and after the COVID-19 lockdowns in China: A comparison of meteorological normalization methods. Atmos Environ. 2022, 278. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Estadística e Informática (INEI). Censos Nacionales 2017: XII de Población, VII de Vivienda y III de Comunidades Indígenas [Internet]. Lima. 2018. Available online: https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1539/libro.pdf (accessed on 14 September 2025).
- Boon, R.G.J.; Alexaki, A.; Becerra, E.H. The Ilo Clean Air Project: a local response to industrial pollution control in Peru. Environ Urban [Internet] 2001, 13. Available online: http://www.ihs.nl. [CrossRef]
- WHO global air quality guidelines. Particulate matter (PM2.5 and PM10) ozone, nitrogen dioxide, sulfur dioxide and carbon monoxide [Internet]. 2021. Available online: https://www.who.int/publications/i/item/9789240034228 (accessed on 28 September 2025).
- Wijnands, J.S.; Nice, K.A.; Seneviratne, S.; Thompson, J.; Stevenson, M. The impact of the COVID-19 pandemic on air pollution: A global assessment using machine learning techniques. Atmos Pollut Res. 2022, 13. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing [Internet]; R Foundation for Statistical Computing: Vienna, Austria, 2025; Available online: https://www.gnu.org/copyleft/gpl.html.
- Cleveland, W.S.; Devlin, S.J. Locally weighted regression: An approach to regression analysis by local fitting. J Am Stat Assoc. 1988, 83, 596–610. [Google Scholar] [CrossRef]
- Cohen, J.; Cohen, P.; West, S.G.; Aiken, L.S. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences, Third Edition. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences, Third Edition [Internet]. 2013, pp. 1–704. Available online: https://www.taylorfrancis.com/books/mono/10.4324/9780203774441/applied-multiple-regression-correlation-analysis-behavioral-sciences-jacob-cohen-patricia-cohen-stephen-west-leona-aiken (accessed on 28 November 2025).
- James Gareth Witten Daniela Hastie Trevor Tibshirani Robert An introduction to statistical learning : with applications in, R. Springer : Springer Science+Business Media; 2017. 426 p.
- Kutner, MH.; Chris, Nachtsheim; John, Neter; William, Li. Applied linear statistical models; McGraw-Hill Irwin, 2005; p. 1396 p. [Google Scholar]
- Chambers, J.M. Hastie Travor Statistical models in, S; Chapman & Hall, 1993. [Google Scholar]
- White, H. A HETEROSKEDASTICITY CONSISTENT COVARIANCE MATRIX ESTIMATOR AND A DIRECT TEST FOR HETEROSKEDASTICITY. Econometrica 1980, 48. [Google Scholar] [CrossRef]
- Cumming, G.; Finch, S. Inference by eye confidence intervals and how to read pictures of data. American Psychologist 2005, 60, 170–180. [Google Scholar] [CrossRef]
- Breiman, L. Random Forests. Mach Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Liaw, A.; Wiener, M. Classification and Regression by randomForest. R News [Internet] 2002, 2. Available online: http://www.stat.berkeley.edu/.
- Bickel, P.; Diggle, P.; Fienberg, S.; Gather, U.; Olkin, I.; Zeger, S. The Elements of Statistical Learning: Data Mining, Inference, and Prediction [Internet], 2nd ed.; Springer: New York, NY, USA, 2009; Available online: http://www.springer.com/series/692.
- Sandve, G.K.; Nekrutenko, A.; Taylor, J.; Hovig, E. Ten Simple Rules for Reproducible Computational Research. In PLoS Computational Biology; Public Library of Science, 2013; Vol. 9. [Google Scholar]
- Louppe, G.; Wehenkel, L.; Sutera, A.; Geurts, P. Understanding variable importances in forests of randomized trees. In 27th Conference on Neural Information Processing Systems (NIPS 2013) [Internet]; Curran Associates Inc.: Red Hook, NY, 2013; pp. 431–439. (accessed on 11 September 2025). [Google Scholar]
- Apte, J.S.; Marshall, J.D.; Cohen, A.J.; Brauer, M. Addressing Global Mortality from Ambient PM2.5. Environ Sci Technol. 2015, 49, 8057–8066. [Google Scholar] [CrossRef] [PubMed]
- Khomenko, S.; Cirach, M.; Pereira-Barboza, E.; Mueller, N.; Barrera-Gómez, J.; Rojas-Rueda, D.; et al. Premature mortality due to air pollution in European cities: a health impact assessment. Lancet Planet Health 2021, 5, e121–34. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Salud del Perú (MINSA). Análisis de Situación de Salud del Perú 2019 [Internet]. Centro Nacional de Epidemiología, Prevención y Control de Enfermedades: Lima, Peru, 2019. 2019. Available online: https://www.dge.gob.pe/portalnuevo/publicaciones/analisis-de-situacion-de-salud/ (accessed on 23 August 2025).
- Krewski, D.; Jerrett, M.; Burnett, R.T.; Ma, R.; Hughes, E.; Shi, Y.; et al. Extended Follow-Up and Spatial Analysis of the American Cancer Society Study Linking Particulate Air Pollution and Mortality; Health Effects Institute: Boston, MA, 2009; Volume 140, pp. 5–114. [Google Scholar]
- Pope, C.A.; Dockery, D.W. Health effects of fine particulate air pollution: Lines that connect. J Air Waste Manage Assoc. 2006, 56, 709–742. [Google Scholar] [CrossRef]
- Orellano, P.; Reynoso, J.; Quaranta, N.; Bardach, A.; Ciapponi, A. Short-term exposure to particulate matter (PM10 and PM2.5), nitrogen dioxide (NO2), and ozone (O3) and all-cause and cause-specific mortality: Systematic review and meta-analysis. Vol. 142, Environment International. Elsevier Ltd; 2020.
- Dockery, D.W.; Pope, C.A.; Xu, X.; Spengler John Ware, J.; Fay, M.; et al. AN ASSOCIATION BETWEEN AIR POLLUTION AND MORTALITY IN SIX U.S. CITIES. N Engl J Med. 1993, 329. [Google Scholar] [CrossRef] [PubMed]
- Wickham, Hadley. ggplot2 Elegant Graphics for Data Analysis [Internet], 2nd ed.; Houston, Texas, USA; Available online: http://www.springer.com/series/6991.
- Garnier, S; Ross, N; Rudis, boB; Filipovic-Pierucci, A; Galili, T; timelyportfolio; et al. sjmgarnier/viridis: CRAN release v0.6.3. 2025. Available online: https://zenodo.org/records/7890878 (accessed on 27 November 2025).
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.; François, R.; et al. Welcome to the Tidyverse. J Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Grolemund, G.; Wickham, H. Journal of Statistical Software Dates and Times Made Easy with lubridate [Internet]. 2011, Vol. 40. Available online: http://www.jstatsoft.org/.
- Carslaw, D.C.; Ropkins, K. openair — An R package for air quality data analysis. Environmental Modelling & Software 2012, 27–28, 52–61. [Google Scholar] [CrossRef]
- Sullivan, G.M.; Feinn, R. Using Effect Size—or Why the P Value Is Not Enough. J Grad Med Educ. 2012, 4, 279–282. [Google Scholar] [CrossRef]
- Gkatzelis, G.I.; Gilman, J.B.; Brown, S.S.; Eskes, H.; Gomes, A.R.; Lange, A.C.; et al. The global impacts of COVID-19 lockdowns on urban air pollution: A critical review and recommendations; University of California Press, 2021; Vol. 9, p. Elementa. [Google Scholar]
- Atiaga, O.; Páez, F.; Jácome, W.; Castro, R.; Collaguazo, E.; Nunes, L.M. COVID-19 pandemic impacted differently air quality in Latin American cities. Air Qual Atmos Health 2025, 18, 1919–1929. [Google Scholar] [CrossRef]
- Querol, X.; Massagué, J.; Alastuey, A.; Moreno, T.; Gangoiti, G.; Mantilla, E.; et al. Lessons from the COVID-19 air pollution decrease in Spain: Now what? Science of the Total Environment 2021, 779. [Google Scholar] [CrossRef]
- Velayarce, D.; Bustos, Q.; García, M.P.; Timaná, C.; Carbajal, R.; Salvatierra, N.; et al. Air Quality Analysis in Lima, Peru Using the NO2 Levels during the COVID-19 Pandemic Lockdown. Atmosphere (Basel) 2022, 13. [Google Scholar] [CrossRef]
- Gómez Peláez, L.M.; Santos, J.M.; de Almeida Albuquerque, T.T.; Reis, N.C.; Andreão, W.L.; de Fátima Andrade, M. Air quality status and trends over large cities in South America. Environ Sci Policy 2020, 114, 422–435. [Google Scholar] [CrossRef]
- Han, S.; Tang, Y.; Lu, M.; Yang, X.; Shi, J.; Cai, Z.; et al. Influence of coastal planetary boundary layer on PM2.5 with unmanned aerial vehicle observation. Atmos Res. 2023, 294. [Google Scholar] [CrossRef]
- Aswini, A.R.; Hegde, P. Impact assessment of continental and marine air-mass on size-resolved aerosol chemical composition over coastal atmosphere: Significant organic contribution in coarse mode fraction. Atmos Res. 2021, 248. [Google Scholar] [CrossRef]
- Vodonos, A.; Awad, Y.A.; Schwartz, J. The concentration-response between long-term PM2.5 exposure and mortality; A meta-regression approach. Environ Res. 2018, 166, 677–689. [Google Scholar] [CrossRef]
- Guan, Y.; Xiao, Y.; Wang, Y.; Zhang, N.; Chu, C. Assessing the health impacts attributable to PM2.5 and ozone pollution in 338 Chinese cities from 2015 to 2020. Environmental Pollution 2021, 287. [Google Scholar] [CrossRef]
- Patel, H.; Davy, P.; Tollemache, C.; Talbot, N.; Salmond, J.; Williams, D.E. Evaluating the efficacy of targeted traffic management interventions: A novel methodology for determining the composition of particulate matter in urban air pollution hotspots. Science of the Total Environment 2024, 951. [Google Scholar] [CrossRef]
- Anastasopolos, A.T.; Hopke, P.K.; Sofowote, U.M.; Mooibroek, D.; Zhang, J.J.Y.; Rouleau, M.; et al. Evaluating the effectiveness of low-sulphur marine fuel regulations at improving urban ambient PM2.5 air quality: Source apportionment of PM2.5 at Canadian Atlantic and Pacific coast cities with implementation of the North American Emissions Control Area. Science of the Total Environment 2023, 904. [Google Scholar] [CrossRef] [PubMed]
- Ramírez, O.; Gutiérrez-Ulloa, C.; Zarate, L.; Carrión, A.M.; Hernandez Guzman, A.; de la Rosa, J. Impact of urbanization and industrialization on PM10 in municipalities near megacities: A case study from an Andean Region, Latin America. Urban Clim. 2025, 64. [Google Scholar] [CrossRef]
Figure 1.
Geographic location of the study area and the fixed monitoring station at the National University of Moquegua (UNAM) in Ilo, Peru.
Figure 1.
Geographic location of the study area and the fixed monitoring station at the National University of Moquegua (UNAM) in Ilo, Peru.
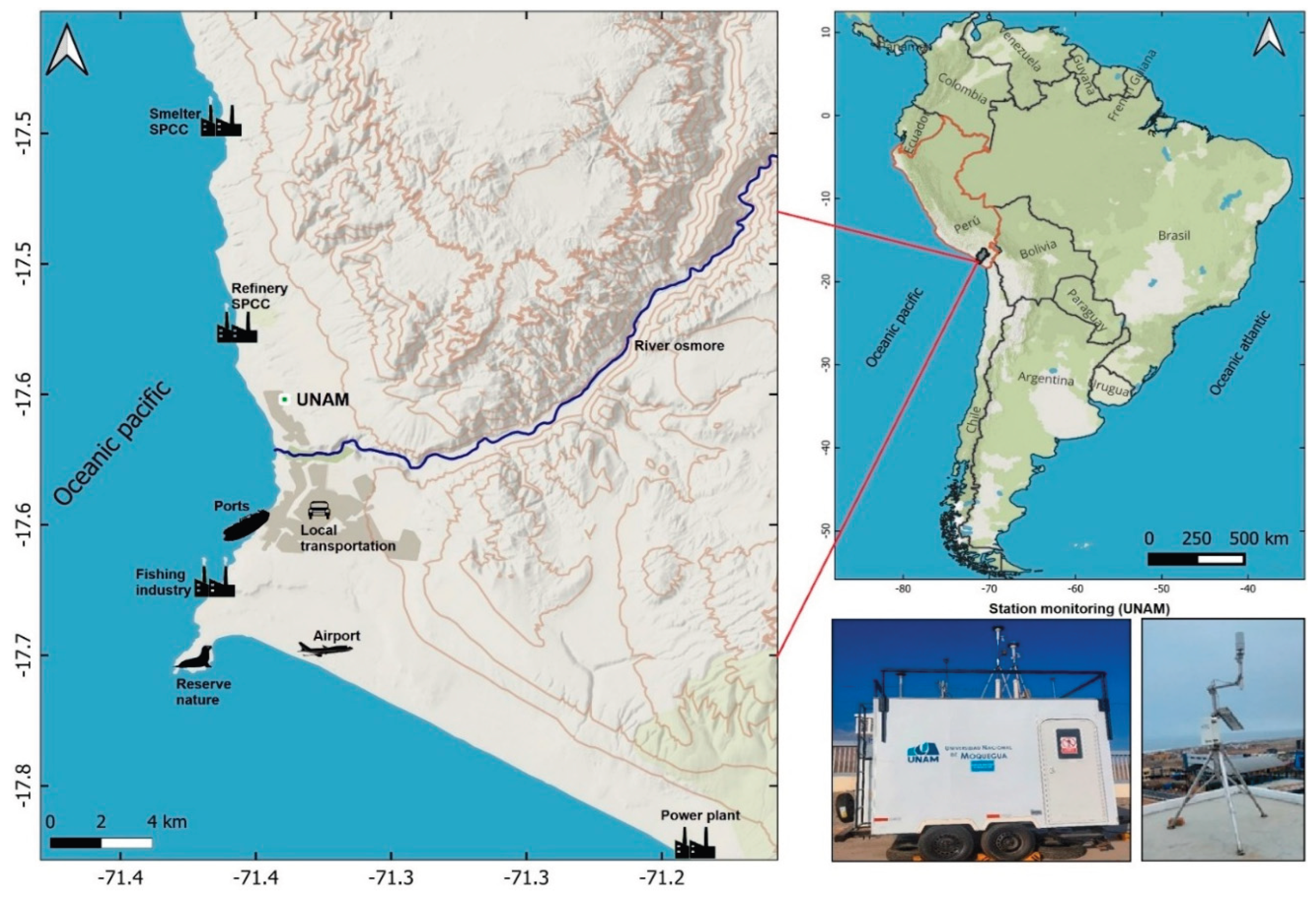
Figure 2.
Methodological framework for the variance decomposition and health impact assessment of COVID-19 lockdown effects on air quality in Ilo, Peru (2019–2020). Blue boxes represent data inputs; green indicates descriptive analysis (Section 3.1–3.2); orange represents variance decomposition and statistical modeling (Section 3.3); pink denotes health impact assessment (Section 3.4). Purple boxes indicate outputs (tables and figures). Arrows show the analytical workflow from data processing through final health impact quantification.
Figure 2.
Methodological framework for the variance decomposition and health impact assessment of COVID-19 lockdown effects on air quality in Ilo, Peru (2019–2020). Blue boxes represent data inputs; green indicates descriptive analysis (Section 3.1–3.2); orange represents variance decomposition and statistical modeling (Section 3.3); pink denotes health impact assessment (Section 3.4). Purple boxes indicate outputs (tables and figures). Arrows show the analytical workflow from data processing through final health impact quantification.
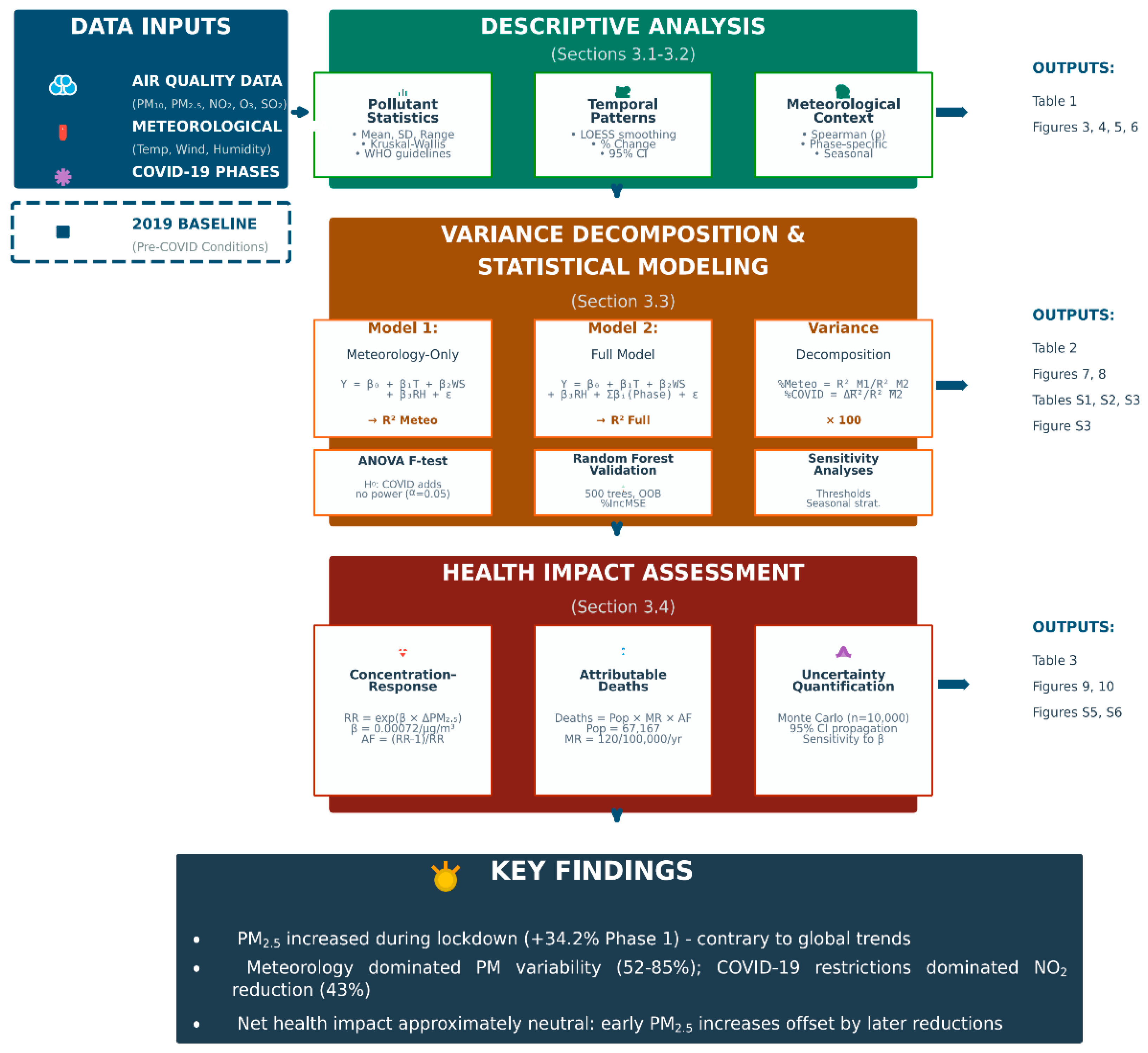
Figure 3.
Daily air pollutant concentrations during six COVID-19 pandemic phases in Ilo, Peru. Boxplots show distributions of daily mean concentrations of PM₁₀, PM2.5, NO₂, O₃, and SO₂. Boxes represent interquartile ranges (IQR), center lines indicate medians, whiskers extend to 1.5×IQR, and points represent outliers. Red dashed horizontal lines mark WHO (2021) 24-h air quality guideline values. Phase definitions are provided in Table 1.
Figure 3.
Daily air pollutant concentrations during six COVID-19 pandemic phases in Ilo, Peru. Boxplots show distributions of daily mean concentrations of PM₁₀, PM2.5, NO₂, O₃, and SO₂. Boxes represent interquartile ranges (IQR), center lines indicate medians, whiskers extend to 1.5×IQR, and points represent outliers. Red dashed horizontal lines mark WHO (2021) 24-h air quality guideline values. Phase definitions are provided in Table 1.
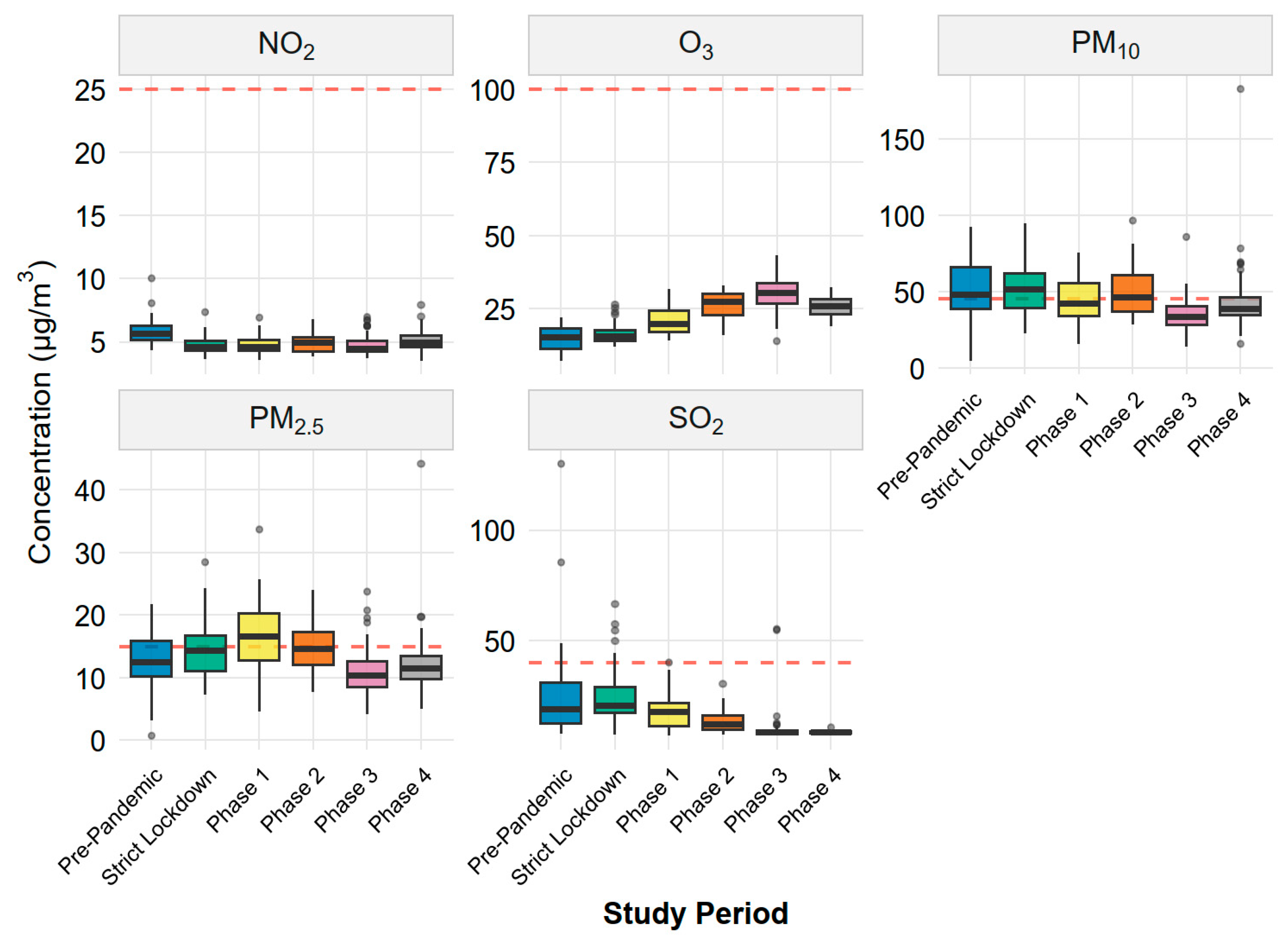
Figure 4.
Temporal evolution of daily air pollutant concentrations during the COVID-19 pandemic in Ilo, Peru. Daily mean concentrations (points) and LOESS-smoothed trends (solid lines; span = 0.3) are shown for PM₁₀, PM2.5, NO₂, O₃, and SO₂ throughout 2020. Vertical dashed lines indicate boundaries between the six COVID-19 phases. Phase color coding is shown in the legend.
Figure 4.
Temporal evolution of daily air pollutant concentrations during the COVID-19 pandemic in Ilo, Peru. Daily mean concentrations (points) and LOESS-smoothed trends (solid lines; span = 0.3) are shown for PM₁₀, PM2.5, NO₂, O₃, and SO₂ throughout 2020. Vertical dashed lines indicate boundaries between the six COVID-19 phases. Phase color coding is shown in the legend.
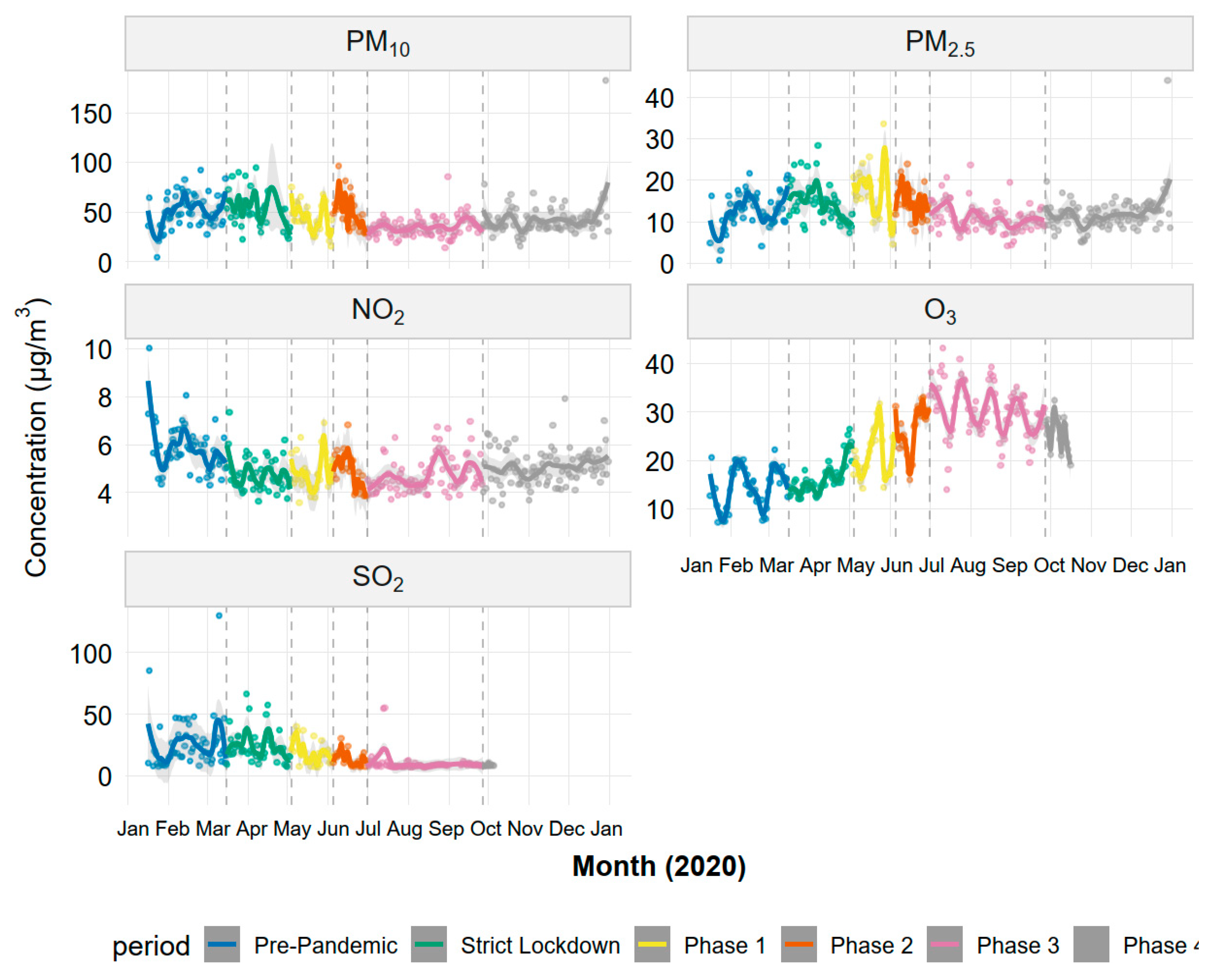
Figure 5.
Percentage change in daily air pollutant concentrations relative to the pre-pandemic baseline during COVID-19 restriction phases in Ilo, Peru. Panels show estimated percentage changes in mean concentrations of NO₂, O₃, PM₁₀, PM2.5, and SO₂ for each restriction phase compared with the Pre-Pandemic period (1 January–15 March 2020). Points represent mean percentage changes, and vertical error bars denote 95% confidence intervals. The horizontal black line marks zero change. Numeric labels display percentage values for each phase.
Figure 5.
Percentage change in daily air pollutant concentrations relative to the pre-pandemic baseline during COVID-19 restriction phases in Ilo, Peru. Panels show estimated percentage changes in mean concentrations of NO₂, O₃, PM₁₀, PM2.5, and SO₂ for each restriction phase compared with the Pre-Pandemic period (1 January–15 March 2020). Points represent mean percentage changes, and vertical error bars denote 95% confidence intervals. The horizontal black line marks zero change. Numeric labels display percentage values for each phase.
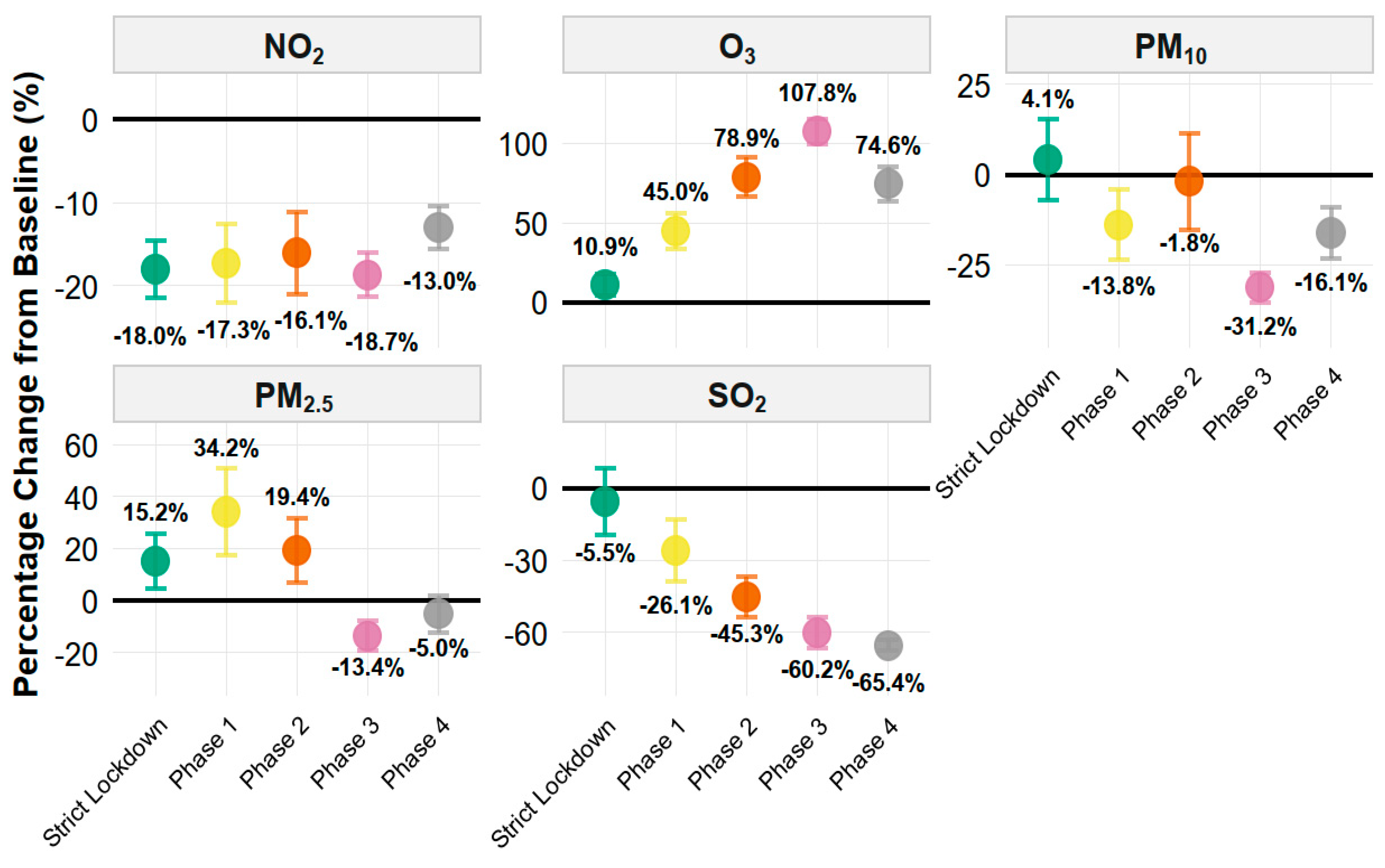
Figure 6.
Daily meteorological conditions during six COVID-19 pandemic phases in Ilo, Peru. Boxplots show the distributions of daily mean temperature (°C), wind speed (m s⁻¹), relative humidity (%), and solar radiation (W m⁻²) for each study phase. Boxplot elements represent interquartile range, median, whiskers to 1.5×IQR, and outliers. These meteorological variables were included as continuous covariates in the multiple regression models (see Section 3.3).
Figure 6.
Daily meteorological conditions during six COVID-19 pandemic phases in Ilo, Peru. Boxplots show the distributions of daily mean temperature (°C), wind speed (m s⁻¹), relative humidity (%), and solar radiation (W m⁻²) for each study phase. Boxplot elements represent interquartile range, median, whiskers to 1.5×IQR, and outliers. These meteorological variables were included as continuous covariates in the multiple regression models (see Section 3.3).
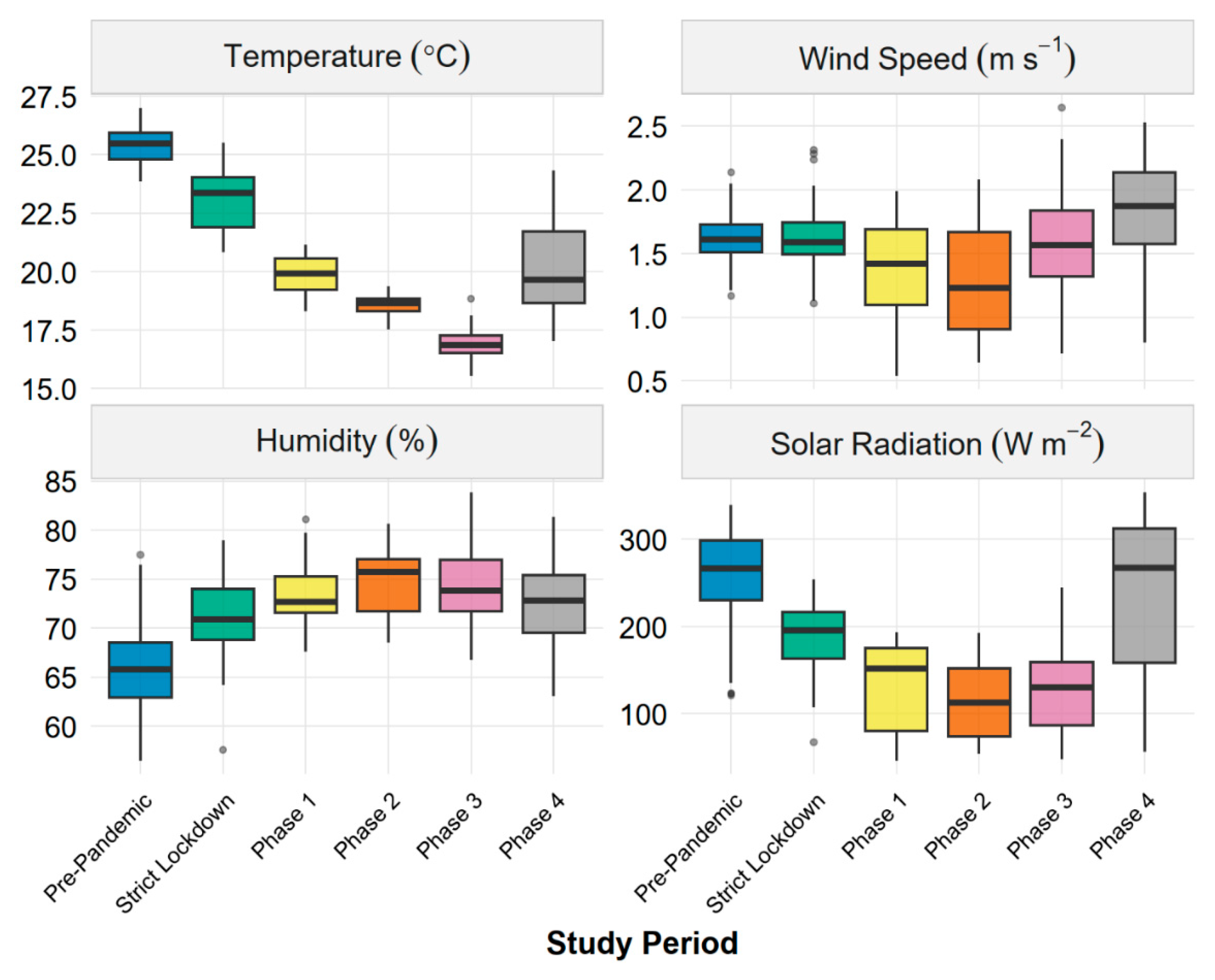
Figure 7.
Phase-specific relationships between daily PM₁₀ concentrations and wind speed during the COVID-19 pandemic in Ilo, Peru. Panels (a–f) show scatter plots for each study phase. Points represent daily mean values and are coloured by temperature (°C) using a plasma palette (cooler days in purple, warmer days in yellow). Red lines indicate ordinary least-squares regression fits with 95% confidence intervals (grey shaded bands). Insets report the regression slope β (µg m⁻³ per m s⁻¹), Spearman correlation coefficient ρ, and number of days n; asterisks denote statistically significant associations (p < 0.05).
Figure 7.
Phase-specific relationships between daily PM₁₀ concentrations and wind speed during the COVID-19 pandemic in Ilo, Peru. Panels (a–f) show scatter plots for each study phase. Points represent daily mean values and are coloured by temperature (°C) using a plasma palette (cooler days in purple, warmer days in yellow). Red lines indicate ordinary least-squares regression fits with 95% confidence intervals (grey shaded bands). Insets report the regression slope β (µg m⁻³ per m s⁻¹), Spearman correlation coefficient ρ, and number of days n; asterisks denote statistically significant associations (p < 0.05).
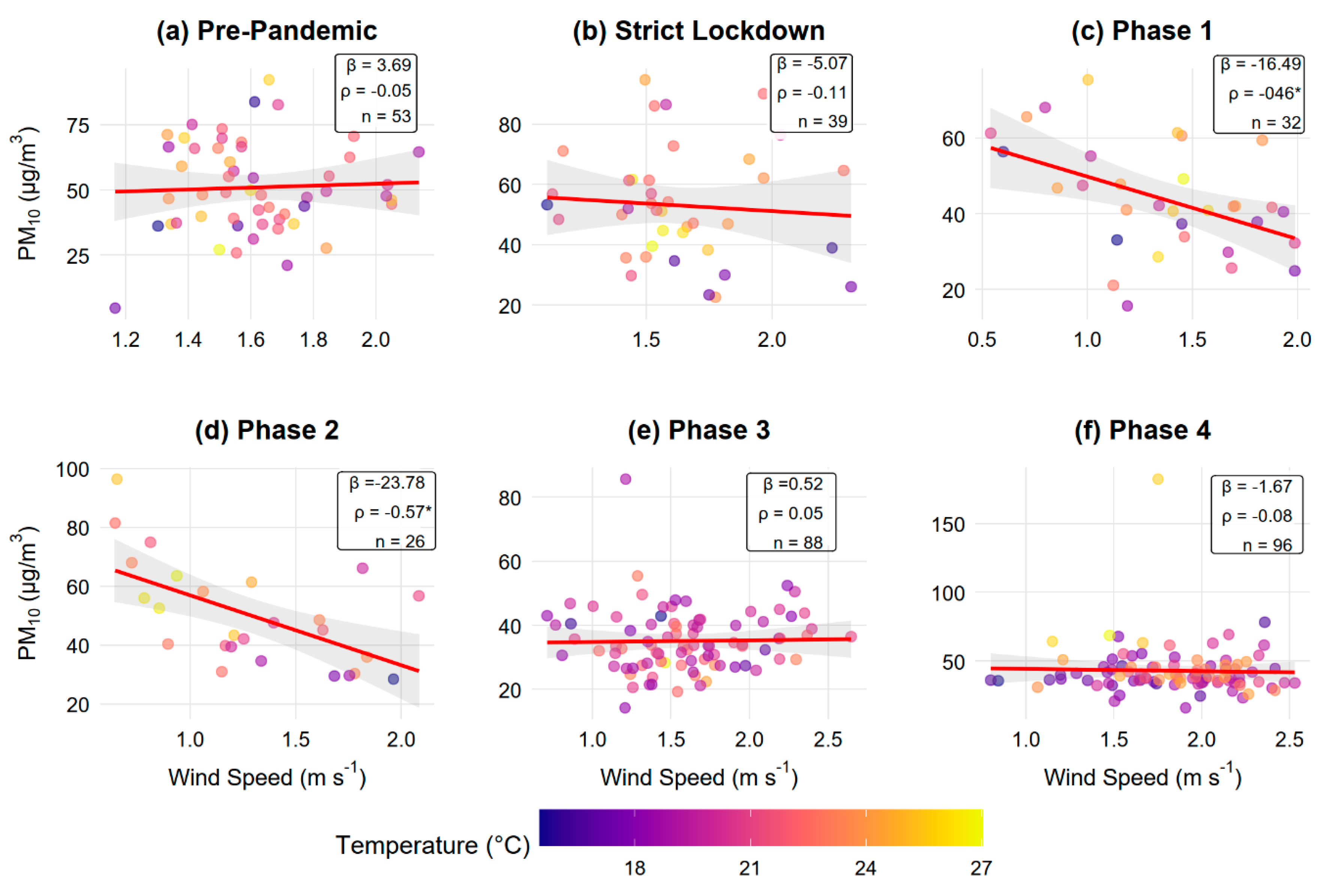
Figure 8.
Relative contributions of meteorology and COVID-19 restriction periods to variability in daily air pollutant concentrations in Ilo, Peru. (a) Variance decomposition based on multiple linear regression models. Grey bars represent unexplained variance (100 × (1 − R²)); blue and red segments show fractions of explained variance attributable to meteorology and COVID-19 periods, respectively. Percentages within the explained component are labeled. (b) Model performance comparison showing R² for meteorology-only models (light blue) and full models including COVID-19 phases (purple). Numeric labels indicate R² values.
Figure 8.
Relative contributions of meteorology and COVID-19 restriction periods to variability in daily air pollutant concentrations in Ilo, Peru. (a) Variance decomposition based on multiple linear regression models. Grey bars represent unexplained variance (100 × (1 − R²)); blue and red segments show fractions of explained variance attributable to meteorology and COVID-19 periods, respectively. Percentages within the explained component are labeled. (b) Model performance comparison showing R² for meteorology-only models (light blue) and full models including COVID-19 phases (purple). Numeric labels indicate R² values.
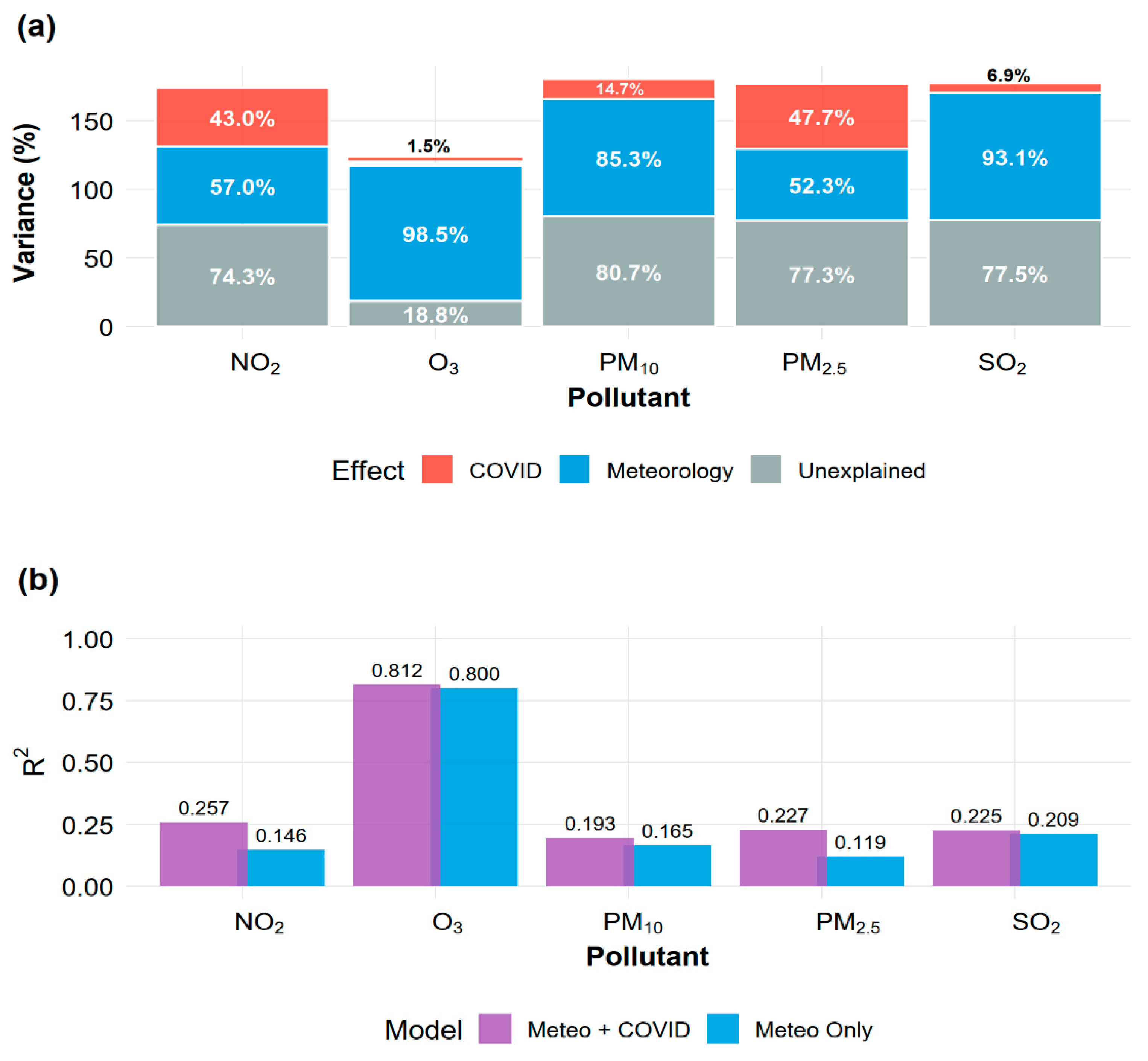
Figure 9.
Average PM2.5 concentrations by COVID-19 restriction phase in Ilo, Peru (2020). Bars represent mean daily PM2.5 concentrations (µg/m³) with error bars indicating ± 1 SD. Red dashed line: Pre-Pandemic baseline (12.60 µg/m³). Green dotted line: WHO 2021 annual guideline (5 µg/m³). Yellow dotted line: Peruvian national standard (25 µg/m³).
Figure 9.
Average PM2.5 concentrations by COVID-19 restriction phase in Ilo, Peru (2020). Bars represent mean daily PM2.5 concentrations (µg/m³) with error bars indicating ± 1 SD. Red dashed line: Pre-Pandemic baseline (12.60 µg/m³). Green dotted line: WHO 2021 annual guideline (5 µg/m³). Yellow dotted line: Peruvian national standard (25 µg/m³).
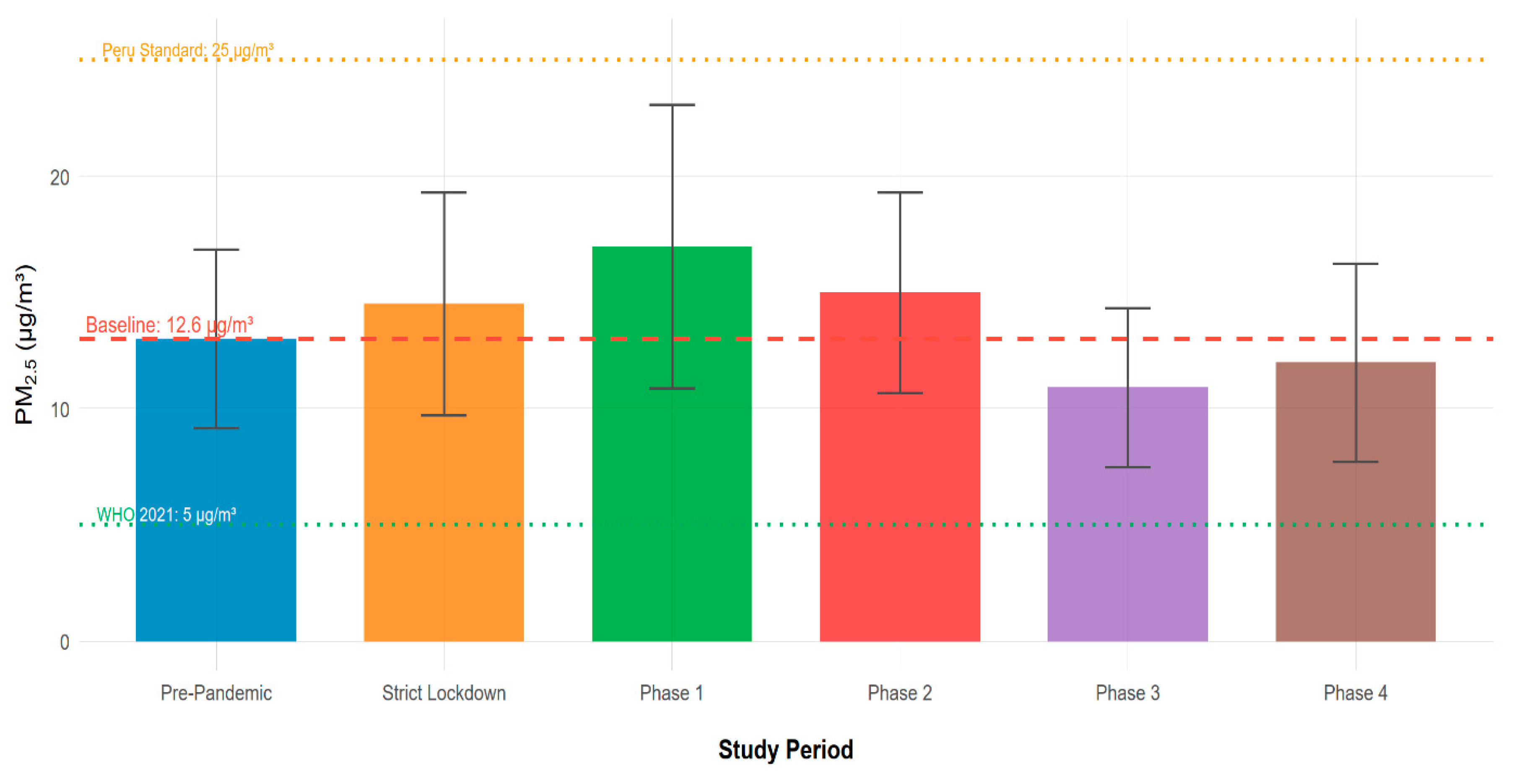
Figure 10.
Health impact assessment: PM2.5-attributable cardiovascular mortality by COVID-19 restriction phase in Ilo, Peru (2020). Bars represent estimated attributable deaths per year relative to Pre-Pandemic baseline, calculated using GBD 2021 concentration-response functions (β = 0.00072 per 1 µg/m³). Error bars indicate 95% confidence intervals. Red bars: additional deaths (increased PM2.5). Green bars: avoided deaths (reduced PM2.5). Numeric labels show point estimates with 95% CI.
Figure 10.
Health impact assessment: PM2.5-attributable cardiovascular mortality by COVID-19 restriction phase in Ilo, Peru (2020). Bars represent estimated attributable deaths per year relative to Pre-Pandemic baseline, calculated using GBD 2021 concentration-response functions (β = 0.00072 per 1 µg/m³). Error bars indicate 95% confidence intervals. Red bars: additional deaths (increased PM2.5). Green bars: avoided deaths (reduced PM2.5). Numeric labels show point estimates with 95% CI.
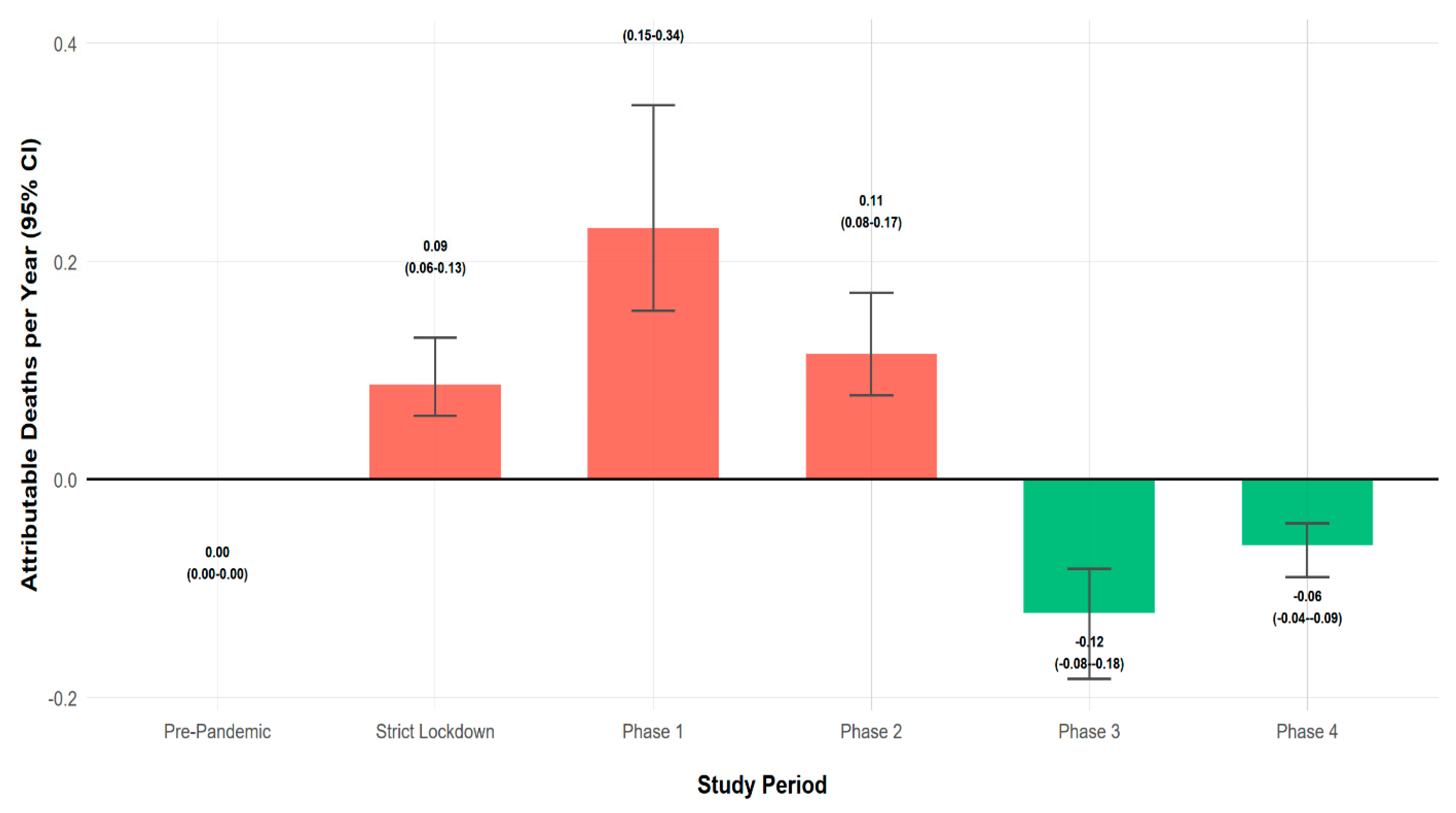

Table 1.
Descriptive statistics of daily air pollutant concentrations by COVID-19 pandemic phase in Ilo, Peru.
Table 1.
Descriptive statistics of daily air pollutant concentrations by COVID-19 pandemic phase in Ilo, Peru.
| Pollutant | Period | M (SD) | Mdn | Range | n |
|---|---|---|---|---|---|
| PM₁₀ | Pre-Pandemic | 50.93 (17.38) | 48.11 | 4.56–92.28 | 53 |
| PM₁₀ | Strict Lockdown | 53.04 (18.31) | 51.43 | 22.57–94.73 | 39 |
| PM₁₀ | Phase 1 | 43.90 (14.41) | 41.79 | 15.66–75.32 | 32 |
| PM₁₀ | Phase 2 | 50.00 (17.60) | 46.33 | 28.40–96.36 | 26 |
| PM₁₀ | Phase 3 | 35.07 (9.90) | 33.63 | 14.18–85.62 | 88 |
| PM₁₀ | Phase 4 | 42.74 (18.18) | 38.43 | 15.74–182.48 | 96 |
| PM2.5 | Pre-Pandemic | 12.60 (4.36) | 12.39 | 0.71–21.71 | 53 |
| PM2.5 | Strict Lockdown | 14.51 (4.70) | 14.23 | 7.33–28.42 | 49 |
| PM2.5 | Phase 1 | 16.91 (6.14) | 16.57 | 4.58–33.65 | 32 |
| PM2.5 | Phase 2 | 15.04 (4.06) | 14.61 | 7.74–23.96 | 26 |
| PM2.5 | Phase 3 | 10.91 (3.44) | 10.31 | 4.19–23.72 | 88 |
| PM2.5 | Phase 4 | 11.96 (4.40) | 11.48 | 5.08–44.13 | 96 |
| NO₂ | Pre-Pandemic | 5.81 (1.00) | 5.67 | 4.31–10.02 | 56 |
| NO₂ | Strict Lockdown | 4.77 (0.71) | 4.61 | 3.64–7.34 | 49 |
| NO₂ | Phase 1 | 4.81 (0.78) | 4.56 | 3.58–6.91 | 32 |
| NO₂ | Phase 2 | 4.88 (0.74) | 4.90 | 3.86–6.82 | 26 |
| NO₂ | Phase 3 | 4.73 (0.74) | 4.47 | 3.72–6.96 | 88 |
| NO₂ | Phase 4 | 5.06 (0.75) | 4.93 | 3.49–7.91 | 96 |
| O₃ | Pre-Pandemic | 14.59 (4.23) | 15.31 | 7.21–22.19 | 56 |
| O₃ | Strict Lockdown | 16.18 (3.38) | 15.44 | 12.03–26.45 | 49 |
| O₃ | Phase 1 | 21.15 (4.79) | 19.70 | 14.23–31.69 | 32 |
| O₃ | Phase 2 | 26.09 (4.75) | 27.25 | 15.98–33.09 | 26 |
| O₃ | Phase 3 | 30.31 (5.47) | 30.37 | 13.96–43.20 | 88 |
| O₃ | Phase 4 | 25.47 (3.56) | 25.80 | 19.02–32.40 | 19 |
| SO₂ | Pre-Pandemic | 25.57 (20.59) | 19.05 | 7.91–129.88 | 56 |
| SO₂ | Strict Lockdown | 24.17 (12.74) | 20.67 | 7.71–66.55 | 49 |
| SO₂ | Phase 1 | 18.90 (9.46) | 17.78 | 7.24–40.18 | 32 |
| SO₂ | Phase 2 | 14.00 (5.64) | 12.41 | 7.68–30.54 | 26 |
| SO₂ | Phase 3 | 10.18 (7.41) | 8.83 | 7.10–55.30 | 79 |
| SO₂ | Phase 4 | 8.85 (0.83) | 8.73 | 8.17–10.91 | 9 |
Note. M = mean; SD = standard deviation; Mdn = median; n = number of daily observations. All concentrations in µg/m³. Study phases: Pre-Pandemic (1 January–15 March 2020), Strict Lockdown (16 March–3 May), Phase 1 (4 May–4 June), Phase 2 (5–30 June), Phase 3 (1 July–26 September), Phase 4 (27 September–31 December). WHO 2021 24-h guideline values: PM₁₀ = 45 µg/m³, PM2.5= 15 µg/m³, NO₂ = 25 µg/m³, O₃ = 100 µg/m³ (8-h), SO₂ = 40 µg/m³. SO₂ and O₃ sample sizes in Phase 4 reflect reduced data availability due to instrument maintenance (SO₂: 27 September–5 October only; O₃: 19 days).
Table 2.
Relative contributions of meteorological variability and COVID-19 restriction periods to variance in daily air pollutant concentrations in Ilo, Peru.
Table 2.
Relative contributions of meteorological variability and COVID-19 restriction periods to variance in daily air pollutant concentrations in Ilo, Peru.
| Pollutant | n | R² | R² Meteo | R² COVID | % Meteo | % COVID | F (5, df₂) |
p |
|---|---|---|---|---|---|---|---|---|
| PM₁₀ | 334 | 0.193 | 0.165 | 0.029 | 85.3 | 14.7 | 2.30 | 0.045 |
| PM2.5 | 344 | 0.227 | 0.119 | 0.108 | 52.3 | 47.7 | 9.40 | 0.001 |
| NO₂ | 347 | 0.257 | 0.146 | 0.110 | 57.0 | 43.0 | 10.02 | 0.001 |
| O₃ | 271 | 0.812 | 0.800 | 0.013 | 98.5 | 1.5 | 3.49 | 0.005 |
| SO₂ | 251 | 0.225 | 0.209 | 0.015 | 93.1 | 6.9 | 0.96 | 0.440 |
Note. n = number of valid daily observations; R² = coefficient of determination for full model; R² Meteo = variance explained by meteorological variables only (temperature, wind speed, relative humidity); R² COVID = incremental variance explained by COVID-19 period indicators beyond meteorology; % Meteo and % COVID = relative percentage contributions to total explained variance (R²); F(5, df₂) = F statistic from ANOVA comparing nested models, where 5 = degrees of freedom for COVID-19 phases and df₂ = residual degrees of freedom; p = probability value. Reference category: Pre-Pandemic period (1 January–15 March 2020). Significant effects (p < 0.05) indicate that COVID-19 periods explain additional variance beyond meteorology.
Table 3.
Health impact assessment results by COVID-19 phase in Ilo, Peru (2020).
| Period | PM2.5 (μg/m³) | Δ PM2.5 (µg/m³) | % Change | RR (95% CI) |
Deaths (95% CI) |
|---|---|---|---|---|---|
| Pre-Pandemic | 12.60 ± 4.36 | 0 | 0 | 1.000 (1.000-1.000) | 0.00 (0.00-0.00) |
| Strict Lockdown | 14.51 ± 4.70 | 1.91 | 15.2 | 1.001 (1.001-1.001) | 0.09 (0.06-0.13) |
| Phase 1 | 16.91 ± 6.14 | 4.31 | 34.2 | 1.003 (1.002-1.003) | 0.23 (0.15-0.34) |
| Phase 2 | 15.04 ± 4.06 | 2.45 | 19.4 | 1.001 (1.001-1.002) | 0.11 (0.08-0.17) |
| Phase 3 | 10.91 ± 3.44 | - 1.69 | -13.4 | 0.998 (0.999-0.998) | -0.12 (-0.08--0.18) |
| Phase 4 | 11.96 ± 4.40 | - 0.63 | -5.0 | 0.999 (0.999-0.999) | -0.06 (-0.04--0.09) |
Note. PM2.5 values expressed as mean ± SD (µg/m³). Δ PM2.5 = absolute change relative to Pre-Pandemic baseline (µg/m³). % Change = percentage change in concentration relative to Pre-Pandemic. RR = Relative Risk calculated using concentration-response coefficient β = 0.00072 per 1 µg/m³ from GBD 2021. Deaths = estimated annual attributable cardiovascular deaths (95% CI). Positive values indicate additional mortality; negative values indicate avoided deaths. Population: 67,167 inhabitants (total population; GBD methodology); baseline cardiovascular mortality rate: 120 per 100,000 inhabitants/year.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



