
Submitted:
10 December 2025
Posted:
12 December 2025
You are already at the latest version
Abstract
Economic crises characterized by financial instability, rising unemployment, and austerity measures are known to have profound social and public health consequences. While their economic impacts are widely studied, their effects on mental health across diverse populations and geographic regions remain fragmented and require synthesis. This scoping review aims to consolidate existing evidence on the relationship between economic crises and a broad range of mental health outcomes, including suicide, depression, anxiety, psychological distress, and health service utilization. Multiple databases (PubMed, EMBASE, Web of Science, Scopus, PsycINFO, EconLit) were explored for reports published between January 2000 and December 2025, following PRISMA-ScR guidelines. Totally, 122 studies met the inclusion criteria. Economic crises are consistently associated with adverse mental health outcomes. Key findings include increased suicide mortality, particularly among working-age men, with pronounced spikes during and after major crises such as the 2008 global financial crisis and the 1997 Asian financial crisis. Non-fatal suicidal behaviors (ideation, attempts, self-harm), depression, anxiety, and psychological distress also rise significantly, driven by unemployment, income loss, debt, and housing insecurity. Vulnerable groups, including the unemployed, low-income populations, youth, and those with pre-existing mental health conditions are disproportionately affected. The evidence also indicates mixed patterns in mental health service utilization, often constrained by austerity and access barriers. Social protection systems and supportive policies appear to mitigate negative mental health impacts. Economic crises exert a significant and multifaceted toll on population mental health, exacerbating inequalities and increasing the burden of mental disorders and suicidal behavior. The findings underscore the need for integrated policy responses that strengthen social safety nets, ensure accessible mental healthcare, and address the psychosocial and economic determinants of health during periods of financial instability. Research gaps remain, particularly in low- and middle-income countries and regarding long-term mental health trajectories post-crisis.
Keywords:
austerity
; economic recession
; public health
; psychiatric disorders
; psychological distress
; health policy
1. Introduction
Economic crises, defined as periods of substantial financial instability characterized by declining gross domestic product (GDP), rising unemployment, collapsing credit systems, and widespread fiscal austerity, are recurring phenomena with profound social and public health consequences (Karanikolos et al., 2013; Stuckler et al., 2009). While the immediate focus during such downturns is often on economic indicators, the ripple effects extend far beyond financial markets. Individuals, households, and communities experience elevated stress, reduced access to essential goods and services, and heightened vulnerability to disease. The relationship between macroeconomic instability and public health outcomes has been increasingly documented, with evidence showing that recessions and financial collapses can adversely affect mental health, exacerbate inequalities, and disrupt healthcare provision (Catalano et al., 2011; Reeves et al., 2013).
Economic crises are not a recent phenomenon. The 19th century witnessed numerous financial contractions, including the Long Depression (1873–1896) following the collapse of European banks and declining commodity prices, which led to mass unemployment and impoverishment in affected regions (Khramov and Lee, 2013; Morgan, 2013). The early 20th century saw the Great Depression (1929–1939), which profoundly altered global economic and social landscapes. Unemployment skyrocketed, banks failed, and widespread poverty contributed to malnutrition and the spread of infectious diseases in many countries (Langthorne and Bambra, 2020; Tapia Granados and Diez Roux, 2009). Following World War II, the global economic order stabilized somewhat, but crises continued to emerge, often triggered by speculative asset bubbles, mismanaged fiscal policies, or exogenous shocks such as oil price spikes (Berend, 2012; Hamilton, 2013).
More recent examples illustrate the globalized nature of economic vulnerability. The Asian financial crisis of 1997–1998 caused severe economic contraction in several East Asian countries, resulting in job losses, decreased household income, and a documented rise in communicable diseases such as tuberculosis (Arinaminpathy and Dye, 2010; Choi et al., 2019; Suhrcke et al., 2011).
The bursting of the dot-com bubble in 2000 and subsequent lending excesses culminated in the 2007–2008 global financial crisis, widely regarded as the most severe economic shock since the Great Depression. This crisis resulted in widespread corporate bankruptcies, massive job losses, a collapse in private sector lending, surging public debt, and a sharp drop in global trade (Falagas et al., 2009; Fountoulakis et al., 2013, 2012; Liaropoulos, 2012; Parmar et al., 2016; Suhrcke et al., 2011; Van Hal, 2015; Wade, 2009).
More recently, economic shocks driven by pandemics, migration, armed conflicts, and climate change have further strained public health systems, particularly in low- and middle-income countries (Clech et al., 2022; Foroughi et al., 2025; Goodell, 2020). Rising unemployment, currency devaluation, and inflation reduce household purchasing power and limit access to essential services, amplifying the negative health consequences of these crises.
Economic crises affect health through multiple direct and indirect pathways. One primary pathway is psychosocial stress, driven by unemployment, income insecurity, and uncertainty about the future. Elevated stress levels are strongly associated with depression, anxiety, substance use, and suicidal behavior (Frasquilho et al., 2015; Guerra and Eboreime, 2021; Gunnell et al., 2004; Haw et al., 2015). Evidence indicates that populations experiencing high unemployment rates during recessions show increased prevalence of mental health disorders, and suicide rates often rise in parallel, particularly among working-age men and young adults (Milner et al., 2014; Virgolino et al., 2022).
A second pathway is healthcare access and service provision. Fiscal austerity and declining public revenues often lead to cuts in health budgets, reduced availability of preventive and primary care, and increased out-of-pocket expenditures for patients (Broadbent et al., 2023; Stuckler et al., 2009). During the 2008 global financial crisis, several European countries implemented austerity policies that reduced funding for hospitals, mental health services, and public health programs, disproportionately affecting vulnerable populations (Kentikelenis and Papanicolas, 2012; Maresso et al., 2015; Van Gool and Pearson, 2014).
In low-income countries, reductions in donor support and local health budgets can impair vaccination campaigns, infectious disease surveillance, and treatment programs, leading to increased morbidity and mortality (Clech et al., 2022; Foroughi et al., 2025; Suhrcke et al., 2011).
Third, changes in health-related behaviors during economic crises can exacerbate health risks. Financial stress may drive individuals toward cheaper, nutrient-poor diets, increased tobacco or alcohol consumption, and reduced physical activity.
Behavioral shifts, combined with weakened health services, can lead to higher prevalence of chronic diseases, obesity, and non-communicable disease-related mortality (De Goeij et al., 2015; European Centre for Disease Prevention and Control. Stockholm: ECDC, 2013; Frasquilho et al., 2015; Suhrcke et al., 2011).
The socioeconomic gradient in health becomes particularly pronounced during economic downturns. Poorer populations are disproportionately affected due to limited resources, pre-existing health disparities, and lower resilience to shocks. Rural populations, marginalized urban communities, and informal workers often bear the brunt of adverse health outcomes during crises, including increased malnutrition, injury, infectious disease exposure, and preventable mortality (Heggebø et al., 2019; Maynou and Saez, 2016; Regidor et al., 2016).
Despite growing interest, evidence on the health impacts of economic crises remains fragmented. Many studies focus on specific countries, population subgroups, or outcomes, and few integrate infectious and non-communicable diseases, mental health, and healthcare system disruptions in a single analysis.
The World Health Organization (WHO) describes mental health as encompassing a wide range of activities that directly or indirectly relate to mental well-being, aligning with its overall definition of health as “a state of complete physical, mental, and social well-being, and not merely the absence of disease.” This approach is also in line with the perspective of the American Psychiatric Association (APA), which defines psychological disorders as patterns of symptoms or behaviors that impair an individual’s well-being and interfere with normal daily functioning (Llosa et al., 2018).
This scoping review aims to fill this gap by evaluating the impact of economic crises including recessions, financial collapses, and austerity measures on a wide spectrum of mental health outcomes. By integrating data across multiple countries, income levels, and health outcomes, this review aims to provide a holistic understanding of how economic instability shapes population mental health resilience. Recognizing these linkages is crucial for designing interventions that protect mental health in times of financial hardship and reduce inequities exacerbated by economic crises.
2. Methodology
2.1. Search Strategy
This study was conducted in accordance with the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews) checklist (Tricco et al., 2018) (Figure 1). A comprehensive search was conducted in electronic databases including PubMed, EMBASE, Web of Science, Scopus, Psychological Information Database (PsycINFO), and Economics Literature (EconLit). Additional searches were performed in WHO, the Organization for Economic Co-operation and Development (OECD), and relevant government health department websites as well as the reference lists of relevant studies, reviews, and meta-analyses. All studies published between January 2000 and December 2025, with no time restriction, were considered eligible.
The search terms were outlined as: “austerity”, “economic crisis”, “fiscal crisis”, “financial crisis”, “economic recession”, “economic depression”, “economic insecurity”, “economic recession”, “banking crisis”, “unemployment”, “personnel downsizing”, “job loss”, “mental health”, “mental disorder”, “mental illness”, “depression”, “anxiety”, “suicide”, “psychological distress”, “depressive disorder”, “mood disorder”, “psychiatric disorder”, “psychological wellbeing”, and “emotional distress” employing “OR” and/or “AND” Boolean operators.
2.2. Study Selection Process
Following the removal of duplicates, two reviewers independently screened all titles and abstracts against the predetermined eligibility criteria. Studies that clearly did not meet the inclusion criteria were excluded at this stage.
The full texts of potentially relevant articles were then obtained and independently assessed by the same two reviewers for eligibility. Any disagreements between reviewers were resolved through discussion, and when consensus could not be reached, a third reviewer was consulted for final decision-making.
2.3. Eligibility Criteria
2.3.1. Inclusion Criteria
1) Primary empirical studies of any design (quantitative, qualitative, or mixed-methods) examining the association between an economic crisis and mental health outcomes; 2) Studies focusing on either the general population or specific vulnerable groups (e.g., unemployed individuals, migrants, healthcare workers); 3) Studies that clearly define or describe exposure to an economic crisis event, published between January 2000 and December 2025; 4) Studies reporting mental health outcomes measured using validated instruments, including depression, anxiety, psychological distress, or composite mental health indicators; and 5) Peer-reviewed original research articles published in English.
2.3.2. Exclusion Criteria
1) Non-primary study designs, including case reports, case series, review articles (systematic, scoping, narrative), meta-analyses, letters, editorials, commentaries, conference abstracts without full text, and publications containing non-original or secondary data; 2) Studies reporting only health behaviors (e.g., smoking, alcohol consumption) without mental health outcomes, and studies using non validated mental health measures; and 3) Studies for which relevant data could not be extracted or where outcomes did not align with the review objectives.
2.4. Software and Data Analysis
All references were imported into Mendeley software for de-duplication. Data from the included studies were charted using Microsoft Excel following the Joanna Briggs Institute (JBI) guidelines for scoping reviews.
3. Results
3.1. Study Selection
The systematic search of electronic databases and relevant sources identified a total of 15,043 records. After removing 13,147 duplicate entries, 1,896 records remained for title and abstract screening. During this initial screening phase, 1,541 records were excluded as irrelevant to the review’s scope, leaving 355 records for full-text retrieval. Of these, 182 reports could not be retrieved, resulting in 173 articles assessed for eligibility through full-text review.
After detailed evaluation, 51 full-text articles were excluded for the following reasons: non-original or secondary data (n=9), improper outcome measures (n=10), overlapping datasets (n=13), lack of relevant data (n=15), and not published in English (n=4). Ultimately, 122 studies met all inclusion criteria and were included in the final scoping review.
3.2. Characteristics of the Included Studies
3.2.1. Study Designs
The methodological approaches of the 122 included studies were diverse, reflecting the multifaceted research on economic crises and mental health. The most common design was the ecological study (n=34, 27.9%), which analyzed population-level data to correlate economic indicators (e.g., unemployment rates) with mental health outcomes.
Longitudinal designs, including cohort and panel studies (n=32, 26.2%), constituted the next largest group, following individuals or groups over time. Repeated cross-sectional surveys (n=29, 23.8%) were also prevalent, capturing trends at multiple time points before, during, and after economic downturns. The remaining studies employed standard cross-sectional designs (n=18, 14.8%), case-control methods (n=2, 1.6%), interrupted time-series analyses (n=4, 3.3%), and other designs (n=3, 2.5%).
The research encompassed a wide geographical scope, with studies from Europe, North America, Asia, and Oceania, and spanned from 2001 to 2024, with a particular concentration around the 2008 global financial crisis (Table 1).
3.2.2. Geographic Distribution of the Studies
Of the 122 studies included in the review, the geographical distribution was predominantly centered on Europe, with 70 studies (57.4%) conducted in European nations. A significant portion of these focused on countries deeply impacted by the 2008 financial crisis and subsequent austerity measures, including Greece, Spain, the United Kingdom, and Italy. North America was the second most represented region, contributing 23 studies (18.9%).
Research from Asia, Australasia, and South America was less common, with a combined total of 17 studies (13.9%). This distribution reveals a notable geographical gap, as no studies from Africa were identified, and only two studies originated in South America. Additionally, nine studies (7.4%) utilized cross-continent or multi-country population samples, analyzing data from groupings such as the European Union or global datasets (Table 1).
3.2.3. Population/Participants
The populations studied were heterogeneous, encompassing: 1) General adult populations: The majority of studies (n=85) analyzed data from national or regional adult populations, often stratifying by sex and age; 2) Specific workforce groups: Several studies (n=18) focused on employed individuals, those experiencing job loss, temporary workers, or employees in specific industrial sectors (e.g., manufacturing plants); 3) Clinical/Patient populations: A subset of studies (n=12) examined individuals with mental health conditions, those attempting suicide, or patients utilizing mental health services (inpatient, outpatient, primary care); and 4) Vulnerable subgroups: Research specifically addressed low-income groups (n=9), unemployed individuals (n=22), older adults (n=3), and adolescents (n=7, often in the context of parental unemployment).
Analyses were frequently disaggregated by sex/gender (male vs. female), revealing often distinct patterns in mental health outcomes.
3.3. Key Topics and Exposures
3.3.1. Suicide Mortality
The literature consistently shows that economic crises increase suicide rates, particularly among working-age men. A global time-trend study of 54 countries found that male suicide rates rose by 3.3% after the 2008 crisis (rate ratio 1.033, 95% CI: 1.027–1.039) (Chang et al., 2013), with larger increases in Europe (+4.2%) and the Americas (+6.4%). In England, Barr et al. reported roughly 846 excess male suicides and 155 excess female suicides during 2008–2010, and found that each 10% rise in unemployment corresponded to a 1.4% increase in male suicide (no significant change for women) (Barr et al., 2012).
The impact of austerity was especially pronounced in Greece reported a 35.7% increase in total suicides in June 2011 coinciding with austerity measures (Branas et al., 2015), and another research found suicide risk was 1.34 times higher during 2011–12 compared to the pre-austerity era (Rachiotis et al., 2015). Similar patterns were observed during the 1997–98 Asian financial crisis: Chang et al. reported male suicide rates rose 39% in Japan, 44% in Hong Kong, and 45% in South Korea (Chang et al., 2009).
Evidence from previous review (Frasquilho et al., 2015) further confirms that suicide rises following recessions are observed globally across multiple crises, including the early 1990s European recessions, the 1997 Asian financial crisis, and the 2008 global financial crisis. These studies consistently show stronger effects in men, middle-aged adults, and populations with weaker social safety nets. Contextual factors, such as timing of the crisis, social protection policies, and pre-existing mental health trends, modify the magnitude of the effect. For instance, Swedish data indicate a delayed increase in suicide among unemployed men post-recession (HR 1.43, 95% CI: 1.31–1.56) (Ásgeirsdóttir et al., 2017), whereas in Iceland, male suicide attempts decreased after the 2008 banking collapse (IRR 0.85, 95% CI: 0.76–0.96) (Garcy and Vågerö, 2013).
3.3.2. Suicidal Ideation, Attempts, and Self-Harm
Economic hardship is strongly linked to nonfatal suicidal behaviors. In Spain, Córdoba-Doña et al. (2014) estimated ~2,017 excess male suicide attempts during 2008–2012 (Córdoba-Doña et al., 2014). Individual-level analyses reinforce this: Belgian adults who lost employment in the past year had nearly nine times higher odds of suicidal thoughts (OR≈8.8, 95% CI: 2.0–39.3) (Vanderoost et al., 2013), and in the US, each additional recession-related hardship (e.g., debt, unemployment, housing loss) increased the odds of a suicide attempt by 53% (OR 1.53, 95% CI: 1.32–1.77) (Elbogen et al., 2020).
Hospitalization data also reflect this trend. In a longitudinal analysis from multi-centre study of Self-harm in England, Hawton and colleagues reported an increase in self-harm presentations following the 2008 recession: rates declined in men until 2008 but then rose steadily up through 2012 (Clements et al., 2019). Their ecological and patient-level study linked increased self-harm rates to areas with greater rises in unemployment (Hawton et al., 2016).
A broader review by Frasquilho et al. (Frasquilho et al., 2015) concluded that evidence from Europe, North America, and Asia consistently shows that economic recessions and associated stressors such as unemployment, income loss, and debt are associated with poorer mental health and increased suicidal behaviours (including attempts and self-harm).
However, the pattern does not always hold. For instance, a population-based study from Iceland found that after the 2008 economic collapse, rates of hospital attendances for suicide attempts and self-harm actually decreased among both men and women: first attendances post-collapse had an incidence rate ratio (IRR) of 0.85 (95% CI: 0.76–0.96) in men, and 0.86 (95% CI: 0.79–0.92) in women (Ásgeirsdóttir et al., 2017).
3.3.3. Depression, Psychological Distress, and Poor Mental Health
Financial strain and unemployment are strongly associated with depression and psychological distress. In Spain, individuals reporting mortgage-payment difficulties or other financial hardship during the crisis even after adjusting for unemployment had roughly double the odds of major depression (OR ≈ 2.11–2.12, p < 0.001), and combinations of unemployment and mortgage difficulties accounted for a large share of increased depression risk among primary-care attenders (Gili et al., 2013).
In Italy, being a first-job seeker or unemployed was associated with significantly worse self-reported health compared with permanently employed peers, and job insecurity or unemployment correlated with poorer mental health especially among young and male workers (Minelli et al., 2014).
In the Great Recession context in the United States, individuals who experienced one or more hardship events related to the recession, including job loss, financial strain, or housing problems had elevated risks of depressive symptoms, anxiety or other mental-health problems years after the recession ended (Forbes and Krueger, 2019). In Canada, a population-based analysis showed that during the austerity period following the financial crisis, the odds of reporting “poor mental health” were 1.26 times higher (95% CI: 1.16–1.32) compared with pre-crisis periods (Nour et al., 2017).
Frasquilho et al. (2016) (Frasquilho et al., 2015) reviewed 101 studies and concluded that depression, anxiety, and psychological distress increased consistently during recessions, with unemployed, lower-income, and socially disadvantaged adults at greatest risk.
Gender differences were observed: men often experienced larger increases in psychological distress than women, likely reflecting male-dominated sectors and income losses.
3.3.4. Utilization of Mental Health Services and Medications
Economic crises appear to affect both mental-health needs and access to care. In the U.S., a previous study (Modrek et al., 2015), found that among employed, continuously insured workers there was an increase after 2009 in both outpatient and inpatient mental-health visits, and in the yearly supply of psychotropic medications. At the same time, a broader review of crises across countries (including the U.S.) observed mixed utilization patterns: while some studies showed increased general help-seeking or psychotropic drug use, others found no change or even declines in specialized mental health care use during and after recessions (Silva et al., 2020).
For example, one U.S. study referenced in the review reported that adults living in counties with higher unemployment rates had lower relative risk of using mental-health services compared to those in low-unemployment counties (ARR ≈ 0.58–0.71 depending on the threshold) (Dunlap et al., 2016).
Thus, while economic downturns may increase mental-health burden and demand for care, access remains unequal, especially for disadvantaged populations or in high-unemployment regions (Frasquilho et al., 2015).
3.3.5. Other Mental and Behavioral Outcomes
Economic downturns are also associated with adverse behavioral and broader health outcomes. For instance, evidence from Impact of the 2008 global financial crisis on the health of Canadians: repeated cross-sectional analysis of the Canadian Community Health Survey, 2007-2013 shows that during the austerity period following the 2008 crisis, the odds of reporting poor self-perceived mental health rose by about 26% (OR = 1.26, 95% CI: 1.16–1.32), compared to pre-crisis baseline. Also in Canada, that same study found increased odds for heavy alcohol drinking (OR = 1.09 in the austerity period vs pre-crisis), indicating that substance use may rise in response to economic stressors (Nour et al., 2017).
Still, the literature on alcohol use and economic crises is not uniform. A realist systematic review How economic crises affect alcohol consumption and alcohol-related health problems: a realist systematic review concluded that while psychological distress linked to unemployment and income reduction could increase harmful drinking, especially among men tighter budget constraints could reduce overall alcohol consumption. The net effect depends heavily on contextual factors (gender, social support, social norms, disposable income) (De Goeij et al., 2015).
Furthermore, long-term follow-up data from a recession in Finland (1990s) revealed significantly increased risk of psychiatric disorders and alcohol-related diseases among men who experienced recession-related hardships (HR ≈ 2.20 and HR ≈ 4.44, respectively) but not among women (Jarroch et al., 2022).
3.3.6. Moderating and Protective Factors
There is also evidence that social and policy context can mitigate the negative mental health effects of economic crises. The systematic review on mental-health outcomes in recessions notes that the overall impact varies considerably by country and is influenced by social protection systems, labor market policies, and welfare measures (Frasquilho et al., 2015). For example, some studies found that increased use of general practitioners (for mental health problems) rose in countries with growing unemployment, but use of specialized psychiatric care often did not increase suggesting that barriers to specialty care remain (Silva et al., 2020).
Likewise, in the U.S., although overall outpatient mental-health service use rose in the 2008–2015 period, much of the increase was driven by individuals with less serious or no psychological distress, rather than those with serious distress raising concerns about unmet need among the most vulnerable (Olfson et al., 2019).
Table 2 summarizes the key findings related to vulnerable population groups identified across the included studies.
4. Discussion
This scoping review finds strong evidence that economic crises are associated with worsening mental health at the population level. The literature consistently shows that recessions and financial shocks coincide with higher rates of common mental disorders and substance use. In particular, many studies report that rising unemployment, wage cuts, and income loss act as powerful stressors that precipitate depression, anxiety, and related disorders (Mucci et al., 2016; Silva et al., 2016). For example, work by Gili et al. (Gili et al., 2013) and colleagues shows an epidemic of new-onset depression emerging alongside spikes in joblessness and financial insecurity during the 2008 Great Recession.
Unemployment and financial strain emerged repeatedly as strong correlates of depression. Most reviewed studies found that higher unemployment rates and individual job loss significantly increased depressive symptoms or diagnoses (Paul and Moser, 2009; Sterud et al., 2025). For instance, cross-national analyses documented that nations experiencing large rises in unemployment after 2008 saw proportionally more adults reporting major depression (Reeves et al., 2014). A systematic review and meta-analysis published in 2022 pooled evidence on unemployment and depression. It found that unemployment, overall, was associated with OR ≈ 2.06 (95% CI: 1.85, 2.30) for depressive symptoms i.e. roughly double the odds compared to employed people. In the same review, the association with clinically diagnosed major depressive disorder (MDD) was also elevated: OR ≈ 1.88 (95% CI: 1.57, 2.25) (Amiri, 2022a).
Anxiety disorders and psychological distress often rise with economic stress, but the population-level patterns can be nuanced: several reviews and population studies report only modest increases and in some national surveys anxiety prevalence remained stable during recessions (Guerra and Eboreime, 2021). However, effects are concentrated in specific, vulnerable groups: people experiencing job loss, precarious employment, large debt burdens, or housing insecurity show substantially larger increases in anxiety symptoms (Forbes and Krueger, 2019). For example, studies using administrative and prescription data find increased use of anxiolytics and related psychotropic medications among workers and populations exposed to downturns (Ferry et al., 2025). Mechanistically, job insecurity, debt, and housing worries appear to act as chronic psychosocial stressors that translate into heightened anxiety for those most exposed (Kopasker et al., 2018).
Economic downturns often drive increases in unhealthy coping behaviors. A large meta-analysis found that unemployed adults have significantly higher odds of heavy alcohol use (OR ≈ 1.25) and smoking (OR ≈ 1.43) compared with their employed peers (Amiri, 2022b). Similarly, a comprehensive review of over 130 studies concluded that risky alcohol consumption, illicit and prescription drug use, smoking, and substance-use disorders are more common among the unemployed (Henkel, 2011). For example, a U.S. national-survey study covering 2002–2010 reported that unemployed individuals had higher rates of past-month tobacco and illicit-drug use, heavy drinking, and past-year alcohol or drug abuse/dependence associations that persisted even during periods of major economic distress (Compton et al., 2014). In other words, as financial strain grows, many individuals may turn to tobacco, alcohol, or other substances as forms of stress relief compounding the public-health burden.
Evidence from the review by Sinyor et al. (Sinyor et al., 2024) underlines the strong impact of economic downturns, financial hardship, and unemployment on mental health, especially regarding suicide risk. It indicated that economic crises are unequivocally associated with heightened suicide rates across nations, regardless of income level or development status, underlining that the detriments of economic stressors on mental health are truly universal.
The relationship between economic crises and suicide is well documented, although the effects are not uniform across populations or contexts. For example, a time-series analysis covering 54 countries estimated about 4,900–5,124 “excess” suicides in 2009 compared with expected trends with significant increases concentrated among men in Europe (≈ 4.2%) and the Americas (≈ 6.4%). In some hard-hit regions, working-age men (especially those aged 45–64 in American countries) saw the largest increases (Chang et al., 2013). These findings suggest that sudden economic shocks, especially steep rises in unemployment may increase suicide risk among acutely vulnerable individuals.
However, the picture is more complex than a uniform rise in self-harm: a scoping review of subsequent research found that while most studies documented increased suicide mortality following recessions, several found little or no change in suicide attempts or self-harm hospitalizations in the post-recession period (Guerra and Eboreime, 2021). This heterogeneity likely reflects the moderating influence of social supports: for example, in a study from Japan, increased local government spending during economic downturns was associated with reduced suicide rates among middle-aged adults (Matsubayashi et al., 2020). Moreover, economic stressors beyond unemployment such as housing insecurity also matter. One analysis found a significant positive association between state-level foreclosure rates and suicide among middle-aged adults (46–64 years) in the U.S., suggesting that home loss may compound financial and emotional stress in a way that can be fatal (Houle and Light, 2014).
Economic crises affect people of all ages, but empirical evidence is particularly limited for the very young and the elderly. Several studies show that children and adolescents whose families experience job loss, income reductions, or broader economic hardship report higher rates of depression, anxiety, self-harm, and suicidal thoughts (Feghali et al., 2025). Parental unemployment or declining household income, along with increased family stress or conflict during recessions, have been identified as key mediating factors (Golberstein et al., 2019). For older adults, the picture is more mixed. On one hand, a longitudinal analysis from the Great Recession (2007–2009) found that decreases in financial resources corresponded with increased “financial strain,” which in turn was strongly associated with worsening anxiety and depressive symptoms (Wilkinson, 2016). On the other hand, some older people may be buffered by fixed incomes or pensions though declines in wealth and job loss during recessions remain linked to adverse mental health and even elevated mortality risk among older workers who lost jobs (Cutler and Sportiche, 2022). Overall, existing research suggests that economic downturns tend to amplify social inequalities: individuals and households already disadvantaged, including low-income families, precarious workers, youth, and older adults with financial vulnerability suffer disproportionately (Frasquilho et al., 2015).
These observed outcome patterns point to several interrelated mechanisms. First, psychosocial stress constitutes a central pathway: conditions such as unemployment, debt, housing loss, and job insecurity tend to increase chronic stress and undermine mental well-being. Evidence for this comes from studies in which individuals reporting insecure employment or debt had significantly higher odds of depressive disorder (Meltzer et al., 2010). Psychological models and surveys consistently find that fear of job loss and the inability to meet basic needs precipitate feelings of hopelessness and despair. Second, behavioral pathways may amplify risk: economic hardship often leads to poorer nutrition, social isolation, increased substance use, and reduced physical activity all factors known to worsen mood and health (Frasquilho et al., 2015). Third, disruptions in healthcare and social systems play a role.
Many governments adopt austerity during recessions, cutting funding for mental-health and social services. In countries facing strict fiscal consolidation, reductions in preventive and community-based mental health services have been associated with increases in suicide and psychiatric admissions (Quaglio et al., 2013). Reduced access to counselling, medications, and community supports thus leaves vulnerable individuals with far fewer resources just when they need them most. Finally, the broader economic and social context significantly shapes outcomes. Research indicates that in nations with weaker social safety nets and lower pre-crisis employment protections, the impact of financial downturns on suicide rates and mental disorders tends to be more severe (Uutela, 2010).
Our findings are in line with prior literature. Several systematic reviews (Frasquilho et al., 2015; Gili et al., 2013) similarly conclude that economic downturns worsen population mental health. These reviews highlight consistent associations between financial stressors and depression/anxiety, as well as elevated substance use during high unemployment. We found that suicide trends during crises can differ by gender, age and country, and that the overall picture depends on intervention context. Importantly, we also note gaps echoing previous calls: much of the evidence comes from Western Europe and North America, with relatively few high-quality studies from low- and middle-income countries or outside the Organisation for Economic Co-operation and Development (OECD). Likewise, there is scant research on post-traumatic stress or on long-term recovery of mental health after a crisis subsides.
Recognizing these patterns is critical for policymakers. The strong links between economic shocks and mental illness underscore the need for robust social safety nets and accessible mental healthcare, especially during downturns. For example, unemployment benefits, housing protections, debt relief and job retraining can reduce the psychological stress of a recession. Community and clinical programs should screen for depression, anxiety and substance use during economic crises to catch problems early. At the population level, protecting health budgets and ensuring continuity of mental health services (rather than cutting them) may mitigate the typical recession-induced spike in disorders. Our review also suggests that enhancing resilience factors – such as social support, education and positive coping – can buffer individuals. Indeed, studies show that life satisfaction, optimism and close social ties consistently protect against depression even in bad economies. Thus, interventions that strengthen community bonds and provide economic stability (e.g. cash transfers, progressive taxation, living wage policies) could have important mental health benefits during financial crises.
5. Limitations
This scoping review has limitations common to the field. Most cited studies are observational and ecological, making causal inference difficult. Data are also highly heterogeneous: crisis severity, duration, and policy responses differ widely across studies, which limits generalizability. Publication bias may exist toward countries with stronger research capacity. Notably, important areas remain under-explored: for example, some types of mental disorders, long-term outcomes beyond the immediate recession, and the effects of combined crises (such as economic collapse plus pandemic) are seldom studied.
6. Conclusions
This scoping review synthesizes an extensive body of evidence that establishes a large and multi-dimensional impact of economic crises on population mental health. The findings consistently point out that financial crises marked by recession, austerity measures, and increased unemployment result in deteriorated mental health at an individual and population level. Indeed, the evidence is strongest for increases in suicide mortality, particularly among working-age men, with pronounced effects observed during major crises such as the 2008 global financial crisis and the 1997 Asian financial crisis. Clear increases have also been linked to economic stressors in respect of other non-fatal suicidal behaviors-ideation, attempts, and self-harm-and the prevalence of common mental disorders, especially major depression, anxiety, and psychological distress. Economic downturns are associated with adverse health-related behaviors, including increased risky alcohol use and smoking, often as maladaptive coping mechanisms. The pathways through which economic shock is linked to poor mental health are interrelated. Psychosocial stress from financial hardship and uncertainty acts as a primary mechanism, while behavioral changes-substance use and social withdrawal-and systemic disruption-particularly austerity-driven cuts to mental health services and social safety nets-increase vulnerability. The impact is not uniform; it is powerfully influenced by socioeconomic and demographic factors. It tends to widen the gap within inequalities, with the greatest burdens on the most vulnerable groups of people: the unemployed, poor, young from affected families, and those with previous vulnerabilities.
Importantly, the review also illustrates that such effects can be moderated by protective factors and policy contexts. In particular, countries with stronger social protection systems, maintained access to healthcare, community support, and proactive economic policies-including unemployment benefits and housing support-have witnessed less severe deterioration in mental health during crises. However, critical evidence gaps remain. There is a striking geographic bias of the literature toward high-income countries in Europe and North America, with almost no contribution from the low- and middle-income regions and Africa. Further, there is a necessity for longitudinal studies considering long-term trajectories of mental health post-crisis and those on under-researched outcomes such as trauma-related disorders.
Funding
This work received no financial support from any organization.
Ethics Statement
This study is based solely on literature reviews and reports. It did not involve human participants or animals; therefore, ethical approval was not required.
Data Availability Statement
All data used in this study are available from the corresponding author upon request.
Acknowledgments
We would like to express our appreciation to the Editor-in-Chief, Editors, and reviewers for their valuable feedback and insightful suggestions for improving this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Amiri, S. Unemployment associated with major depression disorder and depressive symptoms: a systematic review and meta-analysis. Int. J. Occup. Saf. Ergon. 2022a, 28, 2080–2092. [Google Scholar] [CrossRef] [PubMed]
- Amiri, S. Smoking and alcohol use in unemployed populations: A systematic review and meta-analysis. J. Addict. Dis. 2022b, 40, 254–277. [Google Scholar] [CrossRef] [PubMed]
- Arinaminpathy, N.; Dye, C. Health in financial crises: economic recession and tuberculosis in Central and Eastern Europe. J. R. Soc. Interface 2010, 7, 1559–1569. [Google Scholar] [CrossRef]
- Ásgeirsdóttir, H.G.; Ásgeirsdóttir, T.L.; Nyberg, U.; Thorsteinsdottir, T.K.; Mogensen, B.; Matthiasson, P.; Lund, S.H.; Valdimarsdottir, U.A.; Hauksdóttir, A. Suicide attempts and self-harm during a dramatic national economic transition: a population-based study in Iceland. Eur. J. Public Health 2017, 27, 339–345. [Google Scholar] [CrossRef]
- Barr, B.; Taylor-Robinson, D.; Scott-Samuel, A.; McKee, M.; Stuckler, D. Suicides associated with the 2008-10 economic recession in England: time trend analysis. Bmj 2012, 345, e5142. [Google Scholar] [CrossRef]
- Berend, I.T. A restructured economy: From the oil crisis to the financial crisis, 1973--2009. 2012.
- Branas, C.C.; Kastanaki, A.E.; Michalodimitrakis, M.; Tzougas, J.; Kranioti, E.F.; Theodorakis, P.N.; Carr, B.G.; Wiebe, D.J. The impact of economic austerity and prosperity events on suicide in Greece: a 30-year interrupted time-series analysis. BMJ Open 2015, 5, e005619. [Google Scholar] [CrossRef]
- Broadbent, P.; Thomson, R.; Kopasker, D.; McCartney, G.; Meier, P.; Richiardi, M.; McKee, M.; Katikireddi, S.V. The public health implications of the cost-of-living crisis: outlining mechanisms and modelling consequences. Lancet Reg. Heal. 2023, 27. [Google Scholar] [CrossRef]
- Catalano, R.; Goldman-Mellor, S.; Saxton, K.; Margerison-Zilko, C.; Subbaraman, M.; LeWinn, K.; Anderson, E. The health effects of economic decline. Annu. Rev. Public Health 2011, 32, 431–450. [Google Scholar] [CrossRef]
- Chang, S.-S.; Gunnell, D.; Sterne, J.A.C.; Lu, T.-H.; Cheng, A.T.A. Was the economic crisis 1997--1998 responsible for rising suicide rates in East/Southeast Asia? A time--trend analysis for Japan, Hong Kong, South Korea, Taiwan, Singapore and Thailand. Soc. Sci. Med. 2009, 68, 1322–1331. [Google Scholar] [CrossRef]
- Chang, S.-S.; Stuckler, D.; Yip, P.; Gunnell, D. Impact of 2008 global economic crisis on suicide: time trend study in 54 countries. Bmj 2013, 347. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Chung, H.; Muntaner, C. Social selection in historical time: The case of tuberculosis in South Korea after the East Asian financial crisis. PLoS One 2019, 14, e0217055. [Google Scholar] [CrossRef] [PubMed]
- Clech, L.; Meister, S.; Belloiseau, M.; Benmarhnia, T.; Bonnet, E.; Casseus, A.; Cloos, P.; Dagenais, C.; De Allegri, M.; Du Loû, A.D.; et al. Healthcare system resilience in Bangladesh and Haiti in times of global changes (climate-related events, migration and Covid-19): an interdisciplinary mixed method research protocol. BMC Health Serv. Res. 2022, 22, 340. [Google Scholar] [CrossRef]
- Clements, C.; Hawton, K.; Geulayov, G.; Waters, K.; Ness, J.; Rehman, M.; Townsend, E.; Appleby, L.; Kapur, N. Self-harm in midlife: analysis using data from the Multicentre Study of Self-harm in England. Br. J. Psychiatry 2019, 215, 600–607. [Google Scholar] [CrossRef]
- Compton, W.M.; Gfroerer, J.; Conway, K.P.; Finger, M.S. Unemployment and substance outcomes in the United States 2002--2010. Drug Alcohol Depend. 2014, 142, 350–353. [Google Scholar] [CrossRef]
- Córdoba-Doña, J.A.; San Sebastián, M.; Escolar-Pujolar, A.; Mart\’\inez-Faure, J.E.; Gustafsson, P.E. Economic crisis and suicidal behaviour: the role of unemployment, sex and age in Andalusia, southern Spain. Int. J. Equity Health 2014, 13, 55. [Google Scholar] [CrossRef]
- Cutler, D.M.; Sportiche, N. Economic crises and mental health: Effects of the great recession on older Americans. 2022.
- De Goeij, M.C.M.; Suhrcke, M.; Toffolutti, V.; van de Mheen, D.; Schoenmakers, T.M.; Kunst, A.E. How economic crises affect alcohol consumption and alcohol-related health problems: a realist systematic review. Soc. Sci. Med. 2015, 131, 131–146. [Google Scholar] [CrossRef]
- Dunlap, L.J.; Han, B.; Dowd, W.N.; Cowell, A.J.; Forman-Hoffman, V.L.; Davies, M.C.; Colpe, L.J. Behavioral health outcomes among adults: associations with individual and community-level economic conditions. Psychiatr. Serv. 2016, 67, 71–77. [Google Scholar] [CrossRef]
- Elbogen, E.B.; Lanier, M.; Montgomery, A.E.; Strickland, S.; Wagner, H.R.; Tsai, J. Financial strain and suicide attempts in a nationally representative sample of US adults. Am. J. Epidemiol. 2020, 189, 1266–1274. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Health inequalities, the financial crisis, and infectious disease in Europe; ECDC: Stockholm, 2013. [Google Scholar]
- Falagas, M.E.; Vouloumanou, E.K.; Mavros, M.N.; Karageorgopoulos, D.E. Economic crises and mortality: a review of the literature. Int. J. Clin. Pract. 2009, 63, 1128–1135. [Google Scholar] [CrossRef] [PubMed]
- Feghali, R.; El-Hachem, C.; Bakhos, G.; Zarzour, M.; Khalil, R.B. The impact of economic crisis on the mental health of children and adolescents: a systematic review. Asian J. Psychiatr. 2025, 104613. [Google Scholar] [CrossRef] [PubMed]
- Ferry, F.; Kent, L.; Rosato, M.; Curran, E.; Leavey, G. Trends in psychotropic medication across occupation types before and during the Covid-19 pandemic: a linked administrative data study. Soc. Psychiatry Psychiatr. Epidemiol. 2025, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Forbes, M.K.; Krueger, R.F. The great recession and mental health in the United States. Clin. Psychol. Sci. 2019, 7, 900–913. [Google Scholar] [CrossRef]
- Foroughi, Z.; Ebrahimi, P.; Yazdani, S.; Aryankhesal, A.; Heydari, M.; Maleki, M. Analysis for health system resilience against the economic crisis: a best-fit framework synthesis. Heal. Res. Policy Syst. 2025, 23, 1–44. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Grammatikopoulos, I.A.; Koupidis, S.A.; Siamouli, M.; Theodorakis, P.N. Health and the financial crisis in Greece. Lancet 2012, 379, 1001–1002. [Google Scholar] [CrossRef]
- Fountoulakis, K.N.; Siamouli, M.; Grammatikopoulos, I.A.; Koupidis, S.A.; Siapera, M.; Theodorakis, P.N. Economic crisis-related increased suicidality in Greece and Italy: a premature overinterpretation. J Epidemiol Community Heal. 2013, 67, 379–380. [Google Scholar] [CrossRef]
- Frasquilho, D.; Matos, M.G.; Salonna, F.; Guerreiro, D.; Storti, C.C.; Gaspar, T.; Caldas-de-Almeida, J.M. Mental health outcomes in times of economic recession: a systematic literature review. BMC Public Health 2015, 16, 115. [Google Scholar] [CrossRef]
- Garcy, A.M.; Vågerö, D. Unemployment and suicide during and after a deep recession: a longitudinal study of 3.4 million Swedish men and women. Am. J. Public Health 2013, 103, 1031–1038. [Google Scholar] [CrossRef]
- Gili, M.; Roca, M.; Basu, S.; McKee, M.; Stuckler, D. The mental health risks of economic crisis in Spain: evidence from primary care centres, 2006 and 2010. Eur. J. Public Health 2013, 23, 103–108. [Google Scholar] [CrossRef]
- Golberstein, E.; Gonzales, G.; Meara, E. How do economic downturns affect the mental health of children? Evidence from the National Health Interview Survey. Health Econ. 2019, 28, 955–970. [Google Scholar] [CrossRef] [PubMed]
- Goodell, J.W. COVID-19 and finance: Agendas for future research. Financ. Res. Lett. 2020, 35, 101512. [Google Scholar] [CrossRef] [PubMed]
- Guerra, O.; Eboreime, E. The impact of economic recessions on depression, anxiety, and trauma-related disorders and illness outcomes—a scoping review. Behav. Sci. (Basel) 2021, 11, 119. [Google Scholar] [CrossRef]
- Gunnell, D.; Harbord, R.; Singleton, N.; Jenkins, R.; Lewis, G. Factors influencing the development and amelioration of suicidal thoughts in the general population: Cohort study. Br. J. Psychiatry 2004, 185, 385–393. [Google Scholar] [CrossRef]
- Hamilton, J.D. Historical oil shocks. In Routledge Handbook of Major Events in Economic History; Routledge, 2013; pp. 239–265. [Google Scholar]
- Haw, C.; Hawton, K.; Gunnell, D.; Platt, S. Economic recession and suicidal behaviour: Possible mechanisms and ameliorating factors. Int. J. Soc. Psychiatry 2015, 61, 73–81. [Google Scholar] [CrossRef]
- Hawton, K.; Bergen, H.; Geulayov, G.; Waters, K.; Ness, J.; Cooper, J.; Kapur, N. Impact of the recent recession on self-harm: longitudinal ecological and patient-level investigation from the Multicentre Study of Self-harm in England. J. Affect. Disord. 2016, 191, 132–138. [Google Scholar] [CrossRef]
- Heggebø, K.; Tøge, A.G.; Dahl, E.; Berg, J.E. Socioeconomic inequalities in health during the great recession: a scoping review of the research literature. Scand. J. Public Health 2019, 47, 635–654. [Google Scholar] [CrossRef] [PubMed]
- Henkel, D. Unemployment and substance use: a review of the literature (1990-2010). Curr. Drug Abuse Rev. 2011, 4, 4–27. [Google Scholar] [CrossRef]
- Houle, J.N.; Light, M.T. The home foreclosure crisis and rising suicide rates, 2005 to 2010. Am. J. Public Health 2014, 104, 1073–1079. [Google Scholar] [CrossRef] [PubMed]
- Jarroch, R.; Tajik, B.; Tuomainen, T.-P.; Kauhanen, J. Economic Recession and the Long Term Risk of Psychiatric Disorders and Alcohol Related Diseases—A Cohort Study From Eastern Finland. Front. psychiatry 2022, 13, 794888. [Google Scholar] [CrossRef]
- Karanikolos, M.; Mladovsky, P.; Cylus, J.; Thomson, S.; Basu, S.; Stuckler, D.; Mackenbach, J.P.; McKee, M. Financial crisis, austerity, and health in Europe. Lancet 2013, 381, 1323–1331. [Google Scholar] [CrossRef] [PubMed]
- Kentikelenis, A.; Papanicolas, I. Economic crisis, austerity and the Greek public health system. Eur. J. Public Health 2012, 22, 4–5. [Google Scholar] [CrossRef]
- Khramov, M.V.; Lee, M.J.R. The Economic Performance Index (EPI): an intuitive indicator for assessing a country’s economic performance dynamics in an historical perspective. International Monetary Fund 2013. [Google Scholar] [CrossRef]
- Kopasker, D.; Montagna, C.; Bender, K.A. Economic insecurity: A socioeconomic determinant of mental health. SSM-population Heal. 2018, 6, 184–194. [Google Scholar] [CrossRef] [PubMed]
- Langthorne, M.; Bambra, C. Health inequalities in the Great Depression: a case study of Stockton on Tees, North-East England in the 1930s. J. Public Health (Bangkok) 2020, 42, e126–e133. [Google Scholar] [CrossRef]
- Liaropoulos, L. Greek economic crisis: not a tragedy for health. Bmj 2012, 345. [Google Scholar] [CrossRef]
- Llosa, J.A.; Menéndez-Espina, S.; Agulló-Tomás, E.; Rodr\’\iguez-Suárez, J. Job insecurity and mental health: A meta-analytical review of the consequences of precarious work in clinical disorders. 2018.
- Maresso, A.; Mladovsky, P.; Thomson, S.; Sagan, A.; Karanikolos, M.; Richardson, E.; Cylus, J.; Evetovits, T.; Jowett, M.; Figueras, J.; et al. Economic crisis, health systems and health in Europe; Copenhagen WHO, 2015. [Google Scholar]
- Matsubayashi, T.; Sekijima, K.; Ueda, M. Government spending, recession, and suicide: evidence from Japan. BMC Public Health 2020, 20, 243. [Google Scholar] [CrossRef] [PubMed]
- Maynou, L.; Saez, M. Economic crisis and health inequalities: evidence from the European Union. Int. J. Equity Health 2016, 15, 135. [Google Scholar] [CrossRef]
- Meltzer, H.; Bebbington, P.; Brugha, T.; Jenkins, R.; McManus, S.; Stansfeld, S. Job insecurity, socio-economic circumstances and depression. Psychol. Med. 2010, 40, 1401–1407. [Google Scholar] [CrossRef]
- Milner, A.; Page, A.; LaMontagne, A.D. Cause and effect in studies on unemployment, mental health and suicide: a meta-analytic and conceptual review. Psychol. Med. 2014, 44, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Minelli, L.; Pigini, C.; Chiavarini, M.; Bartolucci, F. Employment status and perceived health condition: longitudinal data from Italy. BMC Public Health 2014, 14, 946. [Google Scholar] [CrossRef]
- Modrek, S.; Hamad, R.; Cullen, M.R. Psychological well-being during the great recession: changes in mental health care utilization in an occupational cohort. Am. J. Public Health 2015, 105, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Morgan, E.V. The Great Depression, 1873-96. In The Theory and Practice of Central Banking, 1797–1913; Cambridge University Press, 2013; pp. 187–208. [Google Scholar]
- Mucci, N.; Giorgi, G.; Roncaioli, M.; Fiz Perez, J.; Arcangeli, G. The correlation between stress and economic crisis: a systematic review. Neuropsychiatr. Dis. Treat. 2016, 983–993. [Google Scholar] [CrossRef] [PubMed]
- Nour, S.; Labonté, R.; Bancej, C. Impact of the 2008 global financial crisis on the health of Canadians: repeated cross-sectional analysis of the Canadian Community Health Survey, 2007--2013. J Epidemiol Community Heal. 2017, 71, 336–343. [Google Scholar] [CrossRef] [PubMed]
- Olfson, M.; Wang, S.; Wall, M.; Marcus, S.C.; Blanco, C. Trends in serious psychological distress and outpatient mental health care of US adults. JAMA psychiatry 2019, 76, 152–161. [Google Scholar] [CrossRef]
- Parmar, D.; Stavropoulou, C.; Ioannidis, J.P.A. Health outcomes during the 2008 financial crisis in Europe: systematic literature review. Bmj 2016, 354. [Google Scholar] [CrossRef]
- Paul, K.I.; Moser, K. Unemployment impairs mental health: Meta-analyses. J. Vocat. Behav. 2009, 74, 264–282. [Google Scholar] [CrossRef]
- Quaglio, G.; Karapiperis, T.; Van Woensel, L.; Arnold, E.; McDaid, D. Austerity and health in Europe. Health Policy (New York) 2013, 113, 13–19. [Google Scholar] [CrossRef]
- Rachiotis, G.; Stuckler, D.; McKee, M.; Hadjichristodoulou, C. What has happened to suicides during the Greek economic crisis? Findings from an ecological study of suicides and their determinants (2003--2012). BMJ Open 2015, 5, e007295. [Google Scholar] [CrossRef]
- Reeves, A.; Basu, S.; McKee, M.; Marmot, M.; Stuckler, D. Austere or not? UK coalition government budgets and health inequalities. J. R. Soc. Med. 2013, 106, 432–436. [Google Scholar] [CrossRef] [PubMed]
- Reeves, A.; McKee, M.; Stuckler, D. Economic suicides in the great recession in Europe and North America. Br. J. Psychiatry 2014, 205, 246–247. [Google Scholar] [CrossRef]
- Regidor, E.; Vallejo, F.; Granados, J.A.T.; Viciana-Fernández, F.J.; de la Fuente, L.; Barrio, G. Mortality decrease according to socioeconomic groups during the economic crisis in Spain: a cohort study of 36 million people. Lancet 2016, 388, 2642–2652. [Google Scholar] [CrossRef]
- Silva, M.; Loureiro, A.; Cardoso, G. Social determinants of mental health: a review of the evidence. Eur. J. Psychiatry 2016, 30, 259–292. [Google Scholar]
- Silva, M.; Resurrección, D.M.; Antunes, A.; Frasquilho, D.; Cardoso, G. Impact of economic crises on mental health care: a systematic review. Epidemiol. Psychiatr. Sci. 2020, 29, e7. [Google Scholar] [CrossRef]
- Sinyor, M.; Silverman, M.; Pirkis, J.; Hawton, K. The effect of economic downturn, financial hardship, unemployment, and relevant government responses on suicide. Lancet Public Heal. 2024, 9, e802–e806. [Google Scholar] [CrossRef]
- Sterud, T.; Lunde, L.-K.; Berg, R.; Proper, K.I.; Aanesen, F. Mental health effects of unemployment and re-employment: a systematic review and meta-analysis of longitudinal studies. Occup. Environ. Med. 2025, 82, 343–353. [Google Scholar] [CrossRef]
- Stuckler, D.; Basu, S.; Suhrcke, M.; Coutts, A.; McKee, M. The public health effect of economic crises and alternative policy responses in Europe: an empirical analysis. Lancet 2009, 374, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Suhrcke, M.; Stuckler, D.; Suk, J.E.; Desai, M.; Senek, M.; McKee, M.; Tsolova, S.; Basu, S.; Abubakar, I.; Hunter, P.; et al. The impact of economic crises on communicable disease transmission and control: a systematic review of the evidence. PLoS One 2011, 6, e20724. [Google Scholar] [CrossRef] [PubMed]
- Tapia Granados, J.A.; Diez Roux, A.V. Life and death during the Great Depression. Proc. Natl. Acad. Sci. 2009, 106, 17290–17295. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Uutela, A. Economic crisis and mental health. Curr. Opin. Psychiatry 2010, 23, 127–130. [Google Scholar] [CrossRef]
- Van Gool, K.; Pearson, M. Health, austerity and economic crisis: Assessing the short-term impact in OECD countries. 2014.
- Van Hal, G. The true cost of the economic crisis on psychological well-being: a review. Psychol. Res. Behav. Manag. 2015, 17–25. [Google Scholar] [CrossRef]
- Vanderoost, F.; van der Wielen, S.; van Nunen, K.; Van Hal, G. Employment loss during economic crisis and suicidal thoughts in Belgium: a survey in general practice. Br. J. Gen. Pract. 2013, 63, e691. [Google Scholar] [CrossRef]
- Virgolino, A.; Costa, J.; Santos, O.; Pereira, M.E.; Antunes, R.; Ambrosio, S.; Heitor, M.J.; Vaz Carneiro, A. Lost in transition: a systematic review of the association between unemployment and mental health. J. Ment. Heal. 2022, 31, 432–444. [Google Scholar] [CrossRef] [PubMed]
- Wade, R. Essays on global financial crisis: The crisis as opportunity. Cambridge J. Econ. 2009. [Google Scholar]
- Wilkinson, L.R. Financial strain and mental health among older adults during the great recession. Journals Gerontol. Ser. B Psychol. Sci. Soc. Sci. 2016, 71, 745–754. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
PRISMA flow diagram of the study design process.
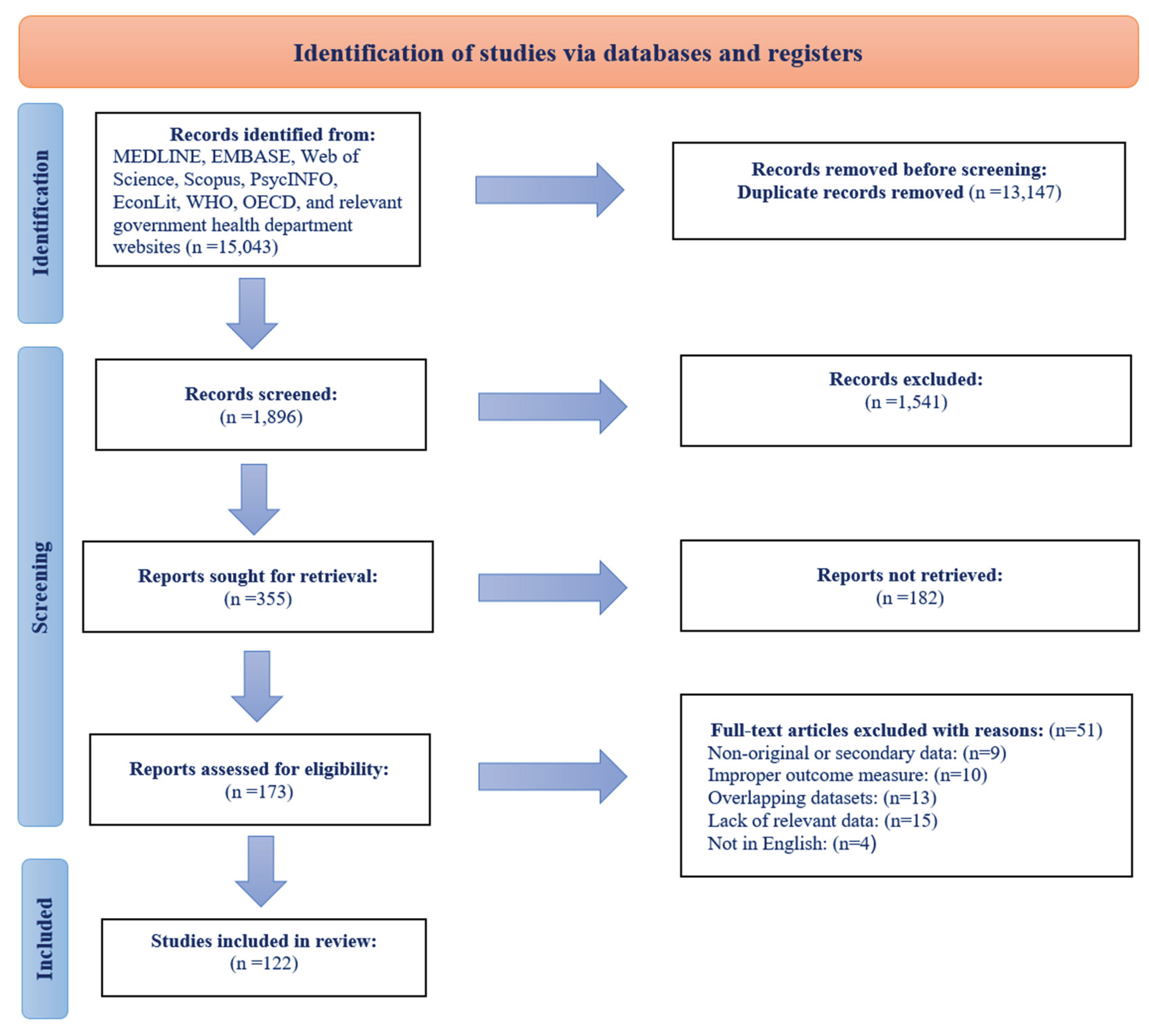

Table 1.
Characteristics of the included studies.
| No | Study | Country/Region | Study Design | Mental Disorder Type | Key Findings/Associations |
|---|---|---|---|---|---|
| 1 | Ostamo & Lönnqvist (2001) | Finland | Repeated cross-sectional | Suicide | Male attempted suicide rates decreased significantly during severe recession |
| 2 | Solantaus et al. (2004) | Finland | Cohort | Child Mental Health | Family economic stress creates risk for child mental health through family processes |
| 3 | Munne (2005) | Argentina | Cross-sectional | Substance Use | Economic crisis led to drinking more at home, shifting to cheaper alcohol |
| 4 | Lindstrom (2005) | Sweden | Cross-sectional | Psychological Distress | Unemployed: OR=5.81 (6.43-7.79) for psychological distress |
| 5 | Savarovalci et al. (2005) | Brazil | Cross-sectional | Depression/Anxiety | Strong association between unemployment and depression/anxiety in men |
| 6 | Reinhardt Pedersen et al. (2005) | Denmark/Sweden | Cross-sectional | Child Psychosomatic | Children with unemployed parents: OR=1.52-3.20 for psychosomatic symptoms |
| 7 | Sleskova et al. (2006) | Slovakia | Cross-sectional | Adolescent Health | Parental unemployment negatively associated with adolescent health |
| 8 | Newman & Bland (2007) | Canada | Case-control | Suicide | Association between unemployment and parasuicide: OR=12.0 (6.0-23.9) |
| 9 | Thomas et al. (2007) | UK | Cohort | Psychological Distress | Job loss increased risk of distress: OR men=3.15 (2.50-3.98) |
| 10 | Taylor et al. (2007) | UK | Cohort | Psychological Distress | Housing payment problems and debts have detrimental effects on mental wellbeing |
| 11 | Meltzer et al. (2007) | UK | Cross-sectional | Suicide | Those in debt twice as likely to think about suicide |
| 12 | Kondo et al. (2008) | Japan | Repeated cross-sectional | Self-Rated Health | OR for poor self-rated health increased from 1.02 to 1.14 after crisis |
| 13 | Charles & Decicca (2008) | USA | Repeated cross-sectional | Psychological Distress | 1% unemployment → 3.4% point increase in sadness |
| 14 | Stuckler et al. (2009) | 26 EU countries | Ecological | Suicide | 1% unemployment increase → 0.79% increase in suicide <65 years |
| 15 | Carter et al. (2009) | New Zealand | Cohort | Psychological Distress | Lowest wealth quintile: RR=3.06 (2.63-3.50) for psychological distress |
| 16 | Molarius et al. (2009) | Sweden | Cross-sectional | Depression/Anxiety | Unemployment (OR=2.9) and financial strain strongly related to anxiety/depression |
| 17 | Chang et al. (2009) | Japan; Hong Kong; South Korea | Time-trend analysis (Japan; Hong Kong; South Korea) | Suicide | Suicide rate in men: RR=1.387 (1.358-1.417) after Asian crisis | Suicide rate in men: RR=1.443 (1.263-1.649) | Suicide rate in men: RR=1.446 (1.387-1.507) |
| 18 | Wang et al. (2010) | Canada | Cross-sectional | Depression | 12-month MDD prevalence increased from 5.1% to 7.6% post-crisis |
| 19 | Lee et al. (2010) | Hong Kong | Repeated cross-sectional | Depression | MDE prevalence increased from 8.5% (2007) to 17.25% (2009) |
| 20 | Ford et al. (2010) | England | Cross-sectional | Common Mental Disorders | Risk of common mental disorders greater in unemployed individuals |
| 21 | Meltzer et al. (2010) | UK | Cross-sectional | Depression | Job insecurity (OR=1.58) and debt (OR=2.17) associated with depression |
| 22 | Borges et al. (2010) | 21 countries | Cross-sectional | Suicide | Unemployment strong risk factor for suicidal ideation and attempts |
| 23 | Stuckler et al. (2011) | Multiple EU countries | Ecological time-series | Suicide | Suicide increased ~7% in old EU countries after 2008 recession |
| 24 | Madianos et al. (2011) | Greece | Repeated cross-sectional | Depression | Major depression prevalence: 6.8% (2008) vs 3.3% (2009) |
| 25 | Davalos & French (2011) | USA | Cohort | General Mental Health | State unemployment worsens individuals’ mental HRQoL |
| 26 | Strandh et al. (2011) | Sweden | Cohort | Psychological Distress | Negative effects of unemployment rate on mental health of unemployed |
| 27 | Economou et al. (2011) | Greece | Repeated cross-sectional | Suicide | High economic distress associated with suicide attempts (p<0.001) |
| 28 | Hong et al. (2011) | South Korea | Repeated cross-sectional | Suicide | Income gradient-related suicide behavior increased post-recession |
| 29 | Karjalainen et al. (2011) | Finland | Case-control | Substance Use | Unemployment strong predictor of driving under influence of drugs |
| 30 | Jefferis et al. (2011) | EU countries /Chile | Cohort | Depression | Job loss → RR=1.58 (0.76-3.27) for depression |
| 31 | Freyer-Adam et al. (2011) | Germany | Cross-sectional | Substance Use | 84.8% of long-term unemployed young men were smokers |
| 32 | Sareen et al. (2011) | USA | Cohort | Mood/Anxiety/Substance | Income decrease → RR=1.30 (1.06-1.60) for mood/anxiety/substance disorders |
| 33 | Sargent-Cox et al. (2011) | Australia | Cohort | Depression/Anxiety | Economic distress linked to depression/anxiety in older adults |
| 34 | Borges et al. (2011) | Portugal | Cross-sectional | Adolescent Health | Parental unemployment negatively impacts adolescent health perceptions |
| 35 | Barr et al. (2012) | England | Time-trend analysis | Suicide | Excess suicides in men: RR~1.036 (1.02-1.052) |
| 36 | Katikireddi et al. (2012) | England | Repeat cross-sectional | Psychological Distress | GHQ caseness in men: OR=1.53 (1.26-1.86) in 2009 vs 2008 |
| 37 | Gill et al. (2012) | Spain | Repeated cross-sectional | Depression | Major depression increased by 194% from pre-crisis period |
| 38 | Reeves et al. (2012) | USA | Ecological | Suicide | 1% unemployment rise → 0.59% increase in suicide rate |
| 39 | Berchick et al. (2012) | USA | Cohort | Depression | Job loss linked with depressive symptoms: coeff=0.333 (SE=0.108) |
| 40 | Butterworth et al. (2012) | Australia | Cohort | General Mental Health | 19.1% with poor mental health experienced subsequent unemployment |
| 41 | Bellis et al. (2012) | UK | Cross-sectional | Life Satisfaction | Most deprived: 17.1% low life satisfaction vs 8.9% most affluent |
| 42 | McLaughlin et al. (2012) | USA | Cohort | Depression | Foreclosure → IDR=2.4 (1.6-3.6) for major depression |
| 43 | Redonnet et al. (2012) | France | Cohort | Substance Use | Low SES linked with higher rates of tobacco (OR=2.11) and cannabis use |
| 44 | Sirvio et al. (2012) | Finland | Cohort | Psychological Distress | Precarious workers have more distress symptoms vs permanent workers |
| 45 | Chang et al. (2013) | 54 countries | Time-trend analysis | Suicide | Suicide rate in men: RR=1.033 (1.027-1.039) after 2008 crisis |
| 46 | Garcy & Vägerö (2013) | Sweden | Longitudinal Cohort | Suicide | Suicide mortality in men post-recession: HR=1.43 (1.31-1.56) |
| 47 | Vanderoost et al. (2013) | Belgium | Cross-sectional survey | Suicide | Employment loss → OR=8.8 (2-39.3) for suicidal thoughts |
| 48 | Bartoll et al. (2013) | Spain | Repeated cross-sectional | General Mental Health | Poor mental health in men: PR=1.15 (1.04-1.26) during crisis |
| 49 | De Vogli et al. (2013) | Italy | Ecological time-series | Mental Disorder Mortality | 1% unemployment increase → RR=1.074 (1.032-1.117) for mental disorder mortality |
| 50 | Modrek (2013) | USA | Longitudinal Industrial Cohort | Hypertension | High-layoff plant work → OR=1.6 (1.04-2.48) for hypertension |
| 51 | Zavras et al. (2013) | Greece | Repeated cross-sectional | Self-Rated Health | Self-reported good health deteriorated from 71% (2006) to 68.8% (2011) |
| 52 | Vandoros et al. (2013) | Greece/Poland | Repeated cross-sectional | General Health | Greece: OR=1.16 (1.04-1.29) for poor health vs control population |
| 53 | Hauksdottir et al. (2013) | Iceland | Cohort | Stress | High stress levels increased only among women during crisis |
| 54 | Gili et al. (2013) | Spain | Repeated cross-sectional | Depression | Risk of depression during crisis almost 3× higher than before |
| 55 | Bor et al. (2013) | USA | Cohort | Substance Use | Binge drinking increased from 4.8% (2006-07) to 5.1% (2008-09) |
| 56 | Lopez Bernal et al. (2013) | Spain | Ecological | Suicide | 8.0% increase in suicide rate above trend since financial crisis |
| 57 | Flint et al. (2013) | UK | Cohort | Psychological Distress | Mental distress among unemployed 2.20× (1.98-2.40) higher than employed |
| 58 | Eichhorn (2013) | 40 European societies | Ecological | Life Satisfaction | Unemployment lowers life satisfaction by 0.5-0.785 points |
| 59 | Evans-Lacko et al. (2013) | Europe (27 countries) | Repeated cross-sectional | General Mental Health | People with mental health problems more vulnerable to job loss: OR=1.12 (1.03-1.34) |
| 60 | Fountoulakis et al. (2013) | Greece | Ecological | Suicide | No correlation found between suicide rates and unemployment |
| 61 | Sauma et al. (2013) | England | Ecological | Suicide | Unemployment-suicide association significant at regional level only |
| 62 | Shin & Choi (2013) | South Korea | Ecological | Substance Use | 20× higher alcohol-attributable deaths in unemployed |
| 63 | Olesen et al. (2013) | Australia | Cohort | General Mental Health | Negative correlation (r=-0.16) between unemployment and mental health |
| 64 | Kan (2013) | Japan | Cohort | General Mental Health | Job loss decreases mental health by 12.0 points (MHI-5) |
| 65 | Pinto-Meza et al. (2013) | EU countries | Cross-sectional | Depression/Anxiety | Unemployed showed highest prevalence of mood/anxiety disorders |
| 66 | Snoradottir et al. (2013) | Iceland | Cross-sectional | Psychological Distress | Downsizing associated with increased psychological distress |
| 67 | Murphy et al. (2013) | USA | Cross-sectional | Substance Use | Housing instability associated with alcohol dependence symptoms |
| 68 | Fone et al. (2013) | Wales, UK | Cross-sectional | General Mental Health | Income inequality at regional level associated with poorer mental health |
| 69 | Saurina et al. (2013) | England | Longitudinal | Suicide | Unemployment increase → coeff=0.384 for male suicide in South West |
| 70 | Economou et al. (2013) | Greece; Greece | Repeated cross-sectional (Greece) | Depression/Suicide | Major depression odds greater in 2011 vs 2008: OR=10.0 (1.97-3.43) | Suicidal ideation increased from 5.2% (2009) to 6.7% (2011) |
| 71 | Minelli et al. (2014) | Italy | Longitudinal Panel | General Health | First-job seekers vs permanent workers: OR=0.65 for worse health |
| 72 | Iglesias García et al. (2014) | Spain | Ecological Time-Series | Mental Health Care Use | Unemployment rate negatively correlated with mental health care demand |
| 73 | Antonakakis & Collins (2014) | Greece | Time-Series | Suicide | 1% decrease in govt expenditure → semi-elasticity=-0.0043 for male suicide |
| 74 | Drydakis (2014) | Greece | Longitudinal panel | General Mental Health | Unemployment (2008-2013) → β=0.0318 for worse mental health |
| 75 | Korhonen et al. (2014) | Finland | Time Series Analysis | Suicide | Economic hardship → coeff=4.12 for suicide rate (1970-2010) |
| 76 | Ásgeirsdóttir et al. (2014) | Iceland | Population-based cohort | Suicide | Economic collapse → RR=0.85 (0.76-0.96) for male suicide attempts |
| 77 | Bartoll et al. (2014) | Spain | Repeated cross-sectional | General Mental Health | Poor mental health among men: PR=1.15 (1.04-1.26) during crisis |
| 78 | Blomqvist et al. (2014) | Sweden | Repeated cross-sectional | Psychological Distress | Mental distress increased among women, especially unemployed |
| 79 | Alameda-Palacios et al. (2014) | Spain | Ecological | Suicide | Suicide rates increased in young people (15-44) at 1.21% annually |
| 80 | Pompili et al. (2014) | Italy | Ecological | Suicide | Suicide rate for men in labor force increased 12% (2006-2010) |
| 81 | Coope et al. (2014) | England/Wales | Ecological | Suicide | Downward trend in male suicide rates stopped/reversed after 2008 |
| 82 | Reeves et al. (2014) | EU countries /Canada/USA | Ecological | Suicide | Suicide rose: EU +6.5%, Canada +4.5%, USA +4.8% |
| 83 | Breuer (2014) | 26 EU countries | Ecological | Suicide | 1% unemployment increase → 0.79% increase in suicide <65 years |
| 84 | Toffolutti & Suhrcke (2014) | 23 EU countries | Ecological | Suicide | 1% unemployment increase → 34.1% increase in suicide rates |
| 85 | Baumbach & Gulis (2014) | 8 EU countries | Ecological | Suicide | Suicide increases: Germany +5.3%, Poland +19.3% with unemployment rise |
| 86 | Moheenich-Enaghlou (2014) | USA | Ecological | Suicide | Positive correlation between unemployment and suicide in prime-age workers |
| 87 | Phillips & Nugent (2014) | USA | Ecological | Suicide | Strong positive association between unemployment and suicide rates |
| 88 | Cylus et al. (2014) | USA | Ecological | Suicide | 1% unemployment → 0.16 more suicide deaths per 100,000 |
| 89 | Chan et al. (2014) | South Korea | Ecological | Suicide | Unemployment rate positively associated with suicide rates |
| 90 | Madianos et al. (2014) | Greece | Ecological | Suicide | Suicide rates correlated with public debt/GDP and unemployment |
| 91 | Fountoulakis et al. (2014) | Hungary | Ecological | Suicide | Unemployment associated with suicidality after 3-5 year lag |
| 92 | Houle & Light (2014) | USA | Ecological | General Mental Health | Foreclosure rate contributed to increased suicides (b=0.04, p<0.1) |
| 93 | Mattei et al. (2014) | Italy | Ecological | General Mental Health | GDP decrease associated with male suicides due to financial problems |
| 94 | McKenzie et al. (2014) | New Zealand | Cohort | Psychological Wellbeing | Job loss decreased mental health by 1.34 points (SF-36) |
| 95 | Milner et al. (2014) | Australia | Cohort | Depression | Unemployed: -1.64 points mental health vs employed |
| 96 | Aslund et al. (2014) | Sweden | Cross-sectional | Substance Use | Unemployed: OR=2.11 (1.79-2.50) for poor psychological wellbeing |
| 97 | Riumallo-Herl et al. (2014) | EU countries /USA | Cohort | Suicide | Unemployment associated with 42% increase in depressive symptoms (USA) |
| 98 | Gfroerer et al. (2014) | USA | Repeated cross-sectional | Suicide | Unemployed show higher prevalence of substance use disorders |
| 99 | Miret et al. (2014) | Spain | Cross-sectional | Suicide | Unemployment associated with suicidal ideation in 18-49 year olds |
| 100 | Rhodes et al. (2014) | Canada | Cohort | Adolescent Health | Downward trend in adolescent suicidal behavior stopped after recession |
| 101 | Gassman-Pines et al. (2014) | USA | Repeated cross-sectional | Life Satisfaction | State job loss increased girls’ suicidal ideation and plans |
| 102 | Pförtner et al. (2014) | 31 countries | Cross-sectional | Depression | Ireland/Portugal: 9-17% rise in adolescent health complaints with unemployment |
| 103 | Klanšček et al. (2014) | Slovenia | Cross-sectional | Suicide | Low SES adolescents: 4× higher odds of low life satisfaction |
| 104 | Cagney et al. (2014) | USA | Cohort | Mental Health Care Use | Foreclosure → OR=1.75 (1.14-2.67) for depression in older adults |
| 105 | Córdoba-Doña et al. (2014) | Spain; Spain | Ecological time-series (Spain) | Suicide | 1% unemployment increase → 1.08 increase in suicide attempt rate | 8.6% more suicide attempts (2017 in men, 2972 in women) 2008-2012 |
| 106 | Modrek et al. (2015) | USA | Longitudinal Panel | Suicide | Post-2009 trend: β=0.0192 (0.0115-0.0269) for outpatient MH visits |
| 107 | Reeves et al. (2015) | 20 EU countries | Cross-national panel | Suicide | 1% male unemployment increase → 0.94% increase in male suicide |
| 108 | Branas et al. (2015) | Greece | Interrupted Time Series | Suicide | Austerity measures → 35.7% increase in total suicides |
| 109 | Rachiotis et al. (2015) | Greece | Ecological Study | Stress/General Mental Health | Austerity period (2011-2012) → RR=1.34 for total suicide rate |
| 110 | Norstrom & Gronqvist (2015) | 30 countries | Ecological | Mental Health Care Use | Unemployment detrimental to suicide, especially in less protected countries |
| 111 | Giorgi et al. (2015) | Italy | Cross-sectional | Suicide | Job stress mediates relationship between fear of crisis and mental health |
| 112 | Dunlap et al. (2016) | USA | Cross-sectional (NSDUH) | General Mental Health | County unemployment (Q4 vs Q1) → RR=0.58 (0.46-0.74) for MH service use |
| 113 | Ásgeirsdóttir et al. (2016) | Iceland | Population-based cohort | Mental Health Care Use | Economic collapse → RR=0.86 (0.79-0.92) for female suicide attempts |
| 114 | Nour et al. (2016) | Canada | Repeated cross-sectional | Depression | Austerity period → OR=1.26 (1.17-1.34) for poor mental health |
| 115 | Buffel et al. (2016) | Europe (27 countries) | Repeated cross-sectional | Depression | High unemployment → OR=1.031 for contacting GP for MH (employed men) |
| 116 | Sicras-Mainar & Navarro-Artieda (2016) | Spain | Retrospective observational | Mental Health Care Use | MDD prevalence increased 0.081 (0.074-0.088) during crisis |
| 117 | Lee et al. (2017) | Taiwan | Interrupted time series | Depression | Low-income men: 18% increase in depression hospitalizations post-2008 |
| 118 | Petrou (2017) | Cyprus | Interrupted time-series | Suicide | Co-payment introduction non-significant effect on MH service visits |
| 119 | Forbes & Krueger (2019) | USA | Longitudinal cohort | Suicide | Financial hardship → OR=1.3 (1.23-1.42) for depression symptoms |
| 120 | Elbogen et al. (2020) | USA | Longitudinal Cohort | Depression | Cumulative financial strain → OR=1.53 (1.32-1.77) for suicide attempt |
| 121 | Meda et al. (2022) | 175 countries | Ecological | Suicide | 1% unemployment increase → RR=1.03 (1.02-1.03) for male suicide (30-59) |
| 122 | Bracone et al. (2024) | Italy | Prospective cohort | Child Mental Health | High economic hardship → OR=1.84 (1.26-2.7) for depression increase |
Table 2.
Summary of key findings related to vulnerable population groups identified across the included studies.
Table 2.
Summary of key findings related to vulnerable population groups identified across the included studies.
| Group | Key Findings |
|---|---|
| Unemployed individuals |
Higher risk of depression, anxiety, distress, and suicide. Longer unemployment = worse mental health outcomes. |
| Precarious/Insecure workers |
Job insecurity and temporary work linked to mental distress. Fear of crisis worsened mental health among workers. |
| Individuals in debt / Financial hardship |
Debt and housing payment problems associated with depression and suicidal ideation. Low wealth linked to high psychological distress. |
| Families and children |
Parental unemployment negatively affected children’s mental health. Family economic stress mediated child psychological outcomes. |
| Adolescents and young adults |
Recession linked to increased psychological complaints and suicidal behaviors in adolescents. Parental job loss affected adolescent well-being. |
| Older adults |
Economic distress and foreclosure linked to depression in older adults. Financial insecurity worsened mental health in aging populations. |
| People with pre-existing mental illness |
More vulnerable to job loss during recession. Faced increased discrimination and isolation. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



