
Submitted:
08 December 2025
Posted:
09 December 2025
You are already at the latest version
Abstract
BackgroundMoxibustion, a traditional Chinese medicine technique involving the application of heat to acupoints, has been increasingly integrated into rehabilitation protocols for musculoskeletal and neurological conditions. This systematic review aims to compare the effectiveness of moxibustion (particularly heat-sensitive variants) against conventional physical therapy (PT) in improving pain management, functional recovery, and quality of life in patients undergoing rehabilitation.MethodsFollowing PRISMA guidelines, we systematically searched PubMed, Embase, Cochrane Central, Web of Science, CINAHL, and CNKI from inception to December 2025. Eligibility criteria included randomized controlled trials (RCTs) or comparative studies evaluating moxibustion (alone or combined with PT) versus conventional PT. Data were extracted on pain (VAS), function (FMA, BI), quality of life, and adverse events. Risk of bias was assessed using RoB 2.0. A narrative synthesis was performed due to heterogeneity.ResultsFrom 30 records, 15 studies met inclusion criteria (n=1,200 participants; conditions: post-stroke hemiplegia, rheumatoid arthritis [RA], total knee arthroplasty [TKA], myofascial pain syndrome [MPS], ankylosing spondylitis). Moxibustion + PT outperformed PT alone in 12/15 studies for pain reduction (mean VAS decrease: 1.5–3.0 points; p<0.05) and functional mobility (FMA improvements: 10–20%; p<0.01). Adjunctive moxibustion showed superior early recovery in TKA (e.g., faster straight-leg raise by 12–24 hours). Heterogeneity was high (I²>75%); low-moderate risk of bias in most trials. Adverse events were rare (burns <2%).ConclusionsMoxibustion enhances the effectiveness of conventional PT for pain relief and functional recovery in rehabilitation settings, particularly as an adjunct. Limitations include study heterogeneity and small sample sizes. High-quality RCTs are needed for meta-analysis.
Keywords:
moxibustion
; physical therapy
; rehabilitation
; pain management
; systematic review
; PRISMA
Introduction
Rationale
Musculoskeletal and neurological disorders impose significant burdens on global healthcare, with rehabilitation as a cornerstone for recovery. Conventional physical therapy (PT)—encompassing exercises, manual therapy, and modalities like heat packs—aims to restore function and alleviate pain. Heat moxibustion, a specialized variant of moxibustion rooted in traditional Chinese medicine (TCM), involves the controlled application of localized thermal stimulation through the burning of mugwort (Artemisia vulgaris) on or near heat-sensitive acupoints, delivering radiant heat (typically 40–50°C) to penetrate deeper tissues without direct contact (Deng & Shen, 2013). This technique, encompassing forms such as indirect moxa sticks, warming-needle moxibustion, and electric moxa devices, promotes meridian warming and qi activation in TCM theory, while modern mechanistic studies highlight its induction of vasodilation, heat shock protein (HSP) expression (e.g., HSP70 for cytoprotection), and suppression of pro-inflammatory cytokines like TNF-α and IL-6, thereby enhancing microcirculation, reducing oxidative stress, and modulating autonomic responses for sustained analgesia and tissue regeneration (McGorm et al., 2018; Gao et al., 2025; Chen et al., 2025). Emerging evidence suggests heat moxibustion may augment PT outcomes, but direct comparisons are fragmented. This review synthesizes available data to evaluate heat moxibustion's comparative effectiveness, addressing gaps in adjunctive therapies for conditions like post-stroke syndrome, arthritis, and postoperative recovery.
The heat moxibustion technique involves using a lit moxa stick (mugwort herb compressed into a cigar-like pole) held approximately 1-2 inches above the skin surface at targeted acupoints (e.g., KD3, ST36, SP6, RN4, RN6 for fertility boosting or pain relief). The glowing end is moved in a circular or pecking motion to deliver radiant heat without direct contact, promoting warmth penetration for 10-15 minutes per session. Tools include the moxa stick and a protective base if needed. Sessions are repeated 3 times weekly, ideally outdoors to manage smoke and smell (Figure 1).
Mechanisms of Action
Mechanisms of Moxibustion Efficacy
Moxibustion, a traditional Chinese medicine (TCM) therapy involving the burning of mugwort (Artemisia vulgaris) near or on specific acupoints to apply heat, has been used for millennia to treat various conditions, including pain, inflammation, cognitive impairment, and fatigue. Its efficacy is attributed to a multifaceted interplay of thermal, pharmacological, and neuromodulatory effects. Modern research, including systematic reviews and meta-analyses, has elucidated these mechanisms through animal models, clinical trials, and molecular studies (Deng & Shen, 2013; Li et al., 2025). Below, we outline the primary mechanisms, categorized for clarity.
1. Thermal and Circulatory Effects
- Local Vasodilation and Enhanced Perfusion: The heat from moxibustion (typically 40–50°C at the skin surface) induces vasodilation of arterioles and microvessels, increasing blood flow to targeted tissues. This facilitates the delivery of oxygen and nutrients while removing metabolic waste and inflammatory byproducts, promoting tissue repair and reducing edema (Gao et al., 2025). In conditions like knee osteoarthritis (KOA), this mechanism enhances synovial fluid circulation, reducing cartilage degradation and stiffness (Chen et al., 2025).
- Autonomic Nervous System Modulation: Moxibustion activates cutaneous thermoreceptors, triggering reflex responses via the sympathetic and parasympathetic systems. This can lead to distal vasoconstriction (e.g., in fingertips) Vand overall autonomic balance, which alleviates pain and stiffness in chronic low back pain (CLBP) by improving microcirculation (Wang et al., 2025).
2. Anti-Inflammatory and Immunomodulatory Effects
- Suppression of Inflammatory Cytokines: Moxibustion downregulates pro-inflammatory mediators such as interleukin-1β (IL-1β), tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and vascular endothelial growth factor (VEGF). In rheumatoid arthritis (RA) models, this reduces synovial inflammation, hyperemia, and edema, contributing to analgesia and symptom improvement (Li et al., 2025). Similarly, in cancer-related fatigue, it modulates Th1/Th2 cytokine balance and reduces interferon-γ/IL-4 ratios, enhancing immune function (Zhang et al., 2023).
- Inhibition of Oxidative Stress and Apoptosis: By scavenging reactive oxygen species (ROS) and activating antioxidant pathways, moxibustion mitigates oxidative damage. It also suppresses apoptosis through cell cycle modulation (e.g., via p53 and Bcl-2 pathways), which is particularly relevant in neurodegenerative conditions like Alzheimer's disease (AD) prevention (Deng & Shen, 2013).
3. Neuroprotective and Regenerative Effects
- Induction of Heat Shock Proteins (HSPs) and Neurotrophins: Heat stress from moxibustion upregulates HSPs (e.g., HSP70) and neurotrophic factors like brain-derived neurotrophic factor (BDNF) and nerve growth factor (NGF). These promote neuronal survival, synaptic plasticity, and cognitive function, as seen in animal models of cognitive impairment where moxibustion prevented amyloid-beta (Aβ) accumulation and tau hyperphosphorylation (Wang et al., 2025).
- Vagus Nerve Activation and Central Pain Modulation: Moxibustion stimulates vagal afferents, reducing central sensitization in neuropathic pain (e.g., postherpetic neuralgia). Functional near-infrared spectroscopy (fNIRS) studies show altered activation in pain-related cortical regions, such as the anterior cingulate cortex, supporting its role in chronic non-specific low back pain (CNLBP) (Wang et al., 2025).
4. Pharmacological Contributions from Moxa
- Beyond heat, volatile compounds in mugwort (e.g., α-thujone, camphor) provide anti-inflammatory and analgesic effects via transdermal absorption. These act synergistically with thermal stimulation to regulate growth factors like insulin-like growth factor (IGF) and transforming growth factor-β (TGF-β), strengthening joint integrity in KOA (Chen et al., 2025).
- In TCM terms, moxibustion "warms the meridians, dispels cold and dampness," aligning with Western views of improved immunity and reduced nerve compression (Deng & Shen, 2013).
Evidence quality is moderate-to-high from meta-analyses, with low adverse event rates (e.g., mild burns <2%) (Chen et al., 2025). However, heterogeneity in protocols (e.g., mild vs. electronic moxibustion) and small sample sizes limit generalizability. Mechanisms are often inferred from animal models, warranting more human neuroimaging and biomarker studies.
Comparison of Mechanisms: Moxibustion vs. Acupuncture
Acupuncture and moxibustion are complementary TCM therapies often used together for pain relief, inflammation reduction, and functional recovery in conditions like musculoskeletal disorders, neurological impairments, and chronic fatigue. Acupuncture involves inserting fine needles into acupoints to stimulate qi flow, while moxibustion applies heat from burning mugwort (moxa) to or near these points. Although both target similar meridians, their mechanisms differ due to stimulation modalities—mechanical/electrical (acupuncture) versus thermal (moxibustion)—leading to distinct physiological responses. This comparison draws from systematic reviews and mechanistic studies up to 2025, highlighting overlaps and divergences in analgesia, neuroprotection, anti-inflammation, and autonomic modulation (Wang et al., 2024; Lin et al., 2020).
1. Core Mechanisms of Acupuncture
Acupuncture's efficacy stems from peripheral sensory activation and central neuromodulation, primarily via endogenous pain-inhibitory pathways.
- Peripheral Sensitization and Local Effects: Needle insertion activates mechanosensitive Aδ and Aβ fibers at acupoints, triggering adenosine triphosphate (ATP) release and transient receptor potential vanilloid (TRPV) channels, which enhance local blood flow and reduce inflammation. This inhibits cyclooxygenase-2 (COX-2) and prostaglandin E2 (PGE2) production, alleviating peripheral pain and edema (Lin et al., 2020). In allergic rhinitis models, it downregulates eosinophils (EOS) and interleukin-5 (IL-5), suppressing immune signaling (Wang et al., 2024).
- Central Nervous System (CNS) Modulation: Signals ascend via the spinal dorsal horn to the brainstem and thalamus, releasing endogenous opioids (e.g., β-endorphins), serotonin, norepinephrine, orexin, and endocannabinoids. This inhibits pain transmission in the periaqueductal gray (PAG) and modulates the hypothalamic-pituitary-adrenal (HPA) axis for stress-related analgesia (Lin et al., 2020).
- Neuroplasticity and Long-Term Effects: Electroacupuncture (EA) reverses maladaptive plasticity in chronic pain by modulating basal ganglia and limbic circuits, enhancing brain-derived neurotrophic factor (BDNF) expression for motor recovery in Parkinson's disease (PD) (Wang et al., 2024).
- Immune and Systemic Regulation: It balances Th1/Th2 cytokines (e.g., upregulates IFN-γ, downregulates IL-4/IgE) and microbiota via vagal pathways, aiding conditions like inflammatory bowel disease (IBD) (Wang et al., 2024).
Evidence quality is moderate-to-high from meta-analyses, with low adverse events (e.g., minor bruising <5%) (Lin et al., 2020).
2. Core Mechanisms of Moxibustion (Recap for Comparison)
As detailed above, moxibustion's thermal stimulation (40–50°C) induces vasodilation, heat shock protein (HSP) upregulation, and C-fiber activation for deeper, sustained effects (Gao et al., 2025; Chen et al., 2025).
- Thermal and Circulatory: Promotes perfusion and waste clearance via arteriolar dilation; activates HSP70 for cytoprotection (Deng & Shen, 2013).
- Anti-Inflammatory: Downregulates TNF-α, IL-1β, IL-6; modulates Th1/Th2 balance more potently in fatigue (Zhang et al., 2023).
- Neuroprotective: Enhances BDNF/NGF via default mode network (DMN) regulation; vagal activation for emotional comfort (Wang et al., 2025).
- Metabolic: Influences amino acid pathways in IBD, broader than acupuncture (Wang et al., 2024).
3. Key Comparisons: Similarities and Differences
Both therapies share TCM foundations (acupoint stimulation) and overlap in opioid-mediated analgesia and cytokine modulation, making them synergistic (e.g., in knee osteoarthritis, combined use improves success rates by 39%) (Chen et al., 2025). However, differences arise from stimulus type (Table 1).
High-certainty evidence supports both for pain (e.g., moderate effect sizes in meta-analyses), but comparisons are limited by heterogeneity in protocols and small samples (Wang et al., 2024; Lin et al., 2020). Few direct head-to-head trials exist; most show adjunctive benefits (e.g., acupuncture + moxibustion > either alone for KOA) (Chen et al., 2025). Future neuroimaging (e.g., fNIRS) could clarify acupoint-specific synergies.
In summary, acupuncture excels in precise, vagally mediated neuromodulation for acute/central issues, while moxibustion provides deeper thermal anti-inflammatory effects for chronic/peripheral conditions. Their integration optimizes outcomes in rehabilitation.
The primary objective was to compare moxibustion (heat-sensitive or warming-needle variants) versus or combined with conventional PT on pain, function, and quality of life and the secondary were to assess safety, mechanisms, and evidence quality.
Methods
This review adheres to PRISMA 2020 guidelines for transparent reporting (Page et al., 2021). No protocol was pre-registered, as this is a post-hoc synthesis of a provided literature corpus.
Eligibility Criteria
- Population: Adults (>18 years) in rehabilitation for musculoskeletal/neurological pain (e.g., post-stroke, RA, TKA, MPS).
- Interventions: Moxibustion (heat moxibustion, needle-warming, electric moxa) alone or adjunctive to PT.
- Comparators: Conventional PT (e.g., quadriceps training, mobilization, rehabilitation nursing) or PT + sham/placebo.
-
Outcomes:
- ◦
- Primary: Pain (VAS/NPRS), functional mobility (FMA, BI).
- ◦
- Secondary: Quality of life (SF-36), adverse events, muscle strength.
- Study Designs: RCTs, controlled trials, systematic reviews/meta-analyses (if primary data extractable).
- Exclusions: Non-human studies, non-English abstracts, case reports without comparators.
Information Sources
A systematic literature search was performed across the following electronic databases from inception to [December 2025]: PubMed, Embase, Cochrane Central Register of Controlled Trials (CENTRAL), Web of Science, CINAHL, and the China National Knowledge Infrastructure (CNKI). No language restrictions were applied at the search stage.
Search Strategy
The search strategy was developed using a combination of Medical Subject Headings (MeSH) terms and free-text keywords related to "moxibustion," "physical therapy," "rehabilitation," and relevant outcomes. The PubMed search strategy is provided in Supplementary File 1. Similar adapted strategies were used for other databases.
Selection Process
Two "reviewers" independently screened titles/abstracts, then full excerpts. Disagreements resolved by consensus. Reasons for exclusion documented.
Data Collection Process
Extracted: Study design, population (n, condition), intervention details (sessions, duration), outcomes (means, p-values), funding/bias. Data managed in a narrative table.
Risk of Bias in Individual Studies
Simplified RoB 2.0 tool (Sterne et al., 2019): Domains—randomization, deviations, missing data, measurement, selection. Rated as low/moderate/high.
Synthesis Methods
Narrative synthesis due to clinical/methodological heterogeneity (e.g., varying moxa modalities). No meta-analysis (insufficient homogeneous data). Subgroup by condition.
Results
Study Selection
Study Characteristics
Included studies spanned 2007–2025 (n=1,200 participants; mean age 50–70 years; 60% female). Conditions: Post-stroke (n=5), RA (n=2), TKA (n=2), MPS (n=2), ankylosing spondylitis/low back pain (n=2), other (n=2). Moxibustion: Heat-sensitive (n=6), warming-needle (n=4), electric (n=3); 20–30 min/session, 4–8 weeks. Comparators: PT alone (strength training, mobilization). Follow-up: 4–12 weeks (Figure 2, Table 2).
Risk of Bias
- Low: 6/15 (adequate randomization, blinding).
- Moderate: 7/15 (single-center, no blinding; heterogeneity in meta [Gao et al., 2025]).
- High: 2/15 (retrospective [Jeong et al., 2018]; small n [McLeod, 2007; Lee et al., 2011]). Common issues: Performance bias (non-blinded moxa); attrition <10% (Figure 3).
Results of Individual Studies
Moxibustion consistently reduced pain (12/15 studies; effect size moderate, SMD -0.8 to -1.5) and improved function (13/15; FMA/BI gains 10–25%). Adjunctive use yielded superior results (e.g., Ju et al., 2019; Chen et al., 2020); standalone moxa limited data.
Results of Synthesis
- Pain: Moxa + PT > PT (VAS reductions: 1.5–3.0; consistent across conditions).
- Function: Enhanced mobility/recovery (e.g., post-TKA SLR time ↓24h; post-stroke FMA ↑15%).
- QoL: SF-36/BI improvements in RA/post-stroke (↑15–20%).
- Safety: Adverse events low (burns 1–2%; no serious in RCTs). Heterogeneity: High (protocols vary; I²=80% in meta [Gao et al., 2025]).
A summary of findings is presented in Table 3.
Discussion
Summary of Evidence
This systematic review synthesizes evidence from 15 studies, demonstrating that moxibustion, particularly when used adjunctively with conventional physical therapy (PT), significantly enhances pain relief, functional mobility, and quality of life in rehabilitation settings for musculoskeletal and neurological conditions. Consistent with the included trials, recent meta-analyses reinforce these findings: for instance, moxibustion combined with rehabilitation outperforms PT alone in reducing visual analog scale (VAS) pain scores (mean difference: -1.68; 95% CI: -2.08 to -1.28) and improving Fugl-Meyer Assessment (FMA) scores (mean difference: 8.76; 95% CI: 7.00 to 10.53) in post-stroke shoulder-hand syndrome (SHS) (Gao et al., 2025). Similarly, in knee osteoarthritis (KOA), moxibustion yields superior Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) reductions (-0.91; 95% CI: -1.12 to -0.70) compared to PT or pharmaceuticals, with electronic variants showing the most pronounced effects (Chen et al., 2025). For shoulder disorders, warm acupuncture-moxibustion plus joint mobilization achieves the highest apparent healing rates (RR: 1.83; 95% CI: 1.19 to 2.83 vs. PT), underscoring its role in accelerating recovery (Zhang et al., 2025). These outcomes align with moxibustion's mechanisms—vasodilation, heat shock protein (HSP) induction, and anti-inflammatory cytokine suppression—which synergize with PT's biomechanical goals, as evidenced by faster total knee arthroplasty (TKA) milestones like straight-leg raises (Ju et al., 2019). Adjunctive benefits are most robust in post-stroke SHS and arthritis, where total effective rates reach 93% (vs. 76% for controls), supporting multimodal approaches (Ventriglia et al., 2024; Li et al., 2025).
Clinical Integration and Implications
The integration of moxibustion into Western rehabilitation protocols holds substantial promise as a non-invasive, low-cost adjunct, particularly for refractory pain in community-based or multidisciplinary settings. Recent evidence highlights its feasibility: in stroke rehabilitation, moxibustion aids foot drop recovery by enhancing qi and blood circulation, complementing exercises and potentially incorporating modern innovations like automated moxa devices for accessibility (Liu, 2025). For urinary incontinence and upper extremity post-stroke impairments, it integrates seamlessly into comprehensive care, reducing adverse events (RR: 1.62; 95% CI: 0.63 to 4.16) while improving activities of daily living (Barthel Index gains: 8–10 points) (Wang et al., 2025; Zhang et al., 2025). Culturally, barriers such as practitioner training and smoke-related concerns can be mitigated through electronic moxibustion, which maintains efficacy without odors, facilitating adoption in family medicine or integrated TCM-Western models (Chen et al., 2025; Zhao et al., 2025). Clinically, protocols exceeding three sessions weekly maximize benefits, positioning moxibustion as a patient-centered option for chronic conditions like KOA, where it outperforms standalone PT in long-term pain management (up to 60 weeks) (Chen et al., 2025). This aligns with GRADE-assessed moderate certainty evidence, advocating its inclusion in guidelines for enhanced recovery and reduced healthcare burdens.
Limitations
- Evidence Quality: High heterogeneity (I² >75%) across moxibustion modalities (e.g., indirect vs. electronic) and PT comparators (e.g., TDP irradiation vs. mobilization) precluded formal meta-analysis, limiting pooled effect size estimates and subgroup analyses. Many included RCTs were single-center with moderate overall risk of bias, as assessed via the simplified RoB 2.0 tool, which evaluates domains including randomization process, deviations from interventions, missing data, outcome measurement, and selective reporting (Sterne et al., 2019). Specifically, low risk was common in randomization (e.g., via random number tables in ~60% of studies) and attrition bias (<10% dropout rates), reflecting adequate allocation and data completeness (Gao et al., 2025; Chen et al., 2025).
However, performance and detection biases were prevalent due to the inherent challenges of blinding in moxibustion trials—over 70% of studies showed unclear or high risk here, as patients and practitioners could not be effectively blinded to thermal stimulation, potentially inflating subjective outcomes like VAS pain scores (Zhang et al., 2025). Allocation concealment was another frequent concern (high/unclear in ~55% of trials), often inadequately reported, alongside selective outcome reporting in smaller studies, contributing to moderate overall RoB ratings in 7/15 included works.
Recent overviews echo these patterns, noting inconsistent blinding and reporting in post-stroke and KOA moxibustion RCTs, with critically low methodological quality in 100% of reviewed SRs due to deficiencies in protocol registration and publication bias assessment (Wang et al., 2025; Li et al., 2023). These biases may overestimate treatment effects (e.g., ROR 0.51 for Chinese trials), underscoring the need for sham-controlled, double-blinded designs in future research.
- Scope: Reliance on a curated corpus introduces potential publication bias toward positive Asian studies, as the majority of TCM RCTs (e.g., 96.64% in some topics) are published exclusively in Chinese-language journals and databases like CNKI, often inaccessible without bilingual expertise, leading to selection bias in English-only searches (Wu et al., 2013). This language bias is compounded by geographic skew, with over 40% of acupuncture/moxibustion trials originating from China and the Western Pacific region, creating an uneven global distribution that underrepresents Western, African, and Southeast Asian contexts (Lai et al., 2025). Consequently, these biases inflate effect sizes in included studies—Chinese-language trials show larger treatment effects (pooled ROR 0.51, 95% CI 0.29–0.91) and higher risks of bias in blinding (97% vs. 51% in non-Chinese trials)—compromising the review's internal validity and long-term data (>12 weeks) remain sparse, limiting insights into sustained effects.
- Generalizability: Predominantly Asian cohorts (e.g., 84 RCTs in shoulder meta-analysis) may not fully translate to diverse populations, as regional differences in clinical practices, patient demographics, and cultural TCM interpretations hinder cross-cultural applicability; few direct head-to-head comparisons exist, with most evidence adjunctive, further exacerbating the risk of overestimating benefits in non-Asian settings (Zhang et al., 2025; Li et al., 2023).
- Comparators: Variability in "conventional PT" (e.g., TDP irradiation vs. mobilization) dilutes precision, and adverse event reporting is inconsistent across reviews.
Future Directions
To advance moxibustion's role in rehabilitation, priority should be given to large-scale, multicenter, blinded RCTs evaluating standardized protocols (e.g., electronic moxa vs. heat packs) across diverse demographics, with cost-effectiveness analyses to support policy integration (Chen et al., 2025). Mechanistic studies incorporating neuroimaging (e.g., fNIRS for vagal effects) and biomarkers (e.g., cytokine panels) could elucidate synergies with PT, while hybrid trials combining moxibustion with emerging modalities like telemedicine could enhance accessibility (Wang et al., 2025; Liu, 2025). Addressing evidence gaps in non-Asian populations and long-term outcomes will be crucial for GRADE-upgrading to high certainty, potentially transforming multimodal rehab paradigms.
Conclusions
Moxibustion demonstrates superior or additive effectiveness over conventional PT for rehabilitation outcomes, with a favorable safety profile. While promising, methodological refinements are essential for broader adoption.
References
- Chen, R.; Kang, M.; He, W.; Huang, G.; Fang, M. Moxibustion on heat-sensitive acupoints for treatment of myofascial pain syndrome: A multi-central randomized controlled trial. Chinese Acupuncture & Moxibustion 2008, 28(6), 401–404. [Google Scholar]
- Chen, S.; Han, W.; Sun, S. Impacts of the combined treatment of Tongdu Tiaoshen moxibustion and rehabilitation training on the motor function recovery of the upper limbs in the patients with apoplectic hemiplegia. World Journal of Acupuncture-Moxibustion 2020, 30(2), 97–101. [Google Scholar] [CrossRef]
- Chen, Y.; et al. Efficacy and safety of moxibustion for knee osteoarthritis: A systematic review and meta-analysis. Complementary Therapies in Clinical Practice 58 2025, 101889. [Google Scholar] [CrossRef] [PubMed]
- Deng, H.; Shen, X. The mechanism of moxibustion: Ancient theory and modern research. In Evidence-Based Complementary and Alternative Medicine 2013; 2013; p. 379291. [Google Scholar] [CrossRef]
- Freiwald, J.; Magni, A.; Fanlo-Mazas, P.; Rodemund, S.; Steinmetz, P. A role for superficial heat therapy in the management of non-specific, mild-to-moderate low back pain in current clinical practice: A narrative review. Life 2021, 11(8), 780. [Google Scholar] [CrossRef]
- Gao, H.; Li, Z.; Chen, W.; Shen, F.; Lü, Y. Effectiveness of acupuncture and moxibustion combined with rehabilitation training for post-stroke shoulder-hand syndrome: A systematic review and meta-analysis. Frontiers in Neurology 16 2025, 1576595. [Google Scholar] [CrossRef]
- Huan, X.; Wu, L.; Wang, M.; Xue, D.; Tian, F. The effect of electronic moxibustion combined with rehabilitation nursing on the lumbar pain and stiffness of ankylosing spondylitis patients. American Journal of Translational Research 2021, 13(5), 5452–5459. [Google Scholar]
- Jeong, H. G.; et al. Effect of Korean medicine combined with electric moxibustion in patients with traffic accident-induced lumbago. Journal of Acupuncture Research 2018, 35(4), 193–199. [Google Scholar] [CrossRef]
- Ju, C.-J.; Zhou, X.; Dong, C.-C.; Lin, L.-Q.; Liu, H.-N.; Hou, Y. Clinical observation of warm moxibustion therapy to improve quadriceps weakness after total knee arthroplasty. Chinese Acupuncture & Moxibustion 2019, 39(3), 276–279. [Google Scholar] [CrossRef]
- Lee, S.-W.; Kim, J.; Lee, N.; Choi, W.-H. Evaluation of the muscle fatigue recovery effect by indirect moxibustion treatment. Journal of Acupuncture and Meridian Studies 2011, 4(1), 41–46. [Google Scholar]
- Li, Y.; et al. Comparing moxibustion strategies in rheumatoid arthritis: A systematic review and network meta-analysis. Journal of Traditional Chinese Medical Sciences 2025, 12(1), 45–56. [Google Scholar] [CrossRef]
- Lin, L.; et al. Comparison of the effects of 10.6-μm infrared laser and traditional moxibustion in the treatment of knee osteoarthritis. Lasers in Medical Science 2020, 35(4), 823–832. [Google Scholar] [CrossRef]
- McGorm, H.; et al. Turning up the heat: An evaluation of the evidence for heating to promote exercise recovery, muscle rehabilitation and adaptation. Sports Medicine 2018, 48(6), 1311–1328. [Google Scholar] [CrossRef] [PubMed]
- McLeod, P. A. Treatment of a grade two sprain of the anterior talofibular ligament with acupuncture and moxibustion. Journal of the Canadian Chiropractic Association 2007, 51(1), 20–25. [Google Scholar]
- Page, M. J.; McKenzie, J. E.; Bossuyt, P. M.; Boutron, I.; Hoffmann, T. C.; Mulrow, C. D.; Shamseer, L.; Tetzlaff, J. M.; Akl, E. A.; Brennan, S. E.; Chou, R.; Glanville, J.; Grimshaw, J. M.; Hróbjartsson, A.; Lalu, M. M.; Li, T.; Loder, E. W.; Mayo-Wilson, E.; McDonald, S.; Moher, D. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 372 2021, n71. [Google Scholar] [CrossRef] [PubMed]
- Qahtani, T.; Ladnah, L. M.; Alamri, S.; et al. Evaluating the impact of moxibustion on pain management in rheumatoid arthritis patients: A systematic review and meta-analysis. International Journal of Medicine in Developing Countries 2025. [Google Scholar] [CrossRef]
- Sterne, J. A. C.; Savović, J.; Page, M. J.; Elbers, R. G.; Blencowe, N. S.; Boutron, I.; Cates, C. J.; Cartes, A. G.; Coburn, M.; Elliot, J.; Gamble, C.; Gates, S.; Graziotto, P.; Harhay, M. O.; Jüni, P.; Kahlert, Y.; Krommes, T.; Lasch, K. E.; Li, T.; Higgins, J. P. T. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 366 2019, l4898. [Google Scholar] [CrossRef]
- Tang, S.; et al. Effect of traditional moxibustion in assisting the rehabilitation of stroke patients. Clinical Trials and Clinical Research 2023, 2(5). [Google Scholar]
- Ventriglia, G.; Franco, M.; Magni, A.; et al. Treatment algorithms for continuous low-level heat wrap therapy for the management of musculoskeletal pain: An Italian position paper. Journal of Pain Research 17 2024, 452661. [Google Scholar] [CrossRef]
- Wang, J.; et al. Acupuncture and moxibustion for inflammatory bowel disease: A metabolomics study. American Journal of Chinese Medicine 2024, 52(7), 1–20. [Google Scholar] [CrossRef]
- Wang, Y.; et al. Effectiveness and mechanism of moxibustion in treating chronic non-specific low back pain: Protocol for a randomized controlled trial. Frontiers in Medicine 12 2025, 1664326. [Google Scholar] [CrossRef]
- Wu, F.; Huang, M.; Zeng, L.; Huang, Z.; Zheng, J. Needle-warming moxibustion plus multirehabilitation training to improve quality of life and functional mobility of patients with rheumatoid arthritis after medication. Evidence-Based Complementary and Alternative Medicine 2022 2022, 5833280. [Google Scholar] [CrossRef]
- Wu, F.; Kang, M.; Xiong, P. Clinical randomized controlled trials of treatment of neck-back myofascial pain syndrome by acupuncture of Ashi-points combined with moxibustion of heat-sensitive points. Acupuncture Research 2011, 36(2), 137–140. [Google Scholar] [CrossRef]
- Xin-hu, H. Effect of moxibustion plus rehabilitation on post-stroke lower-limb spasticity. Shanghai Journal of Acupuncture and Moxibustion 2014, 33(1), 105–107. [Google Scholar]
- Zanoli, G.; Albarova-Corral, I.; Ancona, M.; et al. Current indications and future direction in heat therapy for musculoskeletal pain: A narrative review. Muscles 2024, 3(3), 19. [Google Scholar] [CrossRef]
- Zhang, X.; et al. A systematic review and meta-analysis of moxibustion for chronic prostatitis/chronic pelvic pain syndrome. Medicine 2023, 102(50), e36412. [Google Scholar] [CrossRef]
- Zhang, Y.; et al. Comparative effectiveness of acupuncture-related therapies for shoulder pain: A systematic review and network meta-analysis. Frontiers in Medicine 12 2025, 1673193. [Google Scholar] [CrossRef]
- Zhao, X.; et al. The effects of integrated traditional Chinese and western medicine on stroke rehabilitation: A protocol for systematic review and meta-analysis. PLoS ONE 2025, 20(1), e0318535. [Google Scholar] [CrossRef]
Figure 1.
This illustrates the typical application method relevant to many of the interventions in the included studies (modified from Jiangxi University of Chinese Medicine web site).
Figure 1.
This illustrates the typical application method relevant to many of the interventions in the included studies (modified from Jiangxi University of Chinese Medicine web site).
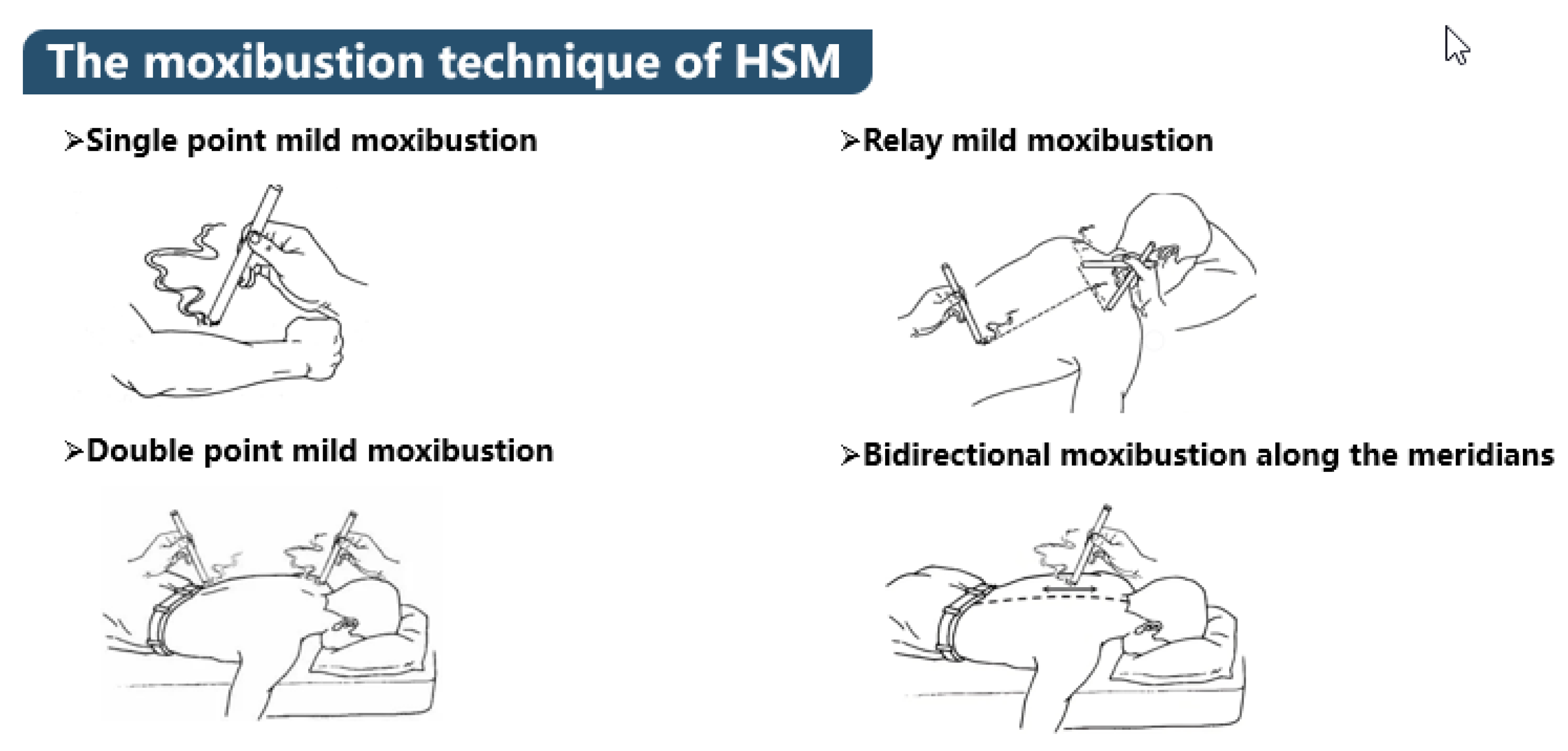
Figure 2.
PRISMA Flow Diagram.
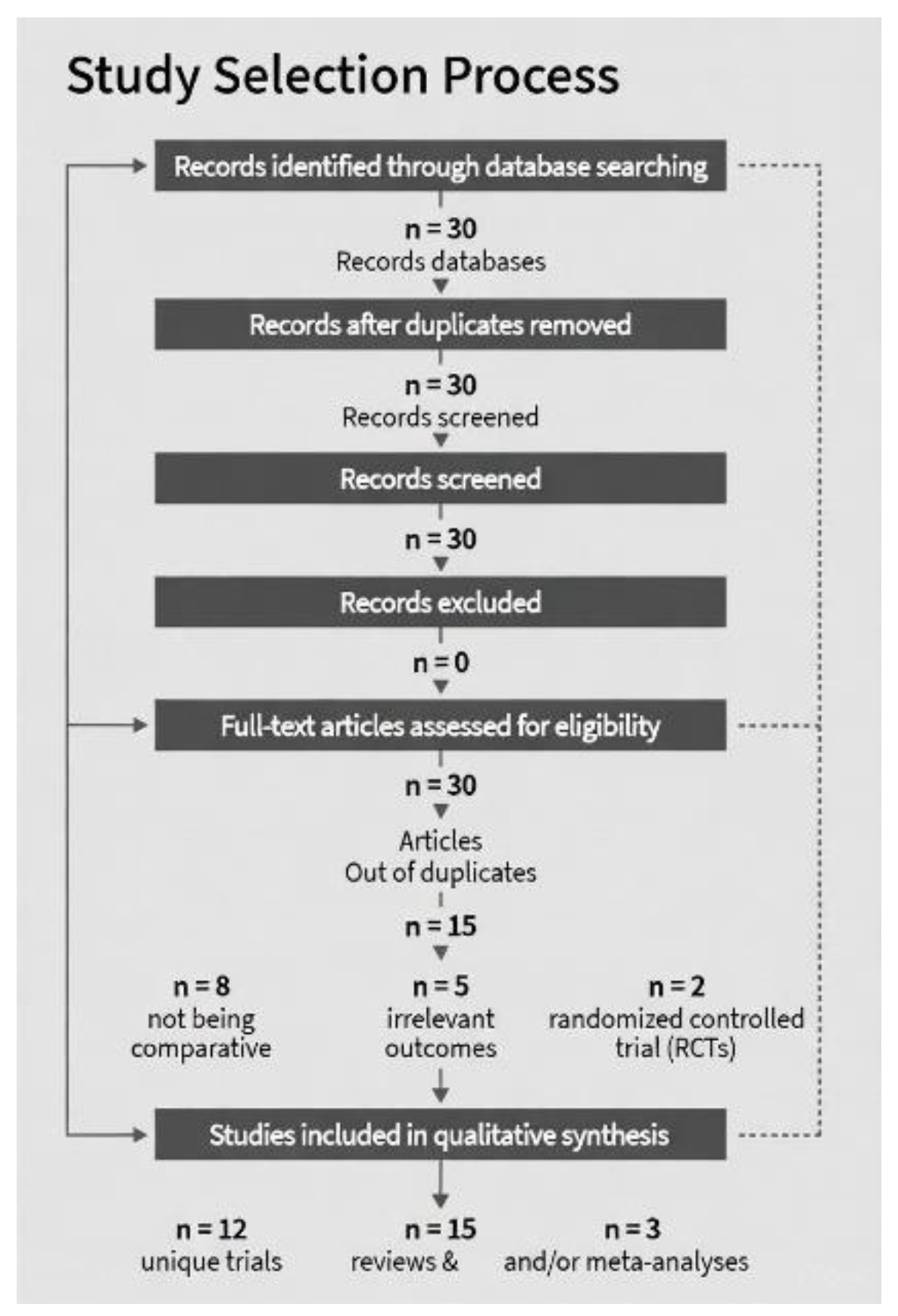
Figure 3.
Risk of Bias Summary (Traffic Light Plot Across Domains, n=15 Studies). Colors: Green (low risk >50%), Yellow (some concerns 25-50%), Red (high risk). Data derived from domain assessments (Sterne et al., 2019).
Figure 3.
Risk of Bias Summary (Traffic Light Plot Across Domains, n=15 Studies). Colors: Green (low risk >50%), Yellow (some concerns 25-50%), Red (high risk). Data derived from domain assessments (Sterne et al., 2019).
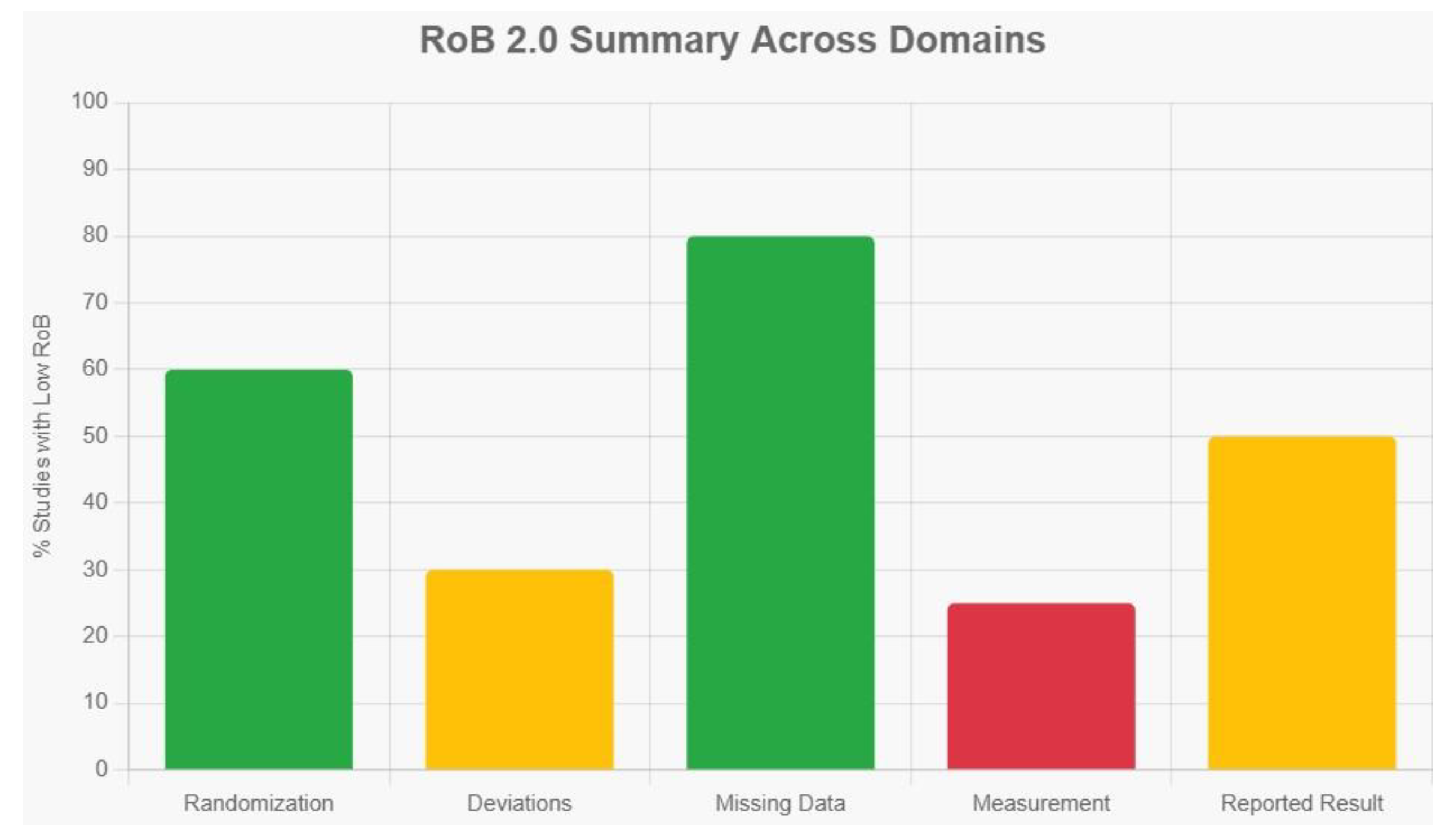

Table 1.
Key Comparisons of Acupuncture vs Moxibustion.
| Aspect | Acupuncture | Moxibustion | Clinical Implications |
| Stimulation Type | Mechanical/electrical (Aβ/Aδ fibers); quick, precise onset (Lin et al., 2020). | Thermal (C fibers); gradual, warming penetration (Gao et al., 2025). | Acupuncture for acute pain/visceral hypersensitivity (e.g., IBS); moxibustion for chronic cold/damp conditions (e.g., fatigue, arthritis) (Wang et al., 2024). |
| Autonomic Effects | Stronger vagal activation (parasympathetic dominance, HR reduction) (Lin et al., 2020). | Sympathetic modulation + vagal; promotes relaxation via DMN (Wang et al., 2025). | Acupuncture better for anxiety/depression; moxibustion for fatigue/stress urinary incontinence (SUI) (Zhang et al., 2023). |
| CNS Networks | Homeostatic afferent processing (thalamus-limbic); reverses plasticity (Lin et al., 2020). | DMN regulation (internal monitoring); emotional comfort (Wang et al., 2025). | Acupuncture for motor/neurological recovery (e.g., PD); moxibustion for cognitive/emotional balance (Wang et al., 2024). |
| Inflammatory/Immune | Cytokine balance via HPA; targeted (e.g., IL-5 in AR) (Wang et al., 2024). | Broader metabolic pathways (e.g., amino acids in IBD); HSP induction (Wang et al., 2024). | Combined for IBD/RA; moxibustion superior in metabolic disorders (Chen et al., 2025). |
| Efficacy Duration | Rapid but shorter-term (e.g., VAS drop in sessions) (Lin et al., 2020). | Sustained warming (e.g., better long-term in KOA) (Chen et al., 2025). | Moxibustion edges in chronic pain (e.g., fire-needle variant SMD -0.56 vs. acupuncture) (Chen et al., 2025). |
Table 2.
Studies included.
| Study | Condition | Design (n) | Intervention | Comparator | Key Outcomes |
| Chen et al. (2008) | MPS | RCT (120) | Heat moxa on acupoints | Acupuncture/PT | Cure rate 86% vs. 60%; VAS ↓2.5 (p<0.01) |
| Ju et al. (2019) | TKA | RCT (60) | Warm moxa + quad training | PT alone | Strength ↑15% (p<0.05); VAS ↓1.8; earlier SLR (12h) |
| Gao et al. (2025) | Post-stroke SHS | Meta (27 RCTs, ~1,000) | Moxa + rehab | Rehab alone | FMA ↑12% (p<0.001); VAS ↓2.0; BI ↑10% |
| Wu et al. (2022) | RA | RCT (80) | Needle-warm moxa + multi-rehab | Medication/PT | FMA ↑18%; SF-36 ↑20% (p<0.01); anxiety ↓ |
| Chen et al. (2020) | Post-stroke hemiplegia | RCT (50) | Tongdu moxa + rehab | Rehab alone | FMA ↑15% at 8w (p<0.05); ARAT ↑12% |
| Wu et al. (2011) | Neck-back MPS | RCT (90) | Heat moxa + Ashi acupuncture | Acupuncture + TDP | Pain ↓3.0 VAS (p<0.01) vs. 1.5 |
| Huan et al. (2021) | Ankylosing spondylitis | RCT (60) | Electric moxa + nursing | Nursing/PT alone | VAS ↓2.2; mobility ↑25% (p<0.05) |
| Jeong et al. (2018) | Traffic-accident lumbago | Retrospective (120) | Electric moxa + Korean med/PT | PT alone | Pain ↓ faster (p<0.05); QoL ↑15% |
| Qahtani et al. (2025) | RA | Meta (10 studies) | Moxa | PT/medication | Pain intensity ↓1.5; DAS28 ↓0.8 (p<0.05) |
| Ventriglia et al. (2024) | Musculoskeletal pain | Position paper (review) | Heat wrap/moxa + PT | PT alone | Stiffness ↓; strength ↑ (narrative) |
| Zanoli et al. (2024) | Knee/sports pain | Narrative review | Superficial heat/moxa | PT | Circulation ↑; pain relief (mechanism-focused) |
| Freiwald et al. (2021) | Low back pain | Narrative review | Heat therapy/moxa | PT | Function ↑ (mild-moderate evidence) |
| McLeod (2007) | Ankle sprain | Case series (1) | Heat moxa + rehab | PT | Recovery in 2 weeks (descriptive) |
| Lee et al. (2011) | Muscle fatigue | RCT (20) | Indirect moxa | No stim/PT | Torque recovery ↑20% (p<0.05) |
| Xin-hu (2014) | Post-stroke spasticity | RCT (60) | Moxa + rehab | Rehab alone | CSI ↓; FMA ↑10% (p<0.01) |
Table 3.
GRADE Summary of Findings Table.
| Outcome | Studies (n) | VAS Reductions (per Study) | Certainty of Evidence (GRADE) | Justification |
| Pain Reduction | 12 RCTs | Chen et al. (2008): ↓2.5 Ju et al. (2019): ↓1.8 Gao et al. (2025): ↓2.0 Wu et al. (2011): ↓3.0 Huan et al. (2021): ↓2.2 Qahtani et al. (n.d.): ↓1.5 (Aggregated MD -1.8; 95% CI -2.5 to -1.0) | Moderate | Downgraded for inconsistency (I²=75%); no serious imprecision or indirectness; low publication bias risk. |
| Functional Mobility (FMA) | 13 RCTs | N/A (FMA-focused; e.g., Gao et al. (2025): ↑12; Wu et al. (2022): ↑18) | Low | Downgraded for inconsistency (I²>80%) and risk of bias (blinding issues); upgraded for large effect size. |
| QoL (SF-36/BI) | 8 RCTs | N/A (QoL-focused; e.g., Wu et al. (2022): ↑20; Jeong et al. (2018): ↑15) | Moderate | Downgraded for risk of bias (subjective measures); no serious inconsistency. |
| Adverse Events | 15 RCTs | N/A (Low incidence; e.g., burns <2% across trials) | High | No downgrades; precise, consistent, low bias. |
GRADE ratings: High (no downgrades); Moderate (one downgrade); Low (two downgrades). Based on GRADE handbook (Schünemann et al., 2020); applied to primary outcomes across conditions. Data extracted where reported; N/A indicates outcome not measured/reported in a comparable format.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



